Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Heart failure wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Coronary artery disease wikipedia , lookup
Electrocardiography wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Jatene procedure wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Heart arrhythmia wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
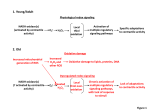
600 Cholinergic Sensitivity of the Denervated Canine Heart DONALD V. PRIOLA AND HAROLD A. SPURGEON With the technical assistance of Constantine Anagnostelis Downloaded from http://circres.ahajournals.org/ by guest on June 18, 2017 SUMMARY We determined whether the extrinsically denervated heart becomes supersensitive to acetylcholine (ACh) and nicotine (NIC). Fifteen mongrel dogs were subjected to total extrinsic cardiac denervation. The negative inotropic responses of their hearts were compared with those of 15 control dogs with respect to ACh (0.005-1.0 pig) and NIC (10-300 fig) administered intracoronary. All dogs were placed on cardiopulmonary bypass, and atrial and ventricular contractility were evaluated using a four-chamber, isovolumic technique. The denervated hearts showed no detectable supersensitivity to ACh. Because the effects of ACh at the doses used are almost completely on the decentralized cardiac muscle cells, the results indicate that the cardiac muscle is an exception to the increased sensitivity usually produced by decentralization. When the positive inotropic effects of NIC were blocked by practolol in the control hearts, the negative inotropic effects of the intrinsic parasympathetic neurons (IPN) are seen clearly. These intrinsic neural elements are specifically activated by NIC. The denervated atria and ventricles displayed NIC dose-response curves that consistently were shifted to the left when compared to control animals after 0,-blockade. These results indicate the IPN, which are denervated by the surgical procedure, do become more sensitive to NIC. The increases in sensitivity to NIC were between 2- and 6-fold, comparable to the increased sensitivity to norepinephrine observed in denervated hearts. The postjunctional IPN supersensitivity probably occurs as a result of spreading of nicotinic receptors on the ganglion cell membrane. WALTER B. CANNON formulated a "law of denervation" based upon extensive experimental work with neuroeffector systems.1 Simply put, this "law" stated that a denervated organ becomes supersensitive, after a time, to its usual neurotransmitter substance. The most exquisite example of this denervation supersensitivity is seen in skeletal muscle whose sensitivity to acetylcholine increases as much as 1000-fold following denervation.2 Other structures show varying degrees of supersensitivity, depending on many factors, among which is whether the denervation is pre- or postganglionic.3 The heart, once thought to be an exception to this law, demonstrates an increase in sensitivity to norepinephrine (NE) of 1.5-10-fold following denervation,4"6 depending on whether one is measuring atrial contractility, ventricular contractility, or heart rate .5 The question of whether or not the heart becomes supersensitive to cholinergic agents following denervation is, however, unsettled. The scanty data which exist are often inconclusive and contradictory.7-8 The following experiments were performed to determine whether the extrinsically denervated heart becomes supersensitive to cholinergic agents which may interact From the Departments of Physiology and Pharmacology, The University of New Mexico, School of Medicine, Albuquerque, New Mexico. Supported by Grant No. HL-10869 from the National Institutes of Health and a Cooperative Grant from the American and New Mexico Heart Associations. Dr. Priola was the recipient of Research Career Development Award KO 5 HL-15, 912 from the National Heart and Lung Institute. Dr. Spurgeon's present address is: Gerontology Research Center, National Institutes of Health, Baltimore City Hospitals, Baltimore, Maryland. Address for reprints: Donald V. Priola, Ph.D., Department of Physiology, The University of New Mexico, School of Medicine, Albuquerque, New Mexico 87131. Received November 8, 1976; accepted for publication April 11, 1977. with myocardium and cardiac parasympathetic neural elements. Two types of agents were employed: one that primarily interacts with the effector cells (acetylcholine) and one that primarily interacts with the intrinsic parasympathetic ganglion cell (nicotine). In this manner, it was hoped that denervation-induced sensitivity changes in either the effector cell or the intrinsic innervation, or both, could be determined. Methods CHRONIC EXPERIMENTS Fifteen mongrel dogs were anesthetized with thiopental sodium (20-25 mg/kg) and subjected to total extrinsic denervation of the heart using the method of Geis et al.9 The procedure consists of two operations separated by an interval of 1-2 weeks. In the first operation, the left atrium is separated from its mediastinal attachments from the superior to the inferior junctions with the interatrial septum and reanastomosed. At the same time, the aorta and pulmonary artery are circumferentially stripped of their adventitial layers. In the second operation, the entire wall of the right atrium, as well as the interatrial septum, is incised and reanastomosed. The latter incision is done under inflow occlusion. This technique produces a heart that has been effectively separated from all mediastinal connections which may act as pathways for both sympathetic and parasympathetic cardiac nerves. It produces a heart that is postganglionically denervated with regard to its sympathetic nerves, but preganglionically denervated with regard to its parasympathetic nerves. A period of 3-6 weeks was allowed for recovery before these dogs were employed in the acute phase of the experiments. This is ample time for development of supersensi- CHOLINERGIC SENSITIVITY OF THE HEART/Pno/a and Spurgeon Downloaded from http://circres.ahajournals.org/ by guest on June 18, 2017 tivity to norepinephrine which usually reaches its maximum in 1-2 weeks.5 Prior to their acute use, the adequacy of denervation was established by supramaximal stimulation of the cervical vagi (30 Hz, 5 msec, 2-10 V) and the stellate ganglia (10 Hz, 5 msec, 10 V). In addition, tyramine, 500 ptg, was injected into the coronary circulation. A change of >10% from control values in atrial contractility, ventricular contractility, or heart rate in response to any one of these procedures was considered sufficient to eliminate the animal from inclusion in the experimental data. No negative inotropic responses to vagal stimulation were observed in the denervated dogs used in this study. In addition, atrial and ventricular myocardial samples were removed after the experiment and analyzed for catecholamine content (both epinephrine and NE). All the denervated dogs used in this study showed NE levels of <0.02 fig/g wet weight in all chambers sampled. Total catecholamine levels (NE + epinephrine) averaged 0.05 ± 0.01 fig/g wet weight in hearts from the denervated dogs. ACUTE EXPERIMENTS In addition to the denervated animals, 15 control dogs were used in these experiments. All dogs were anesthetized with thiopental sodium (25-30 mg/kg, supplemented as necessary) and the chests were opened by transsternal thoracotomy in the fourth or fifth interspace. The cervical vagi and stellate ganglia were isolated and prepared for stimulation and the left carotid artery was cannulated for pressure recording and subsequent drug injections. The tip of the carotid cannula was positioned just at the aortic side of the aortic valve. Once cardiac bypass was established, drugs injected into this cannula would then enter the coronary circulation directly because of the retrograde nature of arterial perfusion during bypass. Total cardiopulmonary bypass was accomplished in the usual manner. Venous return from the venae cavae was drained into a disc oxygenator, oxygenated in an atmosphere of 100% O2, warmed, filtered, and returned to the dog via a femoral artery. Sumps in both ventricles were placed under airrelieved suction and the coronary and bronchial blood was collected and returned to the oxygenator. Arterial pH was measured at intervals throughout the experiments with an Instrumentation Laboratories bloodgas analyzer and ranged between 7.35 and 7.40. Arterial blood temperature was monitored with a thermistor probe (Yellow Springs Instruments) placed directly in the arterial inflow line. The blood temperature was maintained between 34 and 36°C by warming the oxygenator with heat lamps. Arterial pressure was monitored by placing a catheter in the ascending aorta with a pressure transducer (Trantec). In these experiments, arterial pressure varied between 75 and 125 mm Hg. To record the contractile activity of the cardiac chambers, a four-chamber isovolumic technique was used. This technique and the method of drug injection have been described in earlier publications.10' " Saline-filled balloons in each of the four chambers were used to record isovolumic pressures. Diastolic pressures were adjusted to 1-5 mm Hg in the atria and 3-8 mm Hg in the ventricles, 601 pressures equivalent to those recorded in the open-chest dog preparation. The heart rate was held constant by pacing from the right atrium. With heart rate, preload, and afterload eliminated as variables, changes in isovolumic pressures very closely reflect changes in chamber contractility. All drugs were administered intracoronary via the carotid cannula in volumes of 0.5-1.0 ml followed by a 1- to 2-ml wash with normal saline. Acetylcholine (ACh), in doses of 0.005-1.0 fig, was used to produce the expected negative inotropic responses of the cardiac muscle. Nicotine HO (NIC) was used to activate the intrinsic parasympathetic neural elements (IPN). The doses employed were 10-300 /ig. These doses have been shown to produce a highly selective activation of IPN which results in negative inotropic responses of both atria and ventricles." These responses to NIC can be blocked totally by neural or ganglionic blocking agents, while the responses to ACh are completely unaffected." Thus, the two agents can be employed to study the effects of denervation on both the decentralized effector cell and the denervated IPN. In dogs with intact cardiac nerves, NIC also induces the release of NE from postganglionic sympathetic neurons. This results in an indirect, positive inotropic drug effect. In seven experiments on control dogs, these effects were abolished with 2-4 mg of intracoronary practolol, a /3,adrenergic blocking agent. The responses of these control animals after practolol were used as the control group to detect changes in sensitivity of the intrinsic innervation to NIC in the denervated dogs. Changes in isovolumic pulse pressures in response to the injections were measured and expressed as percent change from control ± SEM. Significance of differences between the means of responses in the two groups of dogs was analyzed by Student's Mest. A level of P < 0.05 was considered to indicate a significant difference. Results RESPONSES TO ACh Typical responses of a normal and a denervated dog to ACh, 0.5 jxg, are shown in Figure 1. Both hearts were CONTROL DENERVATED RA 1 RV so- .5mcg ACH FIGURE 1 Recordings which illustrate typical responses of an intact heart (left panel) and a denervated heart (right panel) lo 0.5 fj.g acetylcholine (ACh) (arrows). Isovolumic pressures from the right atrium (RA), right ventricle (RV), left atrium (LA), and left ventricle (LV) are shown. Calibrations (center) are in mm Hg. 602 CIRCULATION RESEARCH Downloaded from http://circres.ahajournals.org/ by guest on June 18, 2017 paced at a constant rate from the right atrium (RA). In the normal heart, both RA and left atrial (LA) isovolumic pressures decrease within a few beats following injection and show significant recovery even before the maximum ventricular depressions have been reached. Both the right (RV) and left (LV) ventricles display negative inotropic responses to ACh, but they develop more gradually (1520 sec) and recover more slowly. These differential atrial and ventricular responses to injected ACh have been reported earlier" and also are typical of atrial and ventricular responses to vagus nerve stimulation.10 The responses of the denervated heart to the same dose of ACh (right panel) are not remarkably different either quantitatively or qualitatively from those of the control animal. In this particular dog, the LA was not responsive to ACh at this dose level. It is important to note that in no case is there a significant positive component to the cardiac responses to ACh. These recordings are quite representative of what was observed overall; i.e., injection of ACh in doses of up to 1.0 /xg, intracoronary, rarely produced any significant positive inotropic response. These observations are in sharp contrast to those for NIC which are described below. The apparent lack of supersensitivity to ACh observed in the denervated dogs is substantiated by the overall comparative data shown in Figure 2. In only one chamber and at only one dose level (RA, 0.01 /xg) is the response of the denervated heart significantly greater than that of the normal heart. In fact, the opposite appears to be true, i.e., in most instances, the denervated heart exhibits less depression in response to ACh than does the intact heart. In four cases, these lesser responses are significantly different at the P — 0.05 level. As previously reported for denervated animals," the most responsive chambers to ACh in the normal dogs were the RA and LA. The RA VOL. 41, No. 5, NOVEMBER 1977 ventricles generally displayed about 50% of the negative inotropic responses of the atria. Except for the RA, these differences are not nearly as clear in the denervated dogs. In both groups of dogs, inotropic responses do not show a clear relationship to ACh dose. Based on the data shown in Figure 2, it does not appear that the denervated heart shows any supersensitivity to the negative inotropic effects of ACh. RESPONSES TO NIC Intracoronary injection of NIC has been shown to activate the intrinsic parasympathetic ganglion cells (IPN) in the heart." Although the cardiac muscle cells undergo parasympathetic decentralization following chronic extrinsic cardiac denervation, these intrinsic neural elements are denervated by the procedure.12 The comparative responses to NIC of the two groups should, therefore, reflect any supersensitivity of the IPN. Typical responses of control hearts (before and after j3,blockade), as well as denervated hearts, to 50 /ig of NIC are shown in Figure 3. Prior to /3,-blockade (left panel), the negative inotropic responses produced by nicotinic activation of the IPN are masked by concurrent release of NE from postganglionic sympathetic nerves. This results from stimulation of nicotinic receptors on the adrenergic nerve fiber.13' H This indirect NIC action is apparent in the responses of the RV in Figure 3. After elimination of this indirect action by /3,-blockade (central panel) or denervation (right panel), only negative inotropic responses are produced. These negative inotropic effects of NIC are qualitatively similar to those produced by ACh (Fig. 1), in that the atrial depression has a short latency and a fast recovery (RA), while the ventricular responses are slower in both developing and recovering (RV and LV, right LA RV LV j I control • denervated I < T a: i- z o o I T a. o .01 .05 .5 s .01 I I .05 .1 -S 81 .85 .1 .01 .05 ACH DOSE,meg INTRACORONARY FIGURE 2 Summary of responses of intact (open bars) and denervated hearts (closed bars) to acetylcholine (ACh). Each bar is the mean of 15 experimental values. SEM is shown by the brackets. Chambers are as in Figure I. Significant differences (P < 0.05) of denervated from control responses at a given dose are indicated by • . CHOLINERGIC SENSITIVITY OF THE HEART/Priola and Spurgeon CONTROL no blockade CONTROL DENERVATED after A blockade RA1 RV LA Slmcg NICOTINE 51 m e g NICOTINE 51 meg NICOTINE FIGURE 3 Recordings illustrating typical responses of intact hearts before (left panel) and after (center panel) f},-blockade with practolol and denervated hearts (right panel) to the same dose of nicotine (arrows). Left and center panel recordings are from the same dog. Calibrations are in mm Hg. Chambers are as in Figure 1. Downloaded from http://circres.ahajournals.org/ by guest on June 18, 2017 panel). The responses of the denervated dog shown in Figure 3 suggest an increase in sensitivity to NIC as a result of denervation of the IPN. After /3,-blockade, the control heart shows little negative inotropic response to 50 /ng NIC, whereas the denervated heart exhibits significant RA, RV, and LV negative inotropy in response to the same dose. When the overall responses of the control (without /3,blockade) and denervated hearts are compared, some clear differences emerge (Fig. 4). At the lower doses of NIC (25 and 50 fig), the control animals show responses that are entirely negative. At the higher doses (100 and 200 /tig), most of the responses are positive. Obviously, the net response of a chamber to NIC is the resultant of the indirectly mediated positive response and the indirectly mediated IPN negative response. In the case of the denervated dogs, the degeneration of the postganglionic sympathetic nerves eliminates the source of NE for the indirect positive response. Therefore, all NIC responses observed in the denervated dogs were negative. On this basis, many of these responses were significantly different from those of the normal dogs. Positive responses to NIC in the 15 denervated animals were very rare; i.e., only nine of 168 observations (5%) were positive. In the 15 intact dogs, 56 of 131 responses to NIC were positive (43%). To provide suitable control responses with which the responses of the denervated animals might be compared, seven intact dogs were given NIC following /3,-blockade with practolol. Figure 5A-D compares the NIC doseresponse curves for the four heart chambers in these two groups. After/3,-blockade, only 10 of 153 responses of the intact dogs to NIC were positive (6.5%). Overall, the denervated dogs displayed an increased sensitivity to NIC. Although the differences between the mean values of the two groups were not all statistically significant, the doseresponse curves for the denervated group were consistently shifted to the left, compared with intact dogs, after /3,-blockade. In Figure 5A, the RA curve for the denervated dogs is significantly shifted to the left, indicating an increase in sensitivity of 3- to 5-fold, depending upon 603 which portion of the curves one selects for comparison. Responses of the denervated animals at 25 and 50 /xg NIC are significantly greater than control. There is no significant difference between maximum responses in the two groups except that they occur at different dose levels. The sensitivity changes in the LA (Fig. 5B) are not as clear. Although the dose-response curve for the denervated dogs is shifted to the left, only the 25 /Ag point is clearly statistically different from control. The magnitude of the shift is approximately 2-fold. There is also evidence in the RV responses that denervation increases sensitivity to NIC (Fig. 5C). Although responses to the two lower doses of NIC do not appear to be different between the two groups, the denervated dogs show a significantly higher response at 100 /ng. The RV is the only chamber in which denervation did not produce an apparent decrease in the threshold dose of NIC. This latter change is clear in the doseresponse curves of Figure 5D. The LV of the denervated dogs exhibits an increased sensitivity to NIC throughout the dose range studied. The difference at only one dose level (100 /Ltg) is statistically significant. Depending on the method of comparison used, the LV of the denervated dogs appears to be 2-4 times more sensitive to NIC than that of the control animals. If one uses the horizontal displacement of the dose-response curve, the increase could be as much as 6-fold. As reported earlier," these responses to NIC could subsequently be blocked by 10-30 /xg of tetrodotoxin, intracoronary, which had no effect on responses to ACh. Discussion On the basis of the data presented, it is clear that the extrinsically denervated heart does not become supersensitive to ACh (Fig. 2). The lack of supersensitivity is undoubtedly related to the fact that the surgical denervation produces a decentralization rather than a denervation of the atrial and ventricular effector cells. This contrasts with data on other organ systems3'I5> 16 which indicate a modest (2- to 4-fold) increase in sensitivity following dedenervated control RA 25 5* 1M 211 25 56 IN 2M 25 51 IN 2M 25 SO IN 2M nicotine dose, meg intracoronary FIGURE 4 Summary of isovolumic inotropic responses to nicotine before /J,-blockade of intact (open bars) and denervated hearts (closed bars). Ordinate indicates percent change of isovolumic pressure from control, and dose of nicotine is shown on abscissa. Each value represents the mean of 15 experiments and the bracket indicates the SEM. Chambers are as in Figure I; • = P < 0.05. CIRCULATION RESEARCH 604 IS RIGHT ATRIUM —Control After Ri Blockade , Cardiac Denervated 3VOLUAHIC PRESSURE, FROM (CONTROL y / 5 SO / J a;"- I 1977 LEFT ATRIUM • Contol After Bi Blockade Cardiac Denervated UJ V VOL. 4 1 , No. 5, NOVEMBER '10- 1 31 40 20 NICOTINE, meg 30 40 SO 60 70 <( s'o 9'oibo 200 300 NICOTINE,meg Downloaded from http://circres.ahajournals.org/ by guest on June 18, 2017 111 K 3 ffig KrO.Z UO20- RIGHT VENTRICLE •-Control After 81 Blockade -Cardiac Denervated 25- L.. lll_ LEFT VENTRICLE —Control After Bi Blockade ° -Cardiac Denervated 20- Q.Z **"i |8.sH _iO 1 5 OK -1-'" >"• O 8? H 40 SO 60 70 80 90100 300 NICOTINE, meg ~30^ 40 50 60 70 I 90100 —I— 200 301 NICOTINE.mcg FIGURE 5 A -D, Dose-response curves for nicotine as measured in the right atrium (A), left atrium (B), right ventricle (C), and left ventricle (D) of normal dogs after (3,-blockade (solid lines) and of denervated dogs (broken lines). The average percent decrease of isovolumic pressure from control is shown on the ordinate, and the dose of nicotine is shown on the abscissa on a log scale. Each point represents the average of 15 experiments, and the bracket indicates the SEM. Curvesfittedby eye. Values for denervated dogs that significantly differ from control (P < 0.05) are indicated by • . centralization. As early as 1936, Cannon and Rosenblueth'6A showed that the denervated superior cervical ganglion displayed a response threshold to ACh that was only one-fourth that of the innervated ganglion. The decentralized nictitating membrane was used as the test system. The phenomenon of supersensitivity following decentralization has also been demonstrated in vas deferens and other effector cells.16 Very little information has been available regarding cholinergic sensitivity of the denervated heart. Recently, Jacobs and his co-workers7 have reported that extrinsic cardiac denervation does not appear to alter the bradycardia in response to ACh. However, these workers did show an increased tendency for atrioventricular (AV) block in response to ACh, suggesting a possible increase in AV nodal sensitivity. More recently, Hageman et al.8 have shown that the perfused sinoatrial (SA) node of selectively parasympathectomized animals does not show an increased sensitivity to ACh injected directly into the isolated SA nodal artery. It appears that the inotropic sensitivity of the denervated heart to ACh also is an exception to the general observations following decentralization. If atrial and ventricular muscle do show any moderately increased cholinergic sensitivity following extrinsic denervation, perhaps the techniques used in these experiments were not sensitive enough to demonstrate it. There is considerable response variability in the methods used because of the stress placed upon the animal, variation in the pattern of drug delivery through the coronary circulation, and the nature of the isovolumic pressure-recording technique. It may be that this variability would be enough to obscure small changes in sensitivity. However, the data of Figure 2 are quite clear and appear to rule out such marginally detectable changes. It is more likely that the heart is indeed an exception to the usual enhancement produced by chronic decentralization. There is no technique presently available for selectively eliminating the IPN in order to obtain truly cholinergically denervated cardiac muscle cells. It is conceivable that chronic ganglionic blockade as used in other organs15 might accomplish this objective. Until elimination of the IPN can be accomplished, the question of whether denervated cardiac muscle becomes supersensitive to ACh will remain unanswered. As we have shown previously, the negative inotropic CHOLINERGIC SENSITIVITY OF THE HEART/Priola and Spurgeon Downloaded from http://circres.ahajournals.org/ by guest on June 18, 2017 effects of NIC at these doses are primarily the result of activating the IPN." Denervation of the 1PN (which would be expected from the surgical technique used) does result in an increased sensitivity to nicotinic stimulation (Fig. 5A-D). Although these increases are not statistically significant in all chambers at all dose levels, the NIC doseresponse curves in the denervated dogs are consistently shifted to the left of the control curves. There are enough statistically significant differences to conclude that denervation supersensitivity of the IPN does occur. This supersensitivity is only apparent, however, when the indirect positive inotropic effects of NIC in the control dogs are blocked by practolol. In the absence of practolol (Fig. 4), the effects of NIC on the IPN are obscured by release of catecholamine from sympathetic postganglionic nerves. This phenomenon has been described previously by a number of workers.14' l7~20 That the sources of this positive inotropic effect of NIC are the sympathetic cardiac neural elements is verified by the complete absence of positive inotropic effects in the denervated animals (Fig. 4). The increased sensitivity of the IPN is probably the result of a postsynaptic change which involves a "spreading" or increased number of drug-sensitive receptors on the membrane of the ganglion cell similar to the well known effect of denervation on the cell membranes of skeletal muscle.2'21 Kuffler and his co-workers22 have shown that the area of chemosensitivity of IPN cells in the interatrial septum of the frog heart increases greatly after section of the vagosympathetic trunks. The time course of development of this IPN supersensitivity (4-8 days) correlates well with the usual time course for supersensitivity development.16 Therefore, the increased responsiveness to NIC seen in the cardiac-denervated animals probably represents a true postjunctional or type II16 supersensitivity of the intrinsic nerves of the heart. No such supersensitivity was observed with ACh (Fig. 2). Neither was ACh effective in producing indirect positive inotropic responses similar to those of NIC. There are at least two reasons for these findings. First of all, nicotinic receptors of the cardiac nerves are probably much less sensitive to ACh than are muscarinic receptors on the cardiac muscle cells. Blumenthal et al.23 have shown that intracoronary doses of ACh from 0.01 to 1.0 fxg produce only negative inotropic effects on the canine LV that can be blocked by atropine. In order to produce positive inotropic effects, the dose of ACh had to be raised to 20300 j/.g, and prior administration of neostigmine and atropine was necessary. These positive responses could then be blocked completely by intracoronary administration of tetraethylammonium chloride.23 These observations indicate a vastly greater ACh sensitivity of cardiac muscarinic receptors, compared with nicotinic receptors. This would explain why ACh did not produce any positive inotropic responses at the doses employed in this study (0.01-0.5 /xg). Even with an increased nicotinic sensitivity of the IPN following denervation, the doses of ACh used probably were still insufficient to produce IPN activation. These speculations assume, of course, that the nicotinic receptors on the IPN and those on the sympathetic nerve endings have approximately the same characteristics. Second, the 605 inotropic responses to both direct and indirect actions of ACh (muscarinic and nicotinic) are qualitatively identical. Therefore, any effects of IPN stimulation which would be produced at the doses used would probably be much less than the direct effects of ACh on the effector cells. Thus, IPN stimulation by ACh would not be detectable under the present experimental circumstances even if it should occur at the doses used. The adrenergic supersensitivity produced by cardiac denervation4"6 would be considered a type I or "deviation" supersensitivity according to Fleming's classification;16 i.e., a change in the percent of an administered amount of a drug that is available in the biophase to interact with its receptors. This results from the loss of the catecholamine reuptake mechanism that had existed in the degenerated sympathetic nerve endings. In contrast, the decentralization supersensitivity observed in the present experiments would fit Fleming's classification as type II or "nondeviation" supersensitivity; i .e., enhanced responsiveness of the target cells (IPN). It is interesting to note that these two diverse mechanisms produce the same order of magnitude of supersensitivity, 2- to 10-fold. The chamber that illustrates the enhanced sensitivity to NIC most clearly is the RA (Fig. 5A). This correlates well with anatomical evidence that indicates the largest concentration of parasympathetic ganglion cells is in the R A .24' 25 References 1. Cannon WB: A law of denervation. Am J Physiol 198: 737-750, 1939 2. Miledi R: The acetylcholine sensitivity of frog muscle fibers after complete or partial denervation. J Physiol (Lond) 151: 1-23, 1960 3. Fleming WW, McPhillips JJ, Westfall, DP: Postjunctional supersensitivity and subsensitivity of excitable tissues to drugs. Ergeb Physiol 68: 55-119,1973 4. Dempsey PJ, Cooper T: Supersensitivity of the chronically denervated feline heart. Am J Physiol 215: 1245-1249, 1968 5. Priola, DV: Individual chamber sensitivity to norepinephrine after unilateral cardiac denervation. Am J Physiol 216: 604-614, 1969 6. Spann JF, Sonnenblick EH, Cooper T, Chidsey CA, Willman VL, Braunwald E: Cardiac norepinephrine stores and the contractile state of heart muscle. Circ. Res. 19: 317-325, 1966 7. Jacobs HK, Randall WC, Kaye MP: Responses of the parasympathectomized canine heart to neurohumora! stimulation (abstr). Physiologist 17: 254, 1974 8. Hageman GR, Urthaler F, James TN: Absence of supersensitivity to acetyl choline in the extrinsically denervated canine sinus node (abstr). Physiologist 18: 236, 1975 9. Geis WP, Tatooles CJ, Kaye MP, Randall WC: Complete cardiac denervation without transplantation; a simple and reliable technique. J Appl Physiol 30: 289-293, 1971 10. Priola DV, Fulton R: Positive and negative inotropic responses of the atria and ventricles to vagosympathetic stimulation in the isovolumic canine heart. Circ Res 25: 265-275, 1969 11. Priola DV, Spurgeon HA, Geis WP: The intrinsic innervation of the canine heart; a functional study. Circ Res 40: 50-56, 1977 12. Napolitano LM, Willman VL, Hanlon CR, Cooper T: Intrinsic innervation of the heart. Am J Physiol. 208: 455-458, 1965 13. Lee WC, Shideman FE: Mechanism of the positive response to certain ganglionic stimulants. J Pharmacol Exp Ther 126: 239-249, 1959 14. Westfall TC, Brasted M: The mechanism of action of nicotine on adrenergic neurons in the perfused guinea-pig heart. J Pharmacol Exp Ther 182: 409-418, 1972 15. Trendelenburg U: Supersensitivity and subsensitivity to sympathomimetic amines. Pharmacol Rev 15: 225-276, 1963 16. Fleming WW: Variable sensitivity of excitable cells; possible mechanisms and biological significance. Rev Neurosci 2: 43-90, 1976 16A. Cannon WB, Rosenblueth A: The sensitization of a sympathetic ganglion by preganglionic denervation. Am J Physiol 116: 408-413, 1936 17. Bassett AL, Wiggins JR, Danilo P, Jr, Nilsson K, Gelband H: Direct and indirect inotropic effects of nicotine on cat ventricular muscle. J 606 CIRCULATION RESEARCH Pharmacol Exp Ther 188: 148-156, 1974 18. Kako. K, Chrysohou A, Bing RJ: Factors affecting myocardial storage and release of catecholamines. Ore Res 9: 295-299, 1961 19. Tillmanns H, Ikeda S, Bing RJ: The effect of nicotine on the coronary microcirculation in the cat heart. J Clin Pharmacol 14: 426-433, 1974 20. Su C, Bevan JA: Blockade of the nicotine-induced norepinephrine release by cocaine, phenoxybenzamine and desipramine. J Pharmacol Exp Ther 175: 533-540, 1970 21. Dreyer F, Peper K: The spread of acetylcholine sensitivity after denervation of frog skeletal muscle fibers. Pfluegers Arch 348: 287-292, 1974 VOL. 41, No. 5, NOVEMBER 1977 22. Kuffler SW, Dennis MJ, Harris AJ: The development of chemosensitivity in extrasynaptic areas of the neuronal surface after denervation of parasympathetic ganglion cells in the heart of the frog. Proc R Soc Lond [Biol] 177: 555-563, 1971 23. Blumenthal MR, Wang H, Markee S, Wang SC: Effects of acetylcholine on the heart. Am J Physiol 214: 1280-1287, 1968 24. Truex RC: Chromaffin tissue of the sympathetic ganglia and heart. Anat Rec 108: 687-697, 1950 25. Jacobowitz D: Histochemical studies of the relationship of chromaffin cells and adrenergic nerve fibers to the cardiac ganglia of several species. J Pharmacol Exp Ther 158: 227-240, 1967 Heterogeneity of the Hypoxic State in Perfused Rat Heart CHARLES STEENBERGEN, GILBERT DELEEUW, CLYDE BARLOW, BRITTON CHANCE, AND Downloaded from http://circres.ahajournals.org/ by guest on June 18, 2017 JOHN R. WILLIAMSON SUMMARY Tissue oxygen gradients were examined in the saline-perfused rat heart by NADH fluorescence photography. In high flow hypoxia, where the coronary flow was maintained and the arterial oxygen tension was gradually reduced, oxygen extraction was virtually complete before oxygen consumption was significantly diminished. Inadequate oxygen delivery resulted in a well defined pattern of anoxic zones. The anoxic zones were several hundred microns in width, an order of magnitude greater than intercapillary distances. In low flow hypoxia (ischemia), where the arterial oxygen tension remained at its control value and the coronary flow was diminished, anoxic zones also developed, following the same pattern as in high flow hypoxia. However, in ischemia, the anoxic areas developed while the effluent oxygen tension was significantly greater than zero. Whereas respiratory acidosis between pH 7.3 and 6.9 resulted in vasodilation, below pH 6.8 there was a marked increase in vascular resistance. Anoxic zones appeared despite only a slight change in effluent oxygen tension from the control. In high flow hypoxia, ischemia, and acidosis-induced ischemia, the anoxic zones disappeared when control perfusion conditions were restored. The data demonstrate that tissue oxygen gradients are very steep in the hypoxic state, so that ischemia and hypoxia result in discrete heterogeneous areas of anoxic tissue bounded by sharp areas where the oxygen supply is sufficient to maintain normal mitochondrial oxidative function. In these states in which oxygen delivery is less than oxygen demand, coronary perfusion appears to be regulated at the level of the arterioles rather than the capillaries. MYOCARDIAL ENERGY production is predominantly determined by aerobic metabolism. ATP synthesis from glycolysis during anoxia is insufficient to maintain cardiac work at its normoxic level, even though glycolytic flux is increased significantly.1"3 Therefore, the delivery of oxygen to the myocardial cells is crucial for normal function. The heart has a rich network of capillaries which provide adequate blood supply under the normal range of work loads so that oxygen delivery does not limit oxygen consumption.4 However, when either the arterial Po2 or the blood flow is lowered below critical levels, oxygen delivery can diminish until it limits aerobic ATP synthesis. The nature of the oxygen gradients in the hypoxic myocardium under these conditions is not well understood. Several theoretical treatments of this issue have been previously presented.5 Initially, oxygen was assumed to be From the Department of Biochemistry and Biophysics. University of Pennsylvania, Philadelphia. Pennsylvania. Supported by National Institutes of Health Grants HL-14461. HL18708, and GM-07170. Address for reprints: Dr. John R. Williamson, University of Pennsylvania. Department of Biochemistry and Biophysics, School of Medicine-G3, Philadelphia. Pennsylvania 19104. Received December 23. 1976; accepted for publication May 5. 1977. supplied to the tissue based on diffusion according to Fick's law. More recently, the importance of myoglobinfacilitated oxygen transport has been recognized." The two principal theoretical models of oxygen delivery are Krogh's cylinder model, which assumes that the venous Po2 limits oxygen diffusion from the capillary, and Diemer's cone model, which recognizes that capillary Po2 varies from the arterial to the venous end but requires that blood flow in adjacent capillaries be in opposite directions. Both models predict that, in the hypoxic myocardium, the anoxic zones should be confined to the tissue at the greatest distance from a capillary. More complex mathematical models based on a single capillary and its surrounding tissue have been devised, but they also predict that oxygen supply will first become limiting in the '"lethal" corners." According to these models, the size of the anoxic areas may increase as the arterial P02 is decreased, but the tissue immediately adjacent to a capillary should remain well oxygenated and the tissue Po2 should decline as the distance from a capillary increases. Grunewald8 has attempted to determine the effect of inhomogeneity in the coronary circulation, but. in the absence of experimental data, he could onlv conclude that the tissue Po2 distribu- Cholinergic sensitivity of the denervated cannine heart. D V Priola and H A Spurgeon Downloaded from http://circres.ahajournals.org/ by guest on June 18, 2017 Circ Res. 1977;41:600-606 doi: 10.1161/01.RES.41.5.600 Circulation Research is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1977 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7330. Online ISSN: 1524-4571 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circres.ahajournals.org/content/41/5/600.citation Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation Research can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation Research is online at: http://circres.ahajournals.org//subscriptions/