Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
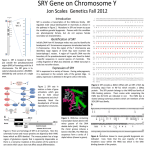
0021-972X/05/$15.00/0 Printed in U.S.A. The Journal of Clinical Endocrinology & Metabolism 90(4):2429 –2435 Copyright © 2005 by The Endocrine Society doi: 10.1210/jc.2004-1110 CLINICAL CASE SEMINAR Three New Novel Point Mutations Localized within and Downstream of High-Mobility Group-box Region in SRY Gene in Three Indian Females with Turner Syndrome Mohammed Shahid, Varinderpal S. Dhillon, Mohammed Aslam, and S. A. Husain Human Genetics Lab (M.S., M.A., S.A.H.), Department of Biosciences, Jamia Millia Islamia, New Delhi 110 025, India; and Commonwealth Scientific and Industrial Research Organization Health Sciences and Nutrition (V.S.D.), Adelaide, Adelaide 5000, Australia Point mutations and deletions in the SRY gene result in XY sex reversal in pure gonadal dysgenesis. To date, a majority of these affect the high-mobility group (HMG) domain of SRY, which plays a key role in its DNA binding activity. We carried out molecular genetics studies in three Turner syndrome patients all presenting with 45,X/46,XY mosaic karyotype. Case 1 demonstrated an insertion of T (thymine) within helix I of HMG box leading to frame shift mutation (N82X). In case 2, insertion of A (adenine) downstream of HMG box resulted in a nonsense frame shift mutation (L159fsX167). These mutations resulted in truncated and altered proteins. In case 3, D URING MAMMALIAN EMBRYOGENESIS, the presence of the SRY gene determines whether the gonads develop as testes, which in turn determines whether the embryo will develop as a male; in its absence, the fetal gonads will develop as ovaries (1). XY gonadal dysgenesis results from an embryogenic testicular regression sequence and can occur in a pure or partial form. Gonadal histology presents with hypoplastic testicular tubules intermixed with ovarian stroma (2). These individuals may have unilateral or bilateral dysgenetic gonads and/or streak gonads. Several genetic loci may play important roles in testis-determining pathways. Male-to-female reversal in 46,XY patients results in failure to develop testis. This could be attributed to the mutations in the SRY gene (3). Sex determination in humans depends on the action of a testis-determining factor encoded by the SRY gene consisting of a single exon. It is located on the short arm of Y chromosome and encodes a protein of 204 amino acids. The human Y chromosome is reported to have about 76 protein-coding genes, although only 27 distinct proteins have been identified thus far. Earlier thought to be a genetic wasteland, the Y chromosome is now found to have expanded its repertoire during the course of evolution by seFirst Published Online February 1, 2005 Abbreviations: ASO, Allele-specific oligonucleotide; F, forward; HMG, high-mobility group; R, reverse; SSCP, single-stranded conformational polymorphism. JCEM is published monthly by The Endocrine Society (http://www. endo-society.org), the foremost professional society serving the endocrine community. G>C missense mutation is found at codon 74 within helix I of HMG box (Q74H). No other mutations were found in the SRY gene of these patients. An allele-specific oligonucleotide study further confirmed that these variants are not common polymorphisms. To our knowledge, this is the first time these mutations are described at these codons resulting in mutated SRY proteins. Lack of a second sex chromosome in a majority of cells [mosaic karyotype and mutation(s) in the SRY gene] in these patients may have triggered the short stature. (J Clin Endocrinol Metab 90: 2429 –2435, 2005) quence amplification and selectively importing genes from autosomes and X chromosomes. This presents evolutionary conserved DNA-binding domain [the high mobility group (HMG) box], suggesting this protein regulates gene expression. SRY gene is essential for initiating testis development and differentiation of indifferent and bipotential gonads into testicular pathway (3, 4). In SRY presence, supporting cells of indifferent gonads become testicular Sertoli cells, whereas in its absence, these become ovarian follicular cells (5). SRY protein has been shown to possess sequence-specific DNAbinding activity and is assumed to regulate other genes involved in male determination pathways (6). Normal SRY changes the architecture of DNA, thus allowing access of other factors needed for its expression (7). This protein binds to target DNA sequences and facilitates DNA bending and hence acts as the main regulatory activity of the SRY gene (8). Mutations in the SRY gene have been found to account for approximately 15% of cases with gonadal dysgenesis (9 –12). However, a majority of these patients may have mutations in other genes involved in sex-differentiation pathway or in the regulatory elements of the SRY gene. To date 44 mutations have been identified within the open reading frame of the SRY gene, and most are located within the HMG box, thus highlighting the critical role of this domain (11, 13, 14). Of these, only 10 mutations outside the HMG box [eight are located in the 5⬘ region upstream of the HMG box, and the remaining two lie downstream, 3⬘ of the HMG box] have been reported so far (14, 15). There is one interesting report describing the mutations in the SRY gene occurring in two of three subjects with the 45,X/46,XY karyotype, one with 2429 2430 J Clin Endocrinol Metab, April 2005, 90(4):2429 –2435 cytogenetically normal Y chromosome and the other with a Y-derived marker chromosome. An identical missense mutation (G2128A, Ser18Asn) upstream of the HMG box of the gene has been found in two patients (16). Turner syndrome is characterized by short stature, gonadal dysgenesis, and dysmorphic features, including neck webbing (17). Almost half of all cases have typical Turner syndrome karyotype (45,X), whereas the remaining cases have either a derivative sex chromosome in the investigated cells or a mosaic karyotype, with the second cell line having a normal or structurally rearranged sex chromosome (18). Various studies have revealed either a normal or derivative Y chromosome in a high proportion of cases with clinical phenotype of Turner syndrome (19, 20). Turner syndrome with a mosaic 45,X/46,XY karyotype comprises a phenotypic spectrum of females (10 –15%) having SRY mutations. Here we describe three novel point mutations in the SRY gene in three Turner syndrome patients. To our knowledge, no mutations at these positions have been reported previously in the literature. Subjects and Methods Informed consent was obtained from all patients and control individuals. This study was approved by the ethics committee of the hospital and university. Subjects Cases 1 and 2. Patients 1 and 2, 24- and 20-yr-old females, respectively, born to healthy but unrelated parents, were referred because of primary amenorrhea. Physical examination revealed a height of 135 and 146.5 cm, respectively (below the fifth percentile). External genitalia were unambiguous female type. Histological investigations revealed white fibrous stromal tissue (with some similarities to testicular histopathology) in streak gonads. Both patients have multiple Turner stigmata (i.e. webbed neck, high arched palate, cubitus valgus, broad shield-like chest with widely spaced nipples, low hairline, disproportionately short legs, presence of müllerian structures, sexual infantilism at puberty, hypertension, and glucose intolerance). Scoliosis, nail dysplasia, and ear anomalies were also found in these patients. Endocrinological studies demonstrated hypergonadotropic hypogonadism (estradiol ⬍ 13.0 pg/ml; LH 32.3 and 26.4 mIU/ml; FSH 56.7 and 48.8 mIU/ml, respectively) as well as normal female concentrations of testosterone and androstenedione. Both suffer from psychological problems and primary amenorrhea. Axillary and pubic hairs were scanty. Case 1 has a blood karyotype as 45,X(80%)/46,XY (20%), whereas case 2 has 45,X (86%)/46,XY (14%) karyotype. Case 3. The proposita presented at 22 yr of age with short stature, ambiguous external genitalia [a birth defect in which the outer genitals do not have typical appearance of either sex] and absence of pubertal development. Clinical examination revealed a height of 151 cm (below the fifth percentile) and multiple Turner stigmata (i.e. micrognathia, low-set ears, high-arched palate, short and webbed neck, bilateral cubitus valgus, and multiple nevi). Sparse axillary and pubic hairs (Tanner stage II) were observed, and there was no clitoromegaly. On arousal, phallus length increased from 20 to 30 mm. The position of urinary meatus lies just beneath the phallus. Sonographic examination revealed a normal-sized uterus with a thin endometrium, bilateral müllerian derivatives, and right intraabdominal testis. Endocrinological studies demonstrated hypergonadotropic hypogonadism (estradiol ⬍ 13.0 pg/ ml; LH 32.5 mIU/ml; FSH 74.2 mIU/ml) as well as normal female concentrations of testosterone and androstenedione. Ovaries were not visible, but thickened structures resembling streak gonads were found on both sides of the uterus. Histological investigations revealed fibrous stromal tissue. No gonadoblastoma and dysgerminomas were found in the streak gonads. She had no psychological problems. Blood karyotype was 45,X (89%)/46,XY (11%). Shahid et al. • SRY Mutations and Turner Syndrome Extraction of DNA Genomic DNA from the blood samples was extracted by digestion with proteinase K (Boehringer, Mannheim, Germany) followed by routine phenol chloroform isolation and precipitation with ethanol or isopropanol with chilled 3 m sodium acetate (pH 5.2). Vacuum-dried DNA samples were dissolved in Tris-EDTA, and DNA concentration was measured by gel electrophoresis method. All reagents used in the DNA isolation were procured from E. Merck India Ltd. (Mumbai, India). PCR Complete SRY exon was studied by overlapping primers; however, only the relevant primers (which helped to identify these mutations) were discussed. The following primer sets were used to amplify fragments of 254 and 351 bp, respectively, from the open reading frame of the SRY gene (17): forward (F)1, 5⬘-CATGAACGCATTCATCGTGTGGTC-3⬘; reverse (R)1, 5⬘-CTGCGGGAAGCAAACTGCAATTCTT-3⬘; F2, 5⬘-CAGTGTGAAACGGGAGAAAACAGT-3⬘; and R2, 5⬘-GTTGTCCAGTTGCACTTCG CTGCA-3⬘. Exon 5 of p53 gene was amplified as internal control using oligonucleotide primers 5⬘-TACTCCCCTGCCCTAACAA-3⬘ (sense) and R, 5⬘-CATCGCTATC TGAGCAGCGC-3⬘ (antisense) to amplify the 184-bp PCR product. PCR amplification was performed in 25 l reaction volume containing 10 mm Tris HCl (pH 8.4), 50 mm KCl, 1.5 mm MgCl2, 200 m each of deoxynucleotide triphosphates (dATP, dCTP, dGTP, dTTP), 5 pmol oligonucleotides primers, 100 g DNA and 0.5 U Taq DNA polymerase (Perkin-Elmer Cetus, Norwalk, CT). PCR was performed as follows: 4 min at 95 C followed by 35 cycles at 95 C for 30 sec; 55 C for 30 sec; 72 C for 30 sec, and a final extension step of 72 C for 7 min. Every PCR included negative (normal XX female) and positive (normal XY male) controls. PCR products (7 l) were run on 2% agarose gels, and bands were visualized by ethidium bromide staining on an UV transilluminator. For all agarose gels, a 100-bp ladder was used as size standard. Allele-specific oligonucleotide (ASO) hybridization With primers F2 and R2 as described above, a 351-bp segment of SRY (including the mutation sites) was amplified from the DNA of the patients and 44 randomly selected normal XY males. The 351-bp SRY PCR products were then arrayed on two identical nylon membranes. Oligonucleotides were designed and synthesized for use as probes in this study: one specific for wild-type SRY (5⬘-tctcgcgatcagaggcgcaagatggc-3⬘) and the other specific for Q74H SRY (5⬘-tctcgcgatcacaggcgcaagatggc-3⬘), differing only at the 12th nucleotide: wild-type (5⬘-atggctctagagaatcccagaatgcg-3⬘) and N82X SRY (5⬘-atggctctagagtaatcccagaatgc-3⬘) differing in having additional “t” at the 13th nucleotide and wild-type SRY (5⬘-agcgaagtgcaactggacaacagg-3⬘) and L159fsX167 SRY (5⬘-agcgaagtgcaaactggacaacagg-3⬘) differing in an additional “a” at the 13th nucleotide position. Twenty-five nanograms of these oligonucleotides were end labeled with ␥-32P by T4 polynucleotide kinase (Fermentas Inc., Hanover, MD) and used separately to probe the duplicate membranes for 16 h at 65 C. The membranes were subsequently washed and exposed to film at ⫺80 C. Hybridizations were done separately with each category of wild-type and mutant oligonucleotides. Single-stranded conformational polymorphism (SSCP) PCR products were labeled with (␣-P32) dCTP by performing 15 additional cycles of PCR and loaded on 6% nondenaturing polyacrylamide gel containing 5% glycerol. The electrophoresis was carried out overnight at 200 V at 17 ⫾ 1 C. The dried gel was exposed to x-ray film for 48 h at ⫺70 C (21). Automated DNA sequencing PCR products were purified using QIAquick PCR purification kit (QIAGEN, Santa Clarita, CA) before being sequenced using an ABI Prism 310 automated sequencer (Applied Biosystems, Foster City, CA). The cycle sequencing of the purified PCR products was performed using BIG Dye terminator sequencing ready reaction mix with AmpliTaq DNA polymerase FS on GeneAmp PCR 9700 (Applied Biosystems). PCR conditions were set as: 96 C ⫻ 10 sec, 56 C ⫻ 5 sec and 60 C ⫻ 4 min for 25 cycles. After cycle sequencing, extension products were purified to Shahid et al. • SRY Mutations and Turner Syndrome remove any unincorporated dye-labeled terminators using ethanol/ sodium acetate precipitation method. Template suppressor reagent was added, and samples were heat denatured, chilled on ice, and loaded on the Prism 310 sequencer. The sequences were analyzed using sequencing analysis software 3.4.1 on a Mac OS 9.1 (Applied Biosystems). Results Chromosome analysis from cultured peripheral blood lymphocytes showed mosaic karyotype (45,X/46,XY). Biochemical parameters showed altered levels of estradiol, LH, and FSH, but normal female concentrations of testosterone and androstenedione. These patients showed altered migration of PCR products in SSCP assay (Fig. 1). In reference to SRY mutations, patient 1 has an insertion of T (thymine) leading to frame shift within the open reading frame inside highly conserved DNA-binding motif-HMG box (N82X; Figs. 2, A and B, and 3, A and B), and the mutated protein lacks the last 123 amino acid residues. The father and other male members of the family did not consent to DNA analysis, but some are already parents of healthy children. Patient 2 showed insertion of A (adenine) leading to frame shift mutation downstream of the HMG box, resulting in an altered protein at the C terminus (L159fsX167; final 46 amino acids), lacking the last 37 residues (Figs. 2, C and D, and 3, A and C). In patient 3, G⬎C transversion was observed leading to Q74H in the HMG box (Figs. 2, E and F, and 3A). We also performed an ASO hybridization study on fragments of SRY amplified from patients’ DNA and 44 randomly selected normal males. Figure 4 shows that these variants were found only in patients and not among any of 44 normal SRY alleles sampled in the present study. The data suggest that these variants are indeed mutations and not common polymorphisms. Discussion Normal male sex determination in mammals is targeted by the SRY gene on the Y chromosome. Timing and expression of this gene are exquisitely regulated and must probably reach the required threshold for testis formation in the developing embryo (9). These patients have mosaic 45,X/46,XY karyotype with multiple Turner stigmata. We identified two new SRY mutations in two phenotypic females with 45,X/ 46,XY mosaic karyotype. Both mutations result in altered nonfunctional protein, which may explain the female phe- FIG. 1. PCR-SSCP analysis of single exon of SRY gene in Turner syndrome patients. Lane 1, SRY from normal male control DNA; lane 2, SRY with shifted band from patient 1; lane 3, SRY with missing band from patient 2; and lane 4, SRY with shifted band from patient 3 indicates that these patients carry mutations in SRY gene. J Clin Endocrinol Metab, April 2005, 90(4):2429 –2435 2431 notypic characteristics and presence of streak gonads. Sexual differentiation during early embryonic stages is characterized by complex interaction of various genetic and nongenetic factors (22). In cascade of gonosomal and autosomal genes, the SRY gene located on the short arm of the Y chromosome is one of the first activated genes. There is evidence that SRY is essential for sex determination (8). However, there are many examples of SRY-negative individuals who differentiate to males (20% XX males). These observations strengthen the notion that there are few other (so far unidentified) genes that could influence the male differentiation. There are few reports of patients representing clinical phenotype resembling Turner syndrome with either normal or derivative Y chromosome in a high proportion of cells. Despite the presence of a structurally abnormal SRY gene, there was a dysfunction at the hormonal level during male sexual differentiation. Apparently, a relatively small proportion of the 45,X cell line is sufficient enough to suppress the male-determining function of SRY gene. This suggests that patients did not result from either abnormal sex chromosomes pairing or deletion of SRY region of the Y chromosome. Loss of the Y chromosome by nondisjunction/mitotic loss after normal disomic fertilization could lead to mosaic karyotype in these patients. It is not known, whether there is a predisposition toward the loss of the Y chromosome or it is merely a random event caused by the inherent instability/inability of the XY chromosome pairing. It is possible that even if the Y chromosome appears to be normal, mutations in other genes that reside on this chromosome, necessary for chromosome integrity, may lead to its eventual loss. This may, therefore, explain the emergence of the abundant 45,X cell line. The presence of streak gonads may be attributed to the invasion of primary genital ridge by the 45,X cell line during early developmental stages. Mutations in the SRY gene and presence of the dominant 45,X cell line in these patients may have acted in a cumulative manner to induce a cause-effect relationship. This may account for nonmasculinization in an otherwise originally XY embryo. Unequal distribution of two cell lines as seen in these patients may have originated at the time of the implantation as per their distribution into fetal and placental poles. Presence of the 45,X cell line may have determined the gonadal development into abdominal streak gonads, whereas the 46,XY cell line with the SRY mutation might have contributed toward the development of intraabdominal testis as in patient 3. The assignment of the SRY as the testis-determining factor is further supported by many studies of human intersex abnormalities (1, 23–27). These reports indicate the association of SRY mutations with gonadal dysgenesis. SRY protein belongs to the SOX family of transcription factors characterized by the HMG domain having DNA binding and bending properties. It has the ability to mediate protein-protein interactions and contains signals for nuclear import (28, 29). The rapid degradation of the truncated proteins in both these patients cannot be verified in vivo because their embryonic expression may be time and tissue specific. However, these truncated proteins found in these patients may be stable, although they are missing C-ter region, which is considered to be necessary for the 2432 J Clin Endocrinol Metab, April 2005, 90(4):2429 –2435 Shahid et al. • SRY Mutations and Turner Syndrome FIG. 2. Partial electropherograms of the SRY gene in patients. Patient 1 shows mutation N82fsX82 (A) and normal or wild-type sequence (B). Patient 2 shows a mutation L159fsX167 (C) and wild-type sequence (D). Patient 3 shows mutation Q74H (E) and wild-type sequence (F). nuclear import of these proteins. This change may form an electrostatic and hydrophobic interaction with phosphate and sugars, respectively, of DNA. This can alter the specific orientation and binding usually to DNA bases in the major groove. This change totally or at least partially may inhibit the interactions of SRY to interact with DNA (30). Insertion of adenine at codon 159 resulted in a frame shift mutation (L159fsX167) downstream of the HMG box, resulting in an altered protein at the C terminus (final 46 amino acids) lacking the last 37 residues. Only two other alterations in the C-ter region (L163X, resulting truncated protein identified in two sisters with 46,XY karyotype, and Q158fsX180 in another 46,XY patient with primary amen- orrhea, resulting in a truncated protein both at 3⬘ end) have been reported in the SRY region (15, 31). Mutation detected in the present case was not found in her paternal or sibling normal males’ DNA. It was therefore, considered to be a de novo mutation, although a paternal germ cell mosaicism cannot be ruled out. To our knowledge this is the first time that a truncated SRY protein has been found in Turner syndrome with mosaic 45,X/46,XY karyotype. These three mutations further strengthen the functional significance of the 3⬘ downstream region of the HMG box. Transversion mutation in patient 3 at codon 74 lies in the 5⬘ region of the HMG box, which contains N-terminal nuclear localization signals, highly conserved in mammals and is Shahid et al. • SRY Mutations and Turner Syndrome J Clin Endocrinol Metab, April 2005, 90(4):2429 –2435 2433 FIG. 3. A, Partial upstream and downstream sequence of HMG box showing the position of mutations (circled amino acids, affected residues). B and C, Partial sequence of SRY resulting from mutation indicating altered protein at C terminus, respectively. *, Stop or termination codon. believed to be required for complete nuclear localization (28). There is just one report showing a mutation at codon 74 in which glutamine is changed to a stop codon in a pure gonadal dysgenesis patient (24). The HMG domain is composed of three ␣-helices and adopts an L shape (32). Change of glutamine (polar, hydrophilic, and neutral amino acid) at codon 74 to histidine (polar, hydrophilic, aromatic, and charged amino acid) within helix 1 may have a direct impact on the nuclear localization of the protein that itself may influence the helix structure and/or impair its DNA binding activity. Takagi et al. (33) reported in a phenotypical female with mosaic 45,X/47,XYY karyotype a frame-shift mutation at position 422 of SRY gene. They have shown that mutant SRY may be assumed to induce a nonfunctional SRY-coded protein that lacks a DNA-binding motif. These results also explain the phenotypic female and the gonadal dysgenesis in the 45,X/47,XYY sex-reversed affected individual. Similarly, Canto et al. (16) reported in two patients presented with mosaic karyotype as 45,X/46,XY with a missense mutation as S18N in the 5⬘ non-HMG box region in DNA from both blood and streak gonads. However, Yorifuji et al. (34) could not find any mutations in the SRY gene in 11 patients with Turner syndrome. Previous studies demonstrated the presence of whole Y chromosome or Y-derived material in varying frequencies, and the presence of Y chromosome material has increased the chances of the gonadoblastoma development in these patients. The presence of intraabdominal testis in patient 3 has further strengthened the critical role of SRY sequences in this patient to develop the testis. But the predominance of the 45,X cell line, besides the presence of mutated SRY, might have impaired the total development of testicular tissue. The majority of the mutations detected so far in the SRY gene lie within the conserved motif, causing alterations in DNA binding/bending activity and therefore the origin of 46, XY females. To date only 12 mutations that lie outside the 2434 J Clin Endocrinol Metab, April 2005, 90(4):2429 –2435 Shahid et al. • SRY Mutations and Turner Syndrome Acknowledgments We thank the patients involved in this study and the clinicians from the Department of Obstetrics and Gynecology (Maulana Azad Medical College and Lok Nayak Hospital, New Delhi, India). Received June 17, 2004. Accepted January 21, 2005. Address all correspondence and requests for reprints to: Dr. Varinderpal S. Dhillon, Genome Stability Laboratory, Commonwealth Scientific and Industrial Research Organization Health Sciences and Nutrition, Gate No. 13, Kintore Avenue, P.O. Box 10041, Adelaide BC, Adelaide 5000, Australia. E-mail: [email protected]. This work was supported by Grant 3/1/2/18/2001-RHN from the Indian Council of Medical Research, New Delhi, India. References FIG. 4. ASO hybridization of wild-type (A) or mutant (B) SRY probes to SRY alleles amplified from the patients and 44 randomly chosen normal males. HMG box have been detected, and all of these have different effects on the phenotype of the patients. It is hypothesized that the regions outside the HMG box might be required to stabilize the protein binding and to generate specificity by helping to discriminate between the protein-protein interactions (12, 29). Proteins like SRY that possess only one HMG box show sequence-specific DNA binding activity probably by recognizing certain AT-rich sequences to induce bend in DNA helix. The DNA binding and bending capability of SRY protein has been demonstrated to be absolutely essential for testis development (1). The strong DNA bending together with lack of potential trans-regulation domain in human SRY has led to the suggestion that the protein may modulate transcription by acting architecturally in the assembly of a nucleoprotein complex (35). The present findings, especially the nonsense mutation downstream of HMG box of the SRY gene, further strengthen its functional importance to its expression and activity in these patients. It is therefore concluded that Turner syndrome patients must be analyzed both by conventional cytogenetic and molecular genetics approach to rule out the presence of the Y chromosome and/or the SRY gene. However, despite the critical role of SRY in the cascade of gene regulation leading to maleness, the direct targets of SRY remain to be positively identified. 1. Harley VR, Jackson DI, Hextall PJ, Hawkins JR, Berkovitz GD, Sockanathan S, Lovell-Badge R, Goodfellow PN 1992 DNA binding activity of recombinant SRY from normal males and XY females. Science 255:453– 456 2. Marcantonio SM, Fechner PY, Migeon CJ, Periman EJ, Berkovitz GD 1994 Embryonic testicular regression sequences: a part of the clinical spectrum of 46, XY gonadal dysgenesis. Am J Med Genet 49:1–5 3. Sinclair AH, Beerta P, Palmer MS, Hawkins JR, Griffiths BL, Goodfellow PN, Fellous M 1990 A gene from the human sex-determining region encodes a protein with homology to a conserved DNA-binding motif. Nature 346: 240 –244 4. Marx J 1995 Snaring the genes that divide the sexes for mammals. Science 269:1824 –1825 5. Capel B 2000 The battle of sexes. Mech Dev 92:89 –103 6. Harley VR, Lovell-Badge R, Goodfellow PN 1994 Definition of a consensus DNA binding site for SRY. Nucleic Acids Res 22:1500 –1501 7. Behlke MA, Began JS, Page DC 1993 Evidence that the SRY protein encoded by a single exon on the human Y-chromosome. Genomics 17:736 –739 8. Sinclair A 2001 Eleven years of sexual discovery. Genome Biol 2:4017 9. Cameron FJ, Sinclair AH 1997 Mutations in SRY and SOX9: testis-determining gene. Hum Mutat 9:388 –395 10. Margarit E, Soler A, Carrio A, Oliva R, Costa D, Vendrell T, Rosell J, Ballesta F 1998 Molecular, cytogenetic and clinical characterization of six XX males including one prenatal diagnosis. J Med Genet 35:727–730 11. Assumpcao JG, Benedetti CE, Maciel-Guerra AT, Guerra Jr G, Baptista, MTM, Scolfaro MR, de Mello MP 2002 Novel mutations affecting SRY DNAbinding activity: the HMG box N65H associated with 46, XY pure gonadal dysgenesis and the familial non-HMG box R30I associated with variable phenotype. J Mol Med 80:782–790 12. Shahid M, Dhillion VS, Jain N, Hedau S, Diwakar S, Sachdeva P, Batra S, Das BC, Husain SA 2004 Two new novel point mutations localized upstream and downstream of the HMG box region of the SRY gene in three Indian 46,XY females with sex reversal and gonadal tumour formation. Mol Hum Reprod 10:521–526 13. Fernandez R, Marchal JA, Sanchez A, Pasaro E 2002 A point mutation, R59G, within HMG-SRY box in a female 45, X/46, X, psu dic(Y)(pter3q11::q113pter). Hum Genet 111:242–246 14. 2003 IMG human gene database (HMGD). Cardiff, UK: Institute of Medical Genetics 15. Baldazzi L, Nicolettic A, Gennari M, Barbaro M, Pirazzoli A, Cicognanai A, Cacciari E 2003 Two new point mutations of the SRY gene identified in two Italian 46, XY females with gonadal dysgenesis. Clin Genet 64:258 –260 16. Canto P, De La Chesnaye E, Lopez M, Cervantes A, Chavez B, Vilchis F, Reyes E, Ulloa-Auirre A, Kofman-Alfaro S, Mendez JP 2000 A mutation in the 5⬘ non-high mobility group box region of the SRY gene in patients with Turner syndrome and Y mosaicism. J Clin Endocrinol Metab 85:1908 –1911 17. Jones KL 1997 Smith’s recognizable patterns of human malformation. 5th ed. Philadelphia: W. B. Saunders Co.; 81– 87 18. Chu CE, Connor JM 1995 Molecular biology of Turner syndrome. Arch Dis Child 72:285–286 19. Patsalis PC, Hadjimarcou MI, Velissriou V, Kitsiou-Tzeli S, Zera C, Syrrou M, Lyberatou E, Tsezou A, Galla A, Skordis N 1997 Supernumerary marker chromosomes (SMC) in Turner syndrome are mostly derived from the Y chromosome. Clin Genet 51:184 –190 20. Osipova GR, Karmanov ME, Kozlova SI, Evgrafov OV 1998 PCR detection of Y-specific sequences in patients with Ulrich-Turner syndrome: clinical implications and limitations. Am J Med Genet 76:283–287 21. Orita M, Suzuki Y, Sekiya T, Hyashi K 1989 Rapid and sensitive detection of point mutations and DNA polymorphisms using the polymerase chain reaction. Genomics 5:874 – 879 22. McElreavey K, Fellous M 1999 Sex determination and the Y chromosome. Am J Med Genet 89:176 –185 23. McElreavey K, Vilain E, Abbas N, Costa JM, Souleyreau N, Kucheria K, Boucekkine C, Thibaud E, Brauner R, Flamant F, Fellous M 1992 XY sex Shahid et al. • SRY Mutations and Turner Syndrome 24. 25. 26. 27. 28. 29. reversal associated with deletion 5⬘ to the SRY “HMG-box” in the testis determining region. Proc Natl Acad Sci USA 89:11016 –11020 Affara NA, Chalmers IJ, Ferguson-Smith MA 1993 Analysis of the SRY gene in 22 sex-reversed XY females identifies four new point mutations in the conserved DNA binding domain. Hum Mol Genet 2:785–789 Zeng Y, Ren Z, Zhang M, Huang Y, Zeng F, Huang S 1993 A new de novo mutation (A113T) in HMG box of the SRY gene leads to XY gonadal dysgenesis. J Med Genet 30:655– 657 Bilbao JR, Loridan L, Castano L 1996 A novel postzygotic nonsense mutation in SRY in familial XY gonadal dysgenesis. Hum Genet 97:537–539 Brown S, Yu CC, Lanzano P, Heller D, Thomas L, Warburton D, Kitajewski J, Stadtmauer L 1998 A de novo mutation (Gln2Stop) at the 5⬘ end of the SRY gene leads to sex reversal with partial ovarian function. Am J Hum Genet 62:189 –192 Südbeck P, Scherer G 1997 Two independent nuclear localization signals are present in the DNA-binding high-mobility group domains of SRY and. SOX9. J Biol Chem 272:27848 –27852 Wilson M, Koopman P 2002 Matching SOX: partner proteins and co-factors J Clin Endocrinol Metab, April 2005, 90(4):2429 –2435 30. 31. 32. 33. 34. 35. 2435 of the SOX family of transcriptional regulators. Curr Opin Genet Dev 12:441– 446 Werner MH, Bianchi ME, Gronenborn AM, Clore GM 1995 NMR spectroscopic analysis of the DNA conformation induced by the human testis determining factor. SRY. Biochemistry 34:11998 –12004 Tajima T, Nakae J, Shinohara N, Fujieda K 1994 A novel mutation localized in the 3⬘ non-HMG box region of the SRY gene in 46, XY gonadal dysgenesis. Hum Mol Genet 3:1187–1189 Read CM, Cary PD, Crane-Robinson C, Driscoll PC, Norman DG 1993 Solution structure of a DNA-binding domain from HMG1. Nucleic Acids Res 21:3427–3436 Takagi A, Imai A, Tamaya T 1999 A novel sex-determining region on Y (SRY) nonsense mutation identified in a 45,X/47,XYY female. Fertil Steril 72:167–169 Yorifuji T, Muroi J, Mamada M, Uematsu A, Kawai M, Momoi T, Kaji M, Yamanaka C, Nakahata T 2001 Analysis of the SRY gene in Turner syndrome patients with Y chromosomal material. J Med Genet 38:e41 Pontiggia A, Rimini R, Harley VR, Goodfellow PN, Lovell-Badge R, Bianchi ME 1994 Sex-reversing mutations affect the architecture of SRY-DNA complexes. EMBO J 13:6115– 6124 JCEM is published monthly by The Endocrine Society (http://www.endo-society.org), the foremost professional society serving the endocrine community.