Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Malnutrition in South Africa wikipedia , lookup
Gastric bypass surgery wikipedia , lookup
Food politics wikipedia , lookup
Food studies wikipedia , lookup
Obesity and the environment wikipedia , lookup
Human nutrition wikipedia , lookup
Food choice wikipedia , lookup
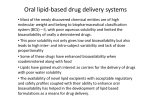
The EFSA Journal (2007) 490, 1-20 Opinion of the Scientific Panel on Food Additives, Flavourings, Processing Aids and Materials in Contact with Food on a request from the Commission related to D-alpha-tocopheryl polyethylene glycol 1000 succinate (TPGS) in use for food for particular nutritional purposes Question number EFSA Q-2003-126 Adopted on 17 April 2007 SUMMARY The Scientific Panel on Food Additives, Flavourings, Processing Aids and Materials in Contact with Foods (AFC Panel) has been asked to advise on the safety and bioavailability of d-α-tocopheryl polyethylene glycol-1000 succinate (TPGS) as a source of vitamin E under Commission Directive 2001/15/EC on substances that may be added for specific nutritional purposes in foods for particular nutritional uses. The present opinion deals only with the safety of d-α-tocopheryl polyethylene glycol1000 succinate as a source of d-α-tocopherol and with the bioavailability of the nutrient from this source, intended to be used in foods for particular nutritional uses. The safety of the nutrient itself, d-α-tocopherol, in terms of amounts that may be consumed, is outside the remit of this Panel. TPGS is intended to be used in patients (mainly infants and children) with impaired vitamin E absorption due to fat malabsorption. The normal bioavailability of fatsoluble vitamin E depends on fat absorption and requires bile acids and pancreatic enzymes to be present. Conditions where insufficient bile is secreted such as cholestatic liver disease or where insufficient pancreatic enzymes are secreted such as cystic fibrosis lead to impaired vitamin E absorption and if not corrected may lead to neurological disorders. Studies in patients with cholestatic liver disease have shown that TPGS administration can correct impaired vitamin E bioavailability in these patients (at a dose level of 20-25 IU/kg bw/day (51.7 –64.5 mg/kg bw/day). Studies to address the bioavailability and safety of TPGS have been conducted, both in humans and in animals. The absorption, distribution and excretion of the PEG 1000 moiety of TPGS have been examined in rats in several studies using radiolabelled TPGS. The majority of the radiolabelled material was rapidly eliminated with the faeces (72-85 %) and urine (7-13%) within 24 hours. In teenage children with chronic cholestasis 1.7% of the administered polyethylene glycol 1000 contained in the TPGS was excreted in the urine, compared with 3.0 % in normal adults. This showed that the systemic exposure to PEG 1000 from TPGS was not higher in persons with © European Food Safety Authority, 2007 TPGS in food for special medical purposes EFSA Journal (2007) 490, p. 2 of 20 impaired bile secretion than in normal persons and that it was lower than in rats, the species used in the safety studies on TPGS. From toxicology studies, an overall no-observed-adverse-effect level (NOAEL) of 1000 mg/kg bw/day can be derived. TPGS is not genotoxic. Limited chronic toxicity and carcinogenicity studies in rats and mice using “TPGS-4001” instead of TPGS, which would be expected to provide a higher systemic exposure to PEG, showed no toxic effects at doses higher than the overall NOAEL of 1000 mg/kg bw/day. The Panel concluded that in the absence of genotoxic effects the safety of TPGS can be assessed on the basis of the overall NOAEL equivalent to 1000 mg TPGS/kg body weight per day, established in a subchronic toxicity study in rats. TPGS is only to be used for food for special medical purposes under medical supervision at estimated intakes varying from 5 mg TPGS /kg bw in teenagers to 13 mg TPGS /kg bw in 1 month old infants. Potential intake would be lower in adults. This provides an adequate margin of safety (ratio between the NOAEL and the intake) compared with the NOAEL of 80 to 200 for infants and young children. The Panel also noted that these estimated intakes to TPGS would correspond to intakes to PEG 1000 at levels equivalent to 3.3 – 8.5 mg/kg bw/day. This is within the range of the group Acceptable Daily Intakes established by the EC Scientific Committee on Food (5 mg/kg bw for PEG 300 - 4000) and the Joint FAO/WHO Expert Committee on Food Additives (10 mg/kg bw for PEGs 200 - 10000). The Panel noted that under the current Community legislation foods for special medical purposes should be used under medical supervision. The supervising physician will be in a position to weigh up any risks and benefits to the patient and to ensure that the patient receives an adequate dose of vitamin E. The Panel noted that studies in healthy humans showed that the administration of TPGS, in contrast to fat-soluble vitamin E sources, only slightly elevated the plasma α-tocopherol level. Therefore, TPGS is not a useful source of vitamin E in healthy humans with a normal fat absorption. The Panel therefore concluded that the use of TPGS in foods for special medical purposes is not of safety concern at the anticipated exposure level. However, the Panel noted that it is advised not to apply the TPGS treatment in children with severe impairment of kidney function. KEY WORDS D-alpha-tocopheryl polyethylene glycol 1000 succinate (TPGS), water-soluble vitamin E, foods for particular nutritional uses, supplement for foods for special medical purposes, vitamin E deficiency, CAS Registry Number 9002-96-4. 1 In this opinion, the term “TPGS-400” is used for d-α-Tocopheryl polyethylene glycol-400 succinate. 2 TPGS in food for special medical purposes EFSA Journal (2007) 490, p. 3 of 20 BACKGROUND The Scientific Committee on Food (SCF) was asked in November 2001 to consider the safety of a number of substances as sources of nutrients for foods for particular nutritional uses (FPNUs). The evaluations could not be completed under the SCF mandate and continuation of this work now falls to the EFSA Scientific Panel on Food Additives, flavourings, processing aids, and materials in contact with food (AFC Panel). Data on polyethylene glycol (PEG) and on D-alpha-tocopheryl acid succinate (TAS) as source of vitamin E are described in separate opinions (EFSA, 2005; EFSA, 2006), and will not be described in detail in this opinion. TERMS OF REFERENCE The Commission asks the European Food Safety Authority (EFSA) to consider the safety and bioavailability of the nutrient source d-α-tocopheryl polyethylene glycol 1000 succinate (TPGS) proposed for use in foods for particular nutritional purposes. ASSESSMENT Chemistry d-α-Tocopheryl polyethylene glycol-1000 succinate (TPGS) is a “water-soluble” source of vitamin E. It is formed by the esterification of polyethylene glycol 1000 with d-α-tocopheryl succinate. Chemically it is a mixture composed principally of the monoesterified polyethylene glycol 1000 (70-87 %), the diesterified polyethylene glycol 1000 (<12 %), free polyethylene glycol 1000 (<12 %), and free tocopherol (<1.5 %). A typical sample contains 27 % d-alpha-tocopherol, 65 % polyethylene glycol 1000 and 8 % succinic acid and has a total alpha-tocopherol potency of 260 mg/g TPGS (387 IU/g), after saponification of the esters. The chemical name is 2R,4’,8’R, αtocopheryl polyethylene glycol 1000 succinate; and the CAS registry number is 900296-4. Since the molecular weight of polyethylene glycol is 1000, the molecular weight of TPGS is calculated to be approximately 1513 Daltons. The molecular formula is C33 O5 H54 (CH2 CH2 O)n, where "n" represents the number of polyethylene oxide moieties attached to the acid group of d-alpha tocopheryl succinate. 3 TPGS in food for special medical purposes EFSA Journal (2007) 490, p. 4 of 20 TPGS can be identified by Fourier transform infrared spectrometry (FT-IR). Properties and proposed specifications Appearance: Waxy solid, white to light brown; Identity: Measured by FT-IR spectroscopy; Potency: 260-300 mg d-α tocopherol/g (after saponification of the ester); Acid value: Not more than 1.5 %; Colour: Not more than 10 (Gradner scale); Specific rotation: Not less than +24. Purity TPGS is composed principally of the monoesterified polyethylene glycol 1000 (70-87 %), the diesterified polyethylene glycol 1000 (<12 %), free polyethylene glycol 1000 (<12 %), and free tocopherol (<1.5 %). The composition can be measured by HPLC using a light scattering detector. Impurities The petitioner mentions that possible impurities may include: Oxidised TPGS monoester Succinic acid ester of TPGS monoester PEG ester impurity of succinic acid ester of TPGS Propionate ester of TPGS monoester Methyl ester of tocopheryl succinate Ethyl ester of tocopheryl succinate Diester of succinic acid with TPGS monoester Alpha-tocopherol succinate Campesterol ester of tocopheryl succinate Sitosterol ester of tocopheryl succinate Other sterol ester of tocopheryl succinate Heavy metals determined as lead: Upper limits 0.6% 1.5% 0.25% 1.5% 0.25% 1.5% 0.5% 0.25% 0.5% 0.5% 0.5% not more than 10 mg/kg 4 TPGS in food for special medical purposes EFSA Journal (2007) 490, p. 5 of 20 Manufacturing process No information on the manufacturing process has been made available. Method of analysis in food The level of vitamin E can be determined in foods by HPLC. Information on analysis of TPGS in food was not provided by the applicant. Reaction and fate in food, stability Stability tests have been carried out on a food for special medical purposes for a patient with liver disease. The product was a powdered nutritionally complete food with whole proteins and added TPGS. The vitamin E content slowly decreased from 120 mg/100 g food to 117 mg/100 g after 9 months and 109 mg/100 g after 24 months. This demonstrates the stability of TPGS in this food matrix. TPGS is unstable in aqueous solution under extreme acidic and alkaline conditions, due to hydrolysis of the ester linkages. However, it is unlikely that the manufacture, processing, or composition of a food for special medical purposes would lead to such conditions. TPGS can also react with strong oxidising agents. Case of need and proposed uses TPGS is added to foods for special medical purposes (FSMP), which are used to provide nutritional support or supplementary feeding for infants and young children with acute and chronic liver disease. Children with (chronic liver) disease are at high risk of malnutrition, especially in cholestatic liver disease when onset is in infancy. The prevalence of malnutrition among these children is significant (Sokol et al. 1990; Beath et al. 1993; Holt et al., 1997). Vitamin E absorption is adversely affected by bile salt deficiency and pancreatic insufficiency. Vitamin E malabsorption and deficiency occur in up to 60-70 % of children with prolonged forms of neonatal cholestatis leading to a degenerative neurological disorder if the deficiency persists past 18-24 months (Argao et al., 1993). Correction of the deficiency before the age of 3 years reverses or prevents the development of neuromuscular symptoms. TPGS does not require the action of bile salts or pancreatic enzymes for absorption into the intestinal wall (Traber et al., 1986; Traber et al., 1988). TPGS is intended to be used as a source of vitamin E in FSMP in conditions where insufficient amounts of bile are secreted, such as in cholestatic liver disease, or where insufficient amounts of pancreatic enzymes are secreted, such as in cystic fibrosis (Sokol et al., 1987a,b, Sokol et al., 1993). However, as the presence of secreted bile salts appear to inhibit the absorption of water miscible forms of vitamin E, such as TPGS (Dimitrov et al., 1996), it is not advisable to use TPGS in individuals with preserved lipid absorption and normal vitamin E homeostasis (Sokol et al., 1987a,b). The FSMPs in which TPGS is to be used will be powdered, liquid, or solid forms as appropriate. TPGS has practically no taste and lacks bitterness; this makes it especially suitable for oral use. 5 TPGS in food for special medical purposes EFSA Journal (2007) 490, p. 6 of 20 TPGS is currently used as a 20% aqueous solution (20% of TPGS by weight or 77.4 IU vitamin E/ml of solution) (Sokol et al., 1993; Socha et al., 1997; Collnot et al., 2006). According to the petitioner, the estimated maximum level of TPGS added to a nutritionally complete food for special medical purposes is approximately 58 mg/100 g product. This has been calculated, based on the maximum level of 0.75 mg vitamin E/100 KJ food permitted according to Directive 1999/21/EC on dietary foods for special medical purposes and the energy content of pre-existing nutritionally complete foods used for patients with liver diseases. TPGS contains 27 % d-α-tocopherol and each gram of TPGS contains 387 IU (260 mg) d-α-tocopherol. Exposure As TPGS is a synthetic source of vitamin E to be used as FSMP only there will be no contribution from the rest of the diet. The estimated intake to TPGS has been calculated based on the maximum use level of 0.75 mg vitamin E/100 KJ food permitted according to Directive 1999/21/EC on dietary foods for special medical purposes. On this basis the potential intake will be highest in infants when the energy intake per kg body weight is highest. The potential intakes to TPGS were estimated in male infants, children, and teenagers based on the estimated energy requirement and average body weight as reported by the Scientific Committee for Food (SCF, 1993) and based on the assumption that each gram of TPGS contains 27% d-α-tocopherol (see Table 1). The estimated potential intake varies from 5 mg TPGS /kg bw/day in teenagers to 13 mg TPGS /kg bw/day in 1 month old infants. Table 1. Estimated potential exposure to TPGS from use in foods for special medical purposes in infants, children and teenagers. Age Estimated energy requirement KJ/day(*) 1 month 6 month 12 month 24 month 36 month 6-7 years 10-11 years 14-15 years 17-18 years 1900 3200 4000 5000 6000 7700 8730 10890 12000 Average body weight (kg)(*) 4 8 10 12.5 15 22 33 53 64.5 Estimated dietary exposure (mg vit. E/day) Estimated dietary exposure to TPGS (mg/day) Estimated dietary exposure to TPGS (mg /kg bw /day) 14.25 24 30 37.5 45 57.75 65.5 81.7 90 54.9 92.4 115.5 144.4 173.3 222.4 252.2 314.6 346.5 13 11 11 11.5 11.5 10.1 7.6 5.9 5.4 (*) as reported in SCF (1993) for males 6 TPGS in food for special medical purposes EFSA Journal (2007) 490, p. 7 of 20 Biological and toxicological data Bioavailability of d-α-tocopherol from TPGS In vitro studies When human fibroblasts, erythrocytes and human intestinal cells (from a cell line) were incubated with TPGS, the total cellular tocopherol content increased (Traber et al., 1988; Carini et al., 1990). The results suggest that addition of the hydrophobic molecule tocopherol to polyethylene glycol 1000 leads to the formation of micelles that readily pass through cell membranes, and that TPGS enters the cells unchanged where it is then hydrolysed enzymatically to release free tocopherol (Traber et al., 1988). The use of TPGS as an oral absorption enhancer has been discussed by Collnot et al. who studied the influences of the PEG chain length in TPGS on apical efflux transporters in Caco-2 cell monolayers by measuring rhodamine 123 transport at different chain length. An inverse relationship between chain length and the efficiency of the transport was observed (Collnot et al., 2006). However, it remains to be established whether such an effect also occurs in vivo. Animal studies Traber et al. (1986) performed an absorption study of vitamin E in water miscible forms in thoracic duct-cannulated cats. It was concluded that TPGS delivers α-tocopherol to enterocytes in the absence of bile salts. As α- or γ-tocopherols normally require the presence of bile salts to be absorbed the authors proposed a hypothesis for the mechanism of enhanced α-tocopherol absorption from TPGS on the basis of TPGS micelles formation. Human studies Traber et al. (1986) performed a trial with an 8-year-old patient who had suffered neurological hallmarks of vitamin E deficiency, including loss of muscle coordination. The trial was performed using either tocopheryl acetate emulsified with medium-chain tri-glycerides and polysorbate 80 (known as MCT-E) or TPGS. The results showed higher concentrations of tocopherol in plasma, erythrocytes, and adipose tissues, and thus better bioavailability after administration of TPGS than after administration of MCT-E. Sokol et al. (1987a) studied the bioavailability of d-α-tocopherol from TPGS in 22 children (7 months to 19 years) with severe cholestasis and vitamin E deficiency who were unresponsive to massive oral doses (100 to 200 IU/kg/day) of dl-α -tocopherol. The results showed that the bioavailability of d-α-tocopherol from TPGS was superior to that from d-α-tocopherol alone in these children. An oral dose of 15-25 IU vitamin E/kg body weight per day from TPGS corrected the vitamin E deficiency state over 1 - 19 months (mean 10.6 months). Sokol et al. (1985) had previously shown that long-term correction of vitamin E deficiency by intramuscular administration of dl-α-tocopherol improved the neurological function in 14 children with chronic cholestasis. Therefore, Sokol et al. 7 TPGS in food for special medical purposes EFSA Journal (2007) 490, p. 8 of 20 (1987b) also studied the effect of oral TPGS administration on the neurological function in 12 children with prolonged neonatal cholestasis and with vitamin E deficiency (aged 9 months to 6 years). Administration of 15 - 25 IU/kg bw/day from TPGS for a mean of 19.3 months normalised the biochemical serum indices of vitamin E status and was well tolerated by all patients. The neurological functions as assessed by serial neurological examinations remained normal in the two children younger than 3 years at the onset of the study without neurological symptoms, improved in six of seven children with neurological symptoms and younger than 3 years at onset of the study, and improved in all three children older than 3 years with neurological symptoms at study start. Traber et al. (1994) performed a 3 year supplementation study with orally administered TPGS in a male 71-year old patient suffering from Crohn’s disease. The supplementation was adjusted twice during the three-year period. Initially, liquid TPGS was administered with meals. The patient consumed variable amounts of the preparation, namely 4000 IU/day (10.3 g TPGS/day; 387 IU vitamin E/g TPGS ) at least four times per week (as stated by the patient) and no less than 1250 IU/day (3.2 g TPGS/day) for the remainder of the week. After 100 weeks of supplementation, a commercially available preparation of encapsulated solid TPGS was tested in order to make the vitamin E supplementation more convenient for the patient. Capsules were given for 4 months at an average of 2500 IU/ day (6.4 g TPGS/day). As the plasma αtocopherol remained unacceptably low, supplementation with liquid TPGS was reinstated at a dose of 4000 IU/day until the test period was finished at week 173. After this treatment the patient had normal plasma alpha-tocopherol concentrations. Administration of deuterium-labelled TPGS to this patient demonstrated that TPGS was absorbed and the released alpha-tocopherol was transported in lipoproteins. The disappearance curves of the deuterated alpha-tocopherol in plasma, red cells and lipoproteins were parallel to those seen in control subjects, suggesting normal metabolic turnover of the absorbed α-tocopherol. A trial with TPGS was performed to determine the long-term efficacy in increasing the vitamin E bioavailability (duration varying from 2 months to 7 years) and safety of TPGS in children with chronic cholestasis. Sixty vitamin E deficient children (aged 0.5-20 years) with chronic cholestasis and unresponsive to 70-212 IU/kg bw/day of oral vitamin E entered a trial with TPGS. After an initial evaluation, the treatment was started with 25 IU Vitamin E/kg body weight per day from TPGS. Vitamin E status and neurological function quantified by a specific scoring system were monitored during the study. All children responded to TPGS with normalisation of vitamin E status. The neurological function, which had deteriorated before entry into the trial, improved in 25, stabilized in 27, and worsened in only 2 children after a mean of 2.3 years of treatment. It was concluded by the authors that orally supplemented TPGS at a level of 20-25 IU vitamin E/kg bw/day appears to be an effective form of vitamin E for reversing or preventing vitamin E deficiency during chronic childhood cholestasis (Sokol et al., 1993). Socha et al. (1997) studied the effects of long-term TPGS supplementation (1 year) in 15 children aged from 9 months to 3.4 years (median 1.3 years), having chronic cholestasis with low serum vitamin E concentrations (median 1.95 mg/L with range 0.8 - 3.7 mg/L). The previous supplementation of alpha-tocopherol was replaced by a 8 TPGS in food for special medical purposes EFSA Journal (2007) 490, p. 9 of 20 20 % solution of TPGS, given as one daily dose of 20 IU vitamin E/kg body weight. Serum α-tocopherol was measured at baseline and again after 1 month in all 15 children and after 1 year in 11 children. Median α-tocopherol levels were significantly increased after 1 month (median 6.9 mg/L with range 4.4-8.4 mg/L) and rose further after 1 year (median 9.7 mg/L with range 7.2-14.9 mg/L); similar results were obtained for the ratio vitamin E/total lipids. It was concluded by the authors that oral TPGS supplementation of cholestatic children can quickly normalise serum vitamin E levels. In a study in healthy human subjects, plasma α-tocopherol concentrations were determined after supplementation with water- or fat-soluble vitamin E. Administration of various amounts of TPGS (400 IU [269 mg], 800 IU [537 mg] and 1200 IU [807 mg] ) were applied either as single doses or as repeated doses during 4 weeks. TPGS given as a single dose resulted in a slight elevation of the plasma α-tocopherol concentration. The repeated administration of TPGS revealed also a slight elevation of the α-tocopherol plasma concentration, whereas the administration of fat-soluble vitamin E led to a significant increase of the plasma α-tocopherol concentration (Dimitrov et al., 1996). These studies show that the bioavailability of Vitamin E from TPGS is low in normal healthy humans. Absorption, metabolism, distribution, and excretion Animal studies The absorption, distribution and excretion of polyethylene glycol 1000 (PEG 1000) from TPGS in rats were evaluated in two studies conducted by Beilman et al. (1988a,b). A third study conducted concurrently evaluated the absorption, disposition and excretion of pure PEG 1000 (Beilman et al., 1988c). In the first study (Beilman et al., l988a) six male rats were gavaged with 360 mg TPGS/kg bw, containing 10 μCi of [14C]-labelled PEG 1000. Urine, faeces, and cage washings were collected at 12, 36 and 60-hours post-exposure. The animals were killed after 60 hours and tissues and carcasses were collected for analysis of residual radioactivity. A total of 91 % of the radioactivity administered was recovered. The largest amount (77%) was recovered in the faeces, with 31 % collected in the first 12 hours and 40% in the 12— 36 hours period. A total of 13 % was found in urine with almost 90% of this fraction (11.5 %) collected during the first 12 hours; cage washings accounted for a total of 0.8%. On average, 0.6% was identified in the body with most of this being present in the stomach (0.1 %) and large intestine (0.1 %), In the second study, animals were divided into 7 groups of 3 animals each and administered a single gavage dose of 60 mg TPGS/kg bw containing 10 μCi of [14C]labelled PEG 1000. Animals were then killed at 0, 1, 3, 6, 12, 24, and 48 hours post dosing. In addition to faeces and urine, the following tissues were analysed for radioactivity at each time point: blood, stomach, small intestine, large intestine, heart, lung, liver, spleen, kidney and brain. Almost all the radioactivity was eliminated from the stomach within 1 hour and with 1% remaining after 6 hours. The radioactivity largely disappeared from the small intestines between 3-6 hours with 2 % remaining at 24 hours and 0.6 % after 48 hours. Fecal elimination was not complete until after 24 hours by which time cumulative totals exceeded 72 % of the dose. Apparent transit times in the stomach, small intestine and large intestine were 1, 11 and 21 hours, 9 TPGS in food for special medical purposes EFSA Journal (2007) 490, p. 10 of 20 respectively only traces of radioactivity could be found in other tissues examined, with the liver accounting for the highest levels measured after 6 hours. Most of the radiolabel was again located in the faeces with 85.3 % recovered after 24 hours. These results are similar to those obtained in the previous study, demonstrating rapid and predominantly faecal elimination of the radiolabelled material from the body (Beilman et al., 1988 b). In the third study by Beilman et al. (1988c) six male rats were orally gavaged with 240 mg PEG 1000/kg bw corresponding to 10 μCi of [14C]-labelled PEG 1000 by gavage. Urine and faeces were collected at 12, 36 and 60 hours post-exposure, while cage washings were collected at 12 and 36 hours. The animals were killed after 60 hours and tissues and carcasses were collected for analysis of residual radioactivity. The largest amount of radioactivity, 95.3 %, was recovered in the faeces with 68.4 % collected in the first 12 hours and 26.1 % in the 12 —36 hour period. Less than 1 % was recovered after 36 hours. A total of 6.7 % was excreted in urine with 6.2% collected during the first 12 hours. Cage washings accounted for a total of 0.3 % of radioactivity. No residual radioactivity was found in any of the examined tissues. These results demonstrated that an oral exposure to PEG 1000 is rapidly eliminated, with faeces being the primary route of excretion and that a minimum of 6.7 % of PEG may be absorbed under these conditions (reflected in the excretion in urine after 36 hours). Human studies In the study by Sokol et al. (1987a) in 22 children (7 months to 19 years) with severe cholestasis and vitamin E deficiency given chronic oral doses of 15-25 IU vitamin E/kg body weight per day from TPGS it was also shown that absorption of PEG 1000 from TPGS in teenage children with chronic cholestasis was similar to that in normal adults. Thus, 1.7% ± 1.6% of the administered PEG 1000 contained in the TPGS was excreted in the urine of the 13 persons analysed by HPLC method, compared with 3.0 % ± 1.3 % in 4 normal adults. Although only a small amount (less than 5 %) of PEG 1000 contained in the TPGS appeared to be absorbed and readily excreted in the urine, Sokol et al. (1987 a,b) considered that at high dose levels of TPGS there is a possibility of the induction of a hyperosmolar state if TPGS is administered during renal insufficiency or dehydration, since excretion of the PEG 1000 relies completely on glomerular filtration and urinary excretion. Therefore, the authors recommended that TPGS should not be administered in children with significant renal insufficiency. Interaction with other dietary components TPGS can form micelles and pass through cell membranes (Argao et al., 1992). As no binding proteins or carriers are required for its uptake into the intestinal cells, it is unlikely that it has to compete with other nutrients and there is no evidence to suggest that TPGS will adversely affect the absorption of other nutrients. There is, however, evidence that TPGS can enhance the absorption of fat-soluble molecules (Argao et al., 1993). 10 TPGS in food for special medical purposes EFSA Journal (2007) 490, p. 11 of 20 Toxicological data Acute toxicity The acute oral toxicity of TPGS was evaluated in mature and neonatal (2 day old) rats (Krasavage and Terhaar, 1977). No mortalities were induced by TPGS in adult animals (l0/sex) exposed to a single oral dose of 7,000 mg/kg bw in corn oil. In male neonatal rats mortality rates of 6/17 (35 %), 7/15 (47%) and 10/15 (67 %) were seen after single doses of 1899, 2981 and 4478 mg TPGS/kg bw, respectively. However, no LD50 was calculated due to many deaths caused by gavage errors. In other oral exposure studies no mortalities, gross necropsy findings or clinical signs were noted in rats following single exposure to 4000 or 5000 mg TPGS/kg bw or higher (Ludwig and Ames, 1959; Shepard, 1989). In Beagle dogs (2 males), the only abnormal clinical sign following oral gavage of TPGS (2,000 mg/kg bw) was loose stools the morning on the day after its administration (SRICC, 1999a). Subchronic toxicity Groups of rats (6/sex/dose) were fed diets containing TPGS at levels of approximately 0, 1, 2, 4, 8, and 16% (equivalent to 0, 500, 1000, 2000 and 4000 mg TPGS/kg bw/day). After 10 weeks the animals fed the 8 and 16% TPGS diets were sacrificed and their tissues examined microscopically while the remainder animals continued on their diets for a total of 60 weeks. After 10 weeks no differences were observed in food consumption and weight gains between the controls and treated groups. No significant findings associated with TPGS exposure were noted during gross (all animals) and microscopic analyses (2/sex) of the 2 treated groups. Following 60 weeks of exposure, mortalities were 7/12, 5/12, 2/12 and 7/12 in the 0, 500, 1000 and 2000 mg TPGS/kg bw/day groups, respectively. All animals were noted to be suffering from respiratory infections. No significant findings attributable to TPGS exposure were noted between controls or any of the three treated groups during gross and microscopic analyses (Ludwig and Ames; 1959). A 91-day toxicity study was conducted in rats (30/sex/dose) with TPGS present in the diet at levels of 0.002, 0.2 and 2.0 % ( equivalent to 1.0 100 and 1000 mg TPGS/kg bw/day for males and 1.14, 116 and 1108 TPGS/kg bw/day for females ) (Krasavage and Terhaar, 1977). The study included analyses of clinical signs, body weights, food consumption, haematology (an additional haematological examination was done at day 42 on high-dose and control animals), serum biochemistry, urinalysis, organ weights and macro- and microscopic evaluations on a comprehensive list of tissues selected for complete necropsies. No consistent treatment related effects were observed in the study. It was concluded that the NOAEL was 2% TPGS in the diet. This is approximately equivalent to 1000 mg TPGS kg bw/day for males and females, respectively, the highest doses tested. A one-year oral gavage study in rats (25/sex/dose level) was conducted with TPGS administered in deionised water at 0, 100, 300 and 1,000 mg/kg bw/day (NCI, 1994a). The study included clinical observations, measurement of body weights and food consumption, ophthalmoscopical signs, haematology, serum biochemistry, urinalysis, 11 TPGS in food for special medical purposes EFSA Journal (2007) 490, p. 12 of 20 determination of organ weights and macro- and microscopic evaluations on a comprehensive number of tissues. All animals survived to the end of the study and no treatment-related findings were noted at any exposure level. The NOAEL was concluded to be 1,000 mg/kg bw/day, the highest dose tested. A similar one-year study was conducted in dogs (4/sex/dose) using essentially identical methodology and dose levels (NCI, 1994b). In this study two intercurrent deaths were seen, which were not related to the TPGS treatment. No treatment related effects were noted in any parameter examined and the NOAEL was concluded to be 1,000 mg/kg bw/day, the highest dose tested. Reproductive and developmental toxicity A one-generation, two litter reproduction and teratology study (Krasavage and Terhaar, 1977 was conducted in rats (15/sex/dose) exposed to TPGS in their diets at levels of 0.002, 0.2, and 2.0 % (equivalent to approximately 1.0, 100 and 1000 mg TPGS/kg bw/day). The females, designated F0, were mated with treated males after 112 days of TPGS exposure to produce the F1a litters. The F0 -females were mated again (using different males) after 175 days of exposure to produce F1b offspring. The F1 animals were maintained on test diets for 5 weeks post-weaning and 4 animals (2/sex) from each litter were randomly chosen for microscopic analysis of their tissues. Haematological analysis was performed on the high dose and control F0 animals 2 weeks prior to study termination and complete histological examinations were performed. These animals had been maintained on the test diets for a total of 265-268 days. The reproductive parameters examined were insemination index, fertility index, gestation index, viability index and lactation index. In addition, the mean gestation period, litter size, sex ratio, pup and parent mortalities, and the mean body weights of the pups per litter at four days of age, at weaning and at one and two weeks after weaning were recorded. The results showed that the exposure to TPGS did not induce alterations in any of the reproductive parameters studied and similarly, no indications of toxicity were noted. The NOAEL was concluded to be 2% in the diet, equivalent to approximately 1500 mg TPGS/kg bw/day, the highest dose level tested. Groups of 15 pregnant rats received diets containing 0, 0.002, 0.2, and 2.0% of TPGS (equivalent to approximately 0, 1.0, 100, 1000 mg TPGS/kg bw/day). The test diets were given on days 6 to 17 of gestation and the animals were killed on day 20. The parameters studied included total implantation sites, resorptions, and total number, weight and sex of live fetuses. All fetuses were examined for external abnormalities and half of them were fixed and dissected for soft tissue evaluations. Gross anomalies seen in only two fetuses from the TPGS-treated groups were considered by the authors to be spontaneous and not attributable to the ingestion of TPGS. Thus, the maternal and developmental NOAEL for dietary TPGS was 2.0% TPGS in the diet, equivalent to approximately 1000 mg TPGS/kg bw/day, the highest dose level tested (Krasavage and Terhaar, 1977). In a second rat study, the effect of TPGS on embryo-fetal, pre- and post-natal development, and maternal function was assessed. TPGS was administered from the time of implantation to weaning by oral gavage at doses of 100, 300 or 1,000 mg/kg bw/day. The parameters evaluated in the dams included clinical observations, body 12 TPGS in food for special medical purposes EFSA Journal (2007) 490, p. 13 of 20 weight changes and food consumption. The fetuses and offspring were assessed for external and visceral and skeletal changes, viability, clinical observations, body weight changes, postnatal development, reflex responses in open field performance, learning ability, and reproductive ability of the offspring. No effects due to TPGS exposure were noted in any endpoints in either the dams or their offspring at 1000 mg/kg bw/day. Thus the NOAEL was 1000 mg TPGS/kg bw/day, the highest dose level tested (SRICC, 1999d). Developmental toxicity of TPGS was also assessed in rabbits (SRICC, 1999b,c). The test material was administered by oral gavage at doses of 100, 300 or 1000 mg/kg bw/day on days 6 -18 of gestation in a preliminary study and in the main study. In the preliminary study soft faeces, decreased food consumption and a concomitant decrease in body weight gain was observed in the dams at the highest dose. These effects were not observed in the main study. No treatment related effects were observed at any dose in external, visceral or skeletal examinations of the fetuses. The NOAEL for fetal effects was 1000 mg/kg bw/day, the highest dose level tested. Chronic toxicity and carcinogenicity No chronic toxicity and carcinogenicity studies are available on TPGS. However, recent limited carcinogenicity studies (only one dose group) in mice and rats are available on a structurally closely related compound, “TPGS-4002” containing PEG 400 instead of PEG 1000. Crl:CD-1 (ICR) BR VAT plus mice and Han Wistar (Glx:HAN, WlfBR) rats (30 animals/sex/group) were dosed with aqueous solutions of “TPGS-400” at dose levels of 1131 and 1414 mg/kg bw/day by oral gavage 7 days a week, respectively. Similar groups of animals received deionised water as controls. The duration of the experiments were 104 weeks. Survival, clinical signs of toxicity, and body weights were recorded during the course of the study. Haematology and macroscopical and microscopical examinations of tissues were performed on all animals. “TPGS-400” had no effects on these parameters and did not increase the tumour incidences in either species (Serota and Slone, 2003a, 2003b). Genotoxicity TPGS was tested for reverse mutations in Salmonella typhimurium strains TA98, TA 100, TA 1535 and TA 1537 and Escherichia coli WP2uvrA with or without metabolic activation by the pre-incubation method. Two independent studies were conducted using up to 5,000 μg/plate. No increases in revertant colonies were seen (SRICC, 1998a). TPGS did not induce chromosomal aberrations in Chinese hamster lung cells at concentrations of 25 to 200 μg/ml, 10 to 80 μg/ml, or 7.5 to 60 μg/ml TPGS for 6, 24 and 48 hours, respectively, without metabolic activation. Similar results were seen following a 6-hour incubation in concentrations up to 1,600 μg/ml with metabolic activation (SRICC, 1998b). 2 In this opinion, the term “TPGS-400” is used for d-α-Tocopheryl polyethylene glycol-400. 13 TPGS in food for special medical purposes EFSA Journal (2007) 490, p. 14 of 20 In an in vivo micronucleus assay, rats were administered TPGS by oral gavage at single doses up to 2,000 mg/kg body weight. Bone marrow preparations were made 24 hours after dosing. There was no difference in the frequency of micronuclei or in the ratio of polychromatic erythrocytes to normochromatic erythrocytes between the treated groups and the negative control group (SRICC, 1998c). Human data In the study by Sokol et al. (1987a) in 22 children (7 months to 19 years) with severe cholestasis and vitamin E deficiency, oral doses of 15-25 IU vitamin E/kg body weight per day, equivalent to 38.8 –64.6 mg TPGS/kg bw per day, did not produce clinical or biochemical evidence of gastrointestinal, renal, hepatic, or haematological toxicity In the study by Sokol et al. (1993) where 60 vitamin E deficient children (aged 0.5-20 years) with chronic cholestasis were given 25 IU vitamin E/kg body weight per day from TPGS (duration varying from 2 months to 7 years) clinical and biochemical parameters (serum bilirubin, aspartate amino-transferase (ASAT), alanine aminotransferase (ALAT), alkaline phosphatase (AP) and cholesterol concentrations) were monitored throughout the study. No adverse effects related to the TPGS administration were observed as judged by these parameters and the authors concluded that oral administration of TPGS at a level of 20-25 IU/kg bw/day, equivalent to 64.6 mg TPGS/kg body weight per day appears to be safe in children suffering chronic cholestasis (Sokol et al., 1993). Socha et al. (1997) studied the effects of TPGS supplementation for one year on lipid peroxidation and polyunsaturated fatty acid status in serum from 15 children aged from 9 months to 3.4 years (median 1.3 years). TPGS was given as a daily dose of 20 IU vitamin E/kg body weight, equivalent to 51.7 mg TPGS/kg body weight per day. Plasma lipid peroxidation expressed as thiobarbituric acid-reactive substances concentration (TBARS) and plasma phospholipid fatty acid profile were estimated at baseline and after 1 month in all 15 children, and after one year in 11 children. TBARS concentrations were significantly higher in cholestatic children at baseline than in the control group, but did not change significantly during the TPGS administration. Compared with the controls, the contributions from polyunsaturated fatty acids to total phospholipid fatty acids were markedly decreased in cholestatic patients at baseline, but did not show major changes after one year of TPGS supplementation. Bilirubin, alanine amino-transferase (ALAT), alkaline phosphatase (AP) and gamma-glutamyl transferase (gamma-GT) were higher in the cholestatic children than the reference values but did not further increase during the one year treatment with TPGS. It was concluded by the authors that oral TPGS supplementation did not alter the increased lipid peroxidation and poor polyunsaturated fatty acid status in cholestatic children. DISCUSSION D-α-tocopheryl polyethylene glycol 1000 succinate (TPGS) is a “water soluble” vitamin E source, in contrast to other vitamin E sources, which are lipophilic. TPGS is intended to be used in patients (mainly infants and children) with impaired vitamin E 14 TPGS in food for special medical purposes EFSA Journal (2007) 490, p. 15 of 20 absorption due to fat malabsorption. The bioavailability of vitamin E and its other lipid-soluble sources depends on fat absorption and therefore requires bile acids and pancreatic enzymes to be present. Conditions where insufficient bile is secreted such as cholestatic liver disease or where insufficient pancreatic enzymes are secreted such as cystic fibrosis lead to impaired vitamin E absorption and if not corrected may lead to neurological disorders. TPGS can form micelles and thus is able to pass the waterlayer in the intestine and reach the enterocytes, readily enabling the absorption of the intact TPGS molecule. In vitro studies have shown that TPGS can be hydrolysed in enterocytes to release α-tocopherol and bioavailability studies in patients with cholestatic liver disease have shown that TPGS administration can correct impaired vitamin E bioavailability. However, studies in normal healthy humans showed that administration of TPGS, in contrast to fat-soluble vitamin E sources, only slightly elevated plasma α-tocopherol. Therefore, TPGS is not a useful source of vitamin E in normal, healthy humans. Several ADME studies in rats using TPGS radiolabeled in the polyethylene glycol 1000 (PEG 1000) moiety showed that radioactivity was to some extent absorbed and distributed throughout the body. The administered radioactivity was readily eliminated, mainly in faeces (about 72-85% in 24 hours) and urine (7-13% in 24 hours). After 60 hour no residual radiolabel was found in any tissues. In teenage children with chronic cholestasis 1.7% of the administered PEG 1000 contained in the TPGS was excreted in the urine, compared with 3.0 % in normal adults. This showed that the systemic exposure to PEG 1000 from TPGS was not higher in persons with impaired bile secretion than in normal persons and that it was lower than in rats (the main species used for the safety studies on TPGS). This pattern of absorption and excretion of PEG 1000 is consistent with many studies in animals and humans on other PEGs previously evaluated by the Panel (EFSA 2006). Generally, these studies demonstrate that the extent of PEG absorption depends on the molecular weight of the specific polymer, such that more complete absorption has been reported for lower molecular weight PEGs, like PEG 400, while absorption is much more limited in case of heavier PEGs. Once absorbed PEGs are excreted in the urine by glomerular filtration without tubular reabsorption (EFSA 2006). According to some investigators, at high dose levels of TPGS there is a possibility of the induction of a hyperosmolar state if TPGS is administered during renal insufficiency or dehydration, since excretion of the PEG 1000 relies on glomerular filtration and urinary excretion. Therefore, the authors recommended that TPGS should not be administered to children with significant renal insufficiency. As TPGS does not have to compete for transport carriers no interaction with other nutrients are known. If tocopheryl acid succinate were formed by hydrolysis, the absorption by individuals with fat malabsorption would be negligible. The studies combining bioavailability, tolerance and the impact of TPGS on neurological effects caused by vitamin E deficiency in patients revealed that no adverse effects of TPGS supplementation were observed at dose levels up to 64.6 mg/kg bw/day 15 TPGS in food for special medical purposes EFSA Journal (2007) 490, p. 16 of 20 The toxicological data reveal that TPGS is of low acute toxicity. Furthermore a number of subchronic toxicity studies, a one-generation reproduction study, and a few developmental studies in rats and one study in rabbits revealed no adverse effects at dose levels equivalent to 1000 mg TPGS/kg body weight per day or higher. Genotoxicity studies of TPGS consisting of one in vitro bacterial (Salmonella and Escherichia coli) test, one in vitro chromosomal aberration test in Chinese hamster lung cells and one bone marrow micronucleus test in rats revealed that TPGS did not have genotoxic properties. The toxicity file also included two limited chronic toxicity and carcinogenicity studies in rats and mice using “TPGS-400” containing PEG-400 instead of PEG-1000 and therefore would be expected to provide a higher systemic exposure to PEG. However, no toxic effects including carcinogenicity was observed in rats and mice after doses of 1131 mg/kg bw/day (mice) and 1414 mg/kg bw per day (rats) for 2 years, respectively. The Panel concluded that in the absence of genotoxic effects the safety of TPGS can be assessed on the basis of the overall NOAEL equivalent to 1000 mg TPGS/kg body weight per day, established in subchronic toxicity studies. TPGS is only to be used for food for special medical purposes under medical supervision at estimated exposure varying from 5 mg TPGS /kg bw in teenagers to 13 mg TPGS /kg bw in 1 month old infants. Potential exposure would be lower in adults. This provides an adequate margin of exposure of 80 to 200. The Panel considered also that in some human studies dose levels up to 64.6 mg/kg bw/day did not reveal any adverse effect in the parameters studied (liver, kidney). The Panel also noted that these estimated intakes to TPGS would correspond to intakes to PEG 1000 at levels equivalent to 3.3 – 8.5 mg/kg bw/day. This is within the range of group ADIs established by the SCF (5 mg/kg bw for PEG 300 - 4000) and JECFA (10 mg/kg bw for PEGs 200 - 10000). The Panel noted that under the current Community legislation foods for special medical purposes should be used under medical supervision. The supervising physician will be in a position to weigh up any risks and benefits to the patient and to ensure that the patient receives an adequate dose of vitamin E. CONCLUSION The Panel therefore concluded that the use of TPGS in foods for special medical purposes is not of safety concern at the anticipated intake level. However, the Panel noted that it is advised not to apply the TPGS treatment in children with severe impairment of kidney function. The Panel noted that studies in healthy humans showed that the administration of TPGS, in contrast to fat-soluble vitamin E sources, only slightly elevated the plasma α-tocopherol level. Therefore, TPGS is not a useful source of vitamin E in healthy humans with a normal fat absorption. 16 TPGS in food for special medical purposes EFSA Journal (2007) 490, p. 17 of 20 DOCUMENTATION PROVIDED TO EFSA Submission to SCF for the safety evaluation of D-alpha-tocopheryl polyethylene glycol 1000 succinate and additional detailed data further sent to EFSA on request. Dossier submitted by SHS International Ltd on behalf of IDACE. REFERENCES Argao, E A, Heubi, J E, Hollis, B W and Tsang, R C (1992) D-α-Tocopherol polyethylene glycol-1000 succinate enhances the absorption of vitamin D in chronic cholestatic liver disease of infancy and childhood. Pediatric Research 31 (2) : 146-150 1992 Argao, E.A. and Heubi, J.E. (1993). Fat-soluble vitamin deficiency in infants and children. Current Opinion in Pediatrics, 5, 5623 –566. Beath, S.V., Brook, G., Kelly, D.A. et al., (1993) Succesful liver transplantation in babies under one year, British Medical Journal, 307, 825-828.Carini, R., Poli, G., Dianzani, M.U., Collnot, E.M., Baldes, C., Wempe, M.F., Hyatt, J., Navarro, L., Edgar, K.J., Schaefer, U.F. and Lehr,C-M. (2006). Influence of vitamin E TPGS poly(ethyleneglycol) chain length on apical efflux transporters in Caco-2 cell monolayers. J.Controlled Release, 111, 35-40. Dimitrov, N.V., Meyer-Leece, C., Mcmillan, J., Gilliland, D., Perloff, M. And Malone, W. (1996). Plasma α-tocopherol concentrations after supplementation with water- and fat-soluble vitamin E. Am.J.Clin Nutr., 64, 329-335. EFSA (2005) Opinion of the AFC Panel related to D-α-tocopheryl acid succinate as a source of vitamin E in foods intended for the general population, food supplements and foods for particular nutritional uses. Question Nr. EFSA-Q-2003-074.Adopted on 26 April 2005 The EFSA Journal, 203, 1-16 http://www.efsa.europa.eu/en/science/afc/afc_opinions/925.html EFSA (2006). Opinion of the Scientific Panel on Food Additives, Flavourings, Processing Aids and Materials in Contact with Food on a request from the Commission related to an application on the use of polyethylene glycol (PEG) as a film coating agent for use in food supplement products. Question No EFSA-Q-2005277. Adopted on 28 November 2006. The EFSA Journal, 414, 1-22. http://www.efsa.europa.eu/en/science/afc/afc_opinions/ej414_polyethyleneglycol.html Holt R.I., Broide, E., Buchanan.C.R. et al., (1997). Orthotopic liver transplantation reverses the adverse nutritional changes of end-stage liver disease in children. American Journal of Clinical Nutrition, 65, 534-542. Krasavage, W.J. and Clarence J. Terhaar. (1977). D-α-tocopheryl poly(ethylene glycol) 1000 succinate. Acute toxicity, subchronic feeding, reproduction and teratology studies in the rat. J. Agric. Food Chem., 25, 273 – 278. 17 TPGS in food for special medical purposes EFSA Journal (2007) 490, p. 18 of 20 Ludwig, M.I., Ames, S.R. (1959). The physiological activity of d-alpha-tocopheryl polyethylene glycol 1000 succinate . laboratory report number 665, December 18, 1959. Distillation Products Industries, Division of Eastman Kodak Campany, Rochester, NY, USA. SCF, EC Scientific Committee for Food (1993). Nutrient and energy intakes for the European Community. Reports of the Scientific Committee for Food (Thirty-first series). European Commission, Luxembourg. Available at http://ec.europa.eu/food/fs/sc/scf/out89.pdf Shepard, K.P. Acute toxicity of vitamin E TPGS., HAEL No. 89-0117, November 28, 1989. Toxicological Sciences Laboratory, Health and Environment Laboratories, Eastman Kodak Caompany, Rochester, NY, USA. Socha, P., Koletzko, B., Pawlowska, J., Proszynska, K. And Socha, J. (1997). Treatment of cholestatic children with water-soluble vitamin E (α- tocopherol polyethylene glycol succinate): Effects on serum vitamin E, lipid peroxides, and polyunsaturated fatty acids. J. Pediatric Gastroenterology and Nutrition, 24, 189 –193. Sokol, R.J., Guggenheim. M., Iannacone, S.T., Barkhaus, P.E., Miller, C.V., Balistreri, W.F. and Heubi, M.D. (1985). Improved neurological function after longterm correction of vitamin E deficiency in children with chronic cholestasis. The New England Journal of Medicine, 313, 1580-1586. Sokol, R.J., Heubi, J.E., Butler-Simon, N.A., McClung, H.J., Lilly, J.R. and Silverman, A. (1987a). Treatment of vitamin E deficiency during chronic childhood cholestasis with oral d-α-tocopheryl polyethylene glycol-1000 succinate. Gastroenterology, 93, 975-985. Sokol, R.J., Butler-Simon, N.A., Bettis, D, Smith, D.J. and Silverman, A. (1987b). Tocopheryl polyethylene glycol 1000 succinate therapy for vitamin E deficiency during chronic childhood cholestasis: Neurologic outcome. J. Pediatr., 111, 830-836. Sokol, R.J. and Stall, C. (1990). Anthropometrics evaluation of children with chronic liver disease. American Journal of Clinical Nutrition, 52, 203-208. Sokol, R.L., Butler-Simon, N.A., Conner, C., Heubi, J.E., Suchy, F.J., Heyman, M.B., Perrault, J., Rothbaum, R.J., Levy, J., Iannacone, S.T., Shneider, Koch, T.K. and Narkewicz, M.R. (1993). Multicenter trailk of d-α- tocopherol polyethylene glycol 1000 succinate for treatment of vitamin E deficiency in children with chronic cholestasis. Gastroenterology, 104, 1727 – 1735. Traber, M.G., Kayden, H.J., Balmer Green, J. And Green M.H. (1986). Absorption of water-miscible forms of vitamin E in a patient with cholestasis and in thoracic ductcannulated rats. Am. J. Clin. Nutr., 44, 914-923. 18 TPGS in food for special medical purposes EFSA Journal (2007) 490, p. 19 of 20 Traber, M.G., Thelleman, C.A., Rindler, M.J. and Kayden, H.J. (1988). Uptake of intact PTPGS (D-α- tocopherol polyethylene glycol 1000 succinate) a wtaer-miscible form of vitamin E by humans cells in vitro. Am.J.Clin. Nutr., 48, 605-611. Traber, M.G.,Schiano, T.D., Steephen, A.C., Kayden, H.J. and Shike, M. (1994). Efficacy of water-soluble vitamin E in the treatment of vitamin E malabsorption in short-bowel syndrome. Am.J.Clin. Nutr., 59, 1270 – 1274. References which were not published Beilman, J.J., Blakely, R.V. and Stong, D.B. Absorption, disposition and excretion of radioactivity following a single oral dose of tocopherol [14C] polyethylene glycol 1000 succinate in rats (1988a). March 14, 1988, Technical Report # DM8805, Eastman Pharmaceuticals Drug Safety Evaluation. Beilman, J.J., Blakely, R.V. and Stong, D.B. Tissue and excrement distribution following a single oral dose of tocopherol [14C] polyethylene glycol 1000 succinate in rats (1988b).. March 24, 1988, Technical Report # DM8807, Eastman Pharmaceuticals Drug Safety Evaluation. Beilman, J.J., Blakely, R.V. and Stong, D.B. Absorption, disposition and excretion of radioactivity following a single oral dose of tocopherol [14C] polyethylene glycol 1000 succinate in rats (1988c).. March 23, 1988, Technical Report # DM8806, Eastman Pharmaceuticals Drug Safety Evaluation. NCI National Cancer Institute (1994a) One year chronic study in rats. Conducted at International Research and Development Corporation, Mattawan MI 49071, November1, 1994 (IRDC report 560-040) for the National Cancer Institute, Bethesda, MD 20892. USA. NCI National Cancer Institute (1994b) One year chronic study in dogs. Conducted at International Research and Development Corporation, Mattawan MI 49071, November1, 1994 (IRDC report 560-041) for the National Cancer Institute, Bethesda, MD 20892. USA. Serota, D.G. and Slone, T.W. (2003a). 2-year oral carcinogenicity study of excipient containing 23 % TPGS in the mouse. Report of MPI Research Study Number 777003, submitted by Eastman Chemical Company Serota, D.G. and Slone, T.W. (2003b). 2-year oral carcinogenicity study of excipient containing 23 % TPGS in the rat. Report of MPI Research Study Number 777-004, submitted by Eastman Chemical Company SRICC (Safety Research Institute for Chemical Compounds Co.) (1998a). Bacterial Reverse Mutation test of TPGS. Study #SR- 9807, September 22, 1998. SRICC, Ltd Sapporo, Hokkaido, Japan. 19 TPGS in food for special medical purposes EFSA Journal (2007) 490, p. 20 of 20 SRICC (Safety Research Institute for Chemical Compounds Co.) (1998b). Chromosal Aberration test of TPGS . Study #SR- 9808, October 28, 1998. SRICC, Ltd Sapporo, Hokkaido, Japan. SRICC (Safety Research Institute for Chemical Compounds Co.) (1998c). Micronucleus Test of TPGS in rats. Study #SR- 9809, September 22, 1998. SRICC, Ltd Sapporo, Hokkaido, Japan. SRICC (Safety Research Institute for Chemical Compounds Co.) (1999a). Single Dose Oral Toxicity Study of TPGS in Beagle Dogs. Study #SR- 9810, March 5, 1999. SRICC, Ltd Sapporo, Hokkaido, Japan. SRICC (Safety Research Institute for Chemical Compounds Co.) (1999b). Study of TPGS for Effects on Embryo-Fetal Development in Rabbits. Study #SR- 9812, March 29, 1999. SRICC, Ltd Sapporo, Hokkaido, Japan. SRICC (Safety Research Institute for Chemical Compounds Co.) (1999c). Additional Study of TPGS for Effects on Embryo-Fetal Development in Rabbits. Study #SR9853, March 29, 1999. SRICC, Ltd Sapporo, Hokkaido, Japan. SRICC (Safety Research Institute for Chemical Compounds Co.) (1999d). Study of TPGS for Effects on Embryo-Fetal Development and Pre- and Post-natal Development, Including Maternal Function in rats. Study #SR- 9813, March 29, 1999. SRICC, Ltd Sapporo, Hokkaido, Japan. SCIENTIFIC PANEL MEMBERS Fernando Aguilar, Herman Autrup, Sue Barlow, Laurence Castle, Riccardo Crebelli, Wolfgang Dekant, Karl-Heinz Engel, Natalie Gontard, David Gott, Sandro Grilli, Rainer Gürtler, John Chr. Larsen, Catherine Leclercq, Jean-Charles Leblanc, F. Xavier Malcata, Wim Mennes, Maria Rosaria Milana, Iona Pratt, Ivonne Rietjens, Paul Tobback, Fidel Toldrá. 20