Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Blast-related ocular trauma wikipedia , lookup
Photoreceptor cell wikipedia , lookup
Eyeglass prescription wikipedia , lookup
Idiopathic intracranial hypertension wikipedia , lookup
Visual impairment due to intracranial pressure wikipedia , lookup
Dry eye syndrome wikipedia , lookup
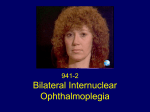
Neuroophthalmology Visual field defects: Scotomas: 1. Central scotoma etiology: optic neuritis, ischaemic lesion, compressive lesion macular diseases 2. Centrocoecal scotoma etiology: toxic optic neuropathies, Leber’s optic neuropathy congenital optic disc pit Visual field defects: 3. Altitudinal defects (retinal vascular damage, ischemic optic neuropathies) 4. Arcuate defects (selective damage to the nerve fibres) glaucoma optic neuritis drusen 5. Concentric narrowing of the isopters : retinitis pigmentosa, hysteria brain tumors Oculomotor (third) nerve disease Clinical features: Ptosis (paralysis of the levator) The eye is in an abducted position Failure of elevation Limitation of depression Trochlear (fourth) nerve disease Defective depression in adduction Hyperdeviation in the primary position Bielschowsky test (for accentuated the vertical deviation) Head tilting towards the normal side: no deviation Head tilting towards the side of paresis: increasing in hyperopia of the involved eye Abducens (sixth) nerve diseases Gives rise to defective abduction of the eye Aetiology of third, fourth and sixth nerve palsy Idiopathic (25 %, 50% recover spontaneously) Vascular (diabetes,hypertension,atherosclerosis) Trauma Aneurisms (basilar aneurisms, posterior communicating aneurisms with involvement of the pupil and severe pain) Abnormalities of the pupil Anatomical pathway of the pupillary light reflex (Parasympathetic nerve supply of the eye) First neurone: from the retina: -to pretectal nucleus in the midbrain Second neurone: -to both Edinger-Westphal nuclei Third neurone: -to the ciliary ganglion Fourth neurone: -to the sphincter pupillae Near reflex triad consists of: 1. lncreased accomodation 2. Convergence of the visual axes 3. Constriction of the pupils Abnormal pupillary reaction 1. Amaurotic pupils (no light perception due to an ON lesion) a. both pupils are of equal size b. neither pupil will react when the defective eye is stimulated c. both pupils react normally when the contralateral normal eye is stimulated d. the reaction of both pupils to a near stimulus is normal Abnormal pupillary reaction 2. Marcus Gunn pupil Swinging flashligt test: direct illumination of the involved eye: the reaction in both eyes will be sluggish when the light is brougt from the normal eye to the abnormal eye its pupil will be seen to dilate instead of constriction Abnormal pupillary reaction 3. Argyll Robertson pupils (hallmark of neurosyphilis) a- light-near dissociation: more extensive reaction to the near response than to a light stimulus, no reaction to light but a brisk response to near bcdef- both pupils are involved ( asymmetrical) vision is normal (in the affected eye) the pupils are frequently irregular in shape the pupils are small the pupils dilate poorly after installation of a mydriatic Abnormal pupillary reaction 4. Holmes-Addie tonic pupil: denervation of the postganglionic nerve supply to the sphincter pupillae and to the ciliary muscle abcdef- the affected pupil is larger than its fellow the reaction to light is extremly poor or non existent the reaction to a near stimulus is very slow and tonic redilation of the pupils is also prolonged and tonic accomodation is slow verniform movements of the iris border (sector paralysis) Diagnosis: 0.125 % pilocarpin: affected eye will constrict (denervation hypersensitivity) normal pupil will be unaffected Sympathetic nerve supply to the eye (can be considered as a three-neurone arc) First neuron: from the posterior hypothalamus to the ciliospinal centre of Budge (uncrossed, down the brainstem) Second neuron: to superior cervical ganglion (related to the subclavian artery and apical pleura) Third neuron: to dilator of the iris (along the internal carotid artery-it joins to the ophthalmic division of the trigeminal nerve - ciliary body nasociliary nerves) Horner's syndrome (oculosympathetic palsy) The features of Horner's syndrome are as follows: a-ptosis (paralysis of Müller's muscle) b-elevation of the lower lid (paralysis of the smooth muscle attached to the inferior tarsal plate) c-enophthalmus (narrowing of the palpebral fissure) d-miosis e-diminished sweating on the the ipsilateral part of the face (if the lesion is below the superior cervical ganglion) f-heterochromia of the iris (in congenital form) g-hypotony (transient) f- increase in amplitude of accomodation Diagnosis: 4% cocain; normal pupil will dilate; Horner‘s pupil will not dilate Nystagmus (involuntary to and fro oscillation of the eyes ) Classification: Pendular nystagmus: eye movements that are of equal velocity in each direction The movements can be horisontal, vertical, oblique or rotary Jerk nystagmus: a slow component in one direction and a fast component in the other direction (defined by the direction ofthe rapid fase: can be: right, left, up, down or rotary) Mixed nystagmus: the pendular movements are present in the primary position and the jerk movement are present when the eyes become deviated laterally The nystagmus can be further described as being either rapid or slow, coarse or fine, manifest or latent. Clinical types of nystagmus Phisiological end-point nystagmus optokinetic nystagmus vestibular nystagmus (caloric stimulation) Sensory deprivation nystagmus (ocular) This is due to an afferent defect in the neural contol system of ocular system: Common causes: Congenital cataract Macular hypoplasia Albinism Leber's congenital amaurosis The 2-4-6 rules: If a child loses central vision prior to the age of 2 years he will develop nystagmus Between the ages 2-6 years, some will and some will not develop Tipically pendular and horisontal Severity will depend on the extent of visual loss and it can often be dampened by convergence An anomalous head posturere may be adopted Motor inbalance nystagmus (due to a primary defect in the efferent mechanism ) Congenital nystagmus apparent at birth or shortly after (may be XLrecessiv or AD) jerk type, horisontal, may be dampened by convergence, not present during sleep abnormal head movements, strabismus Spasmus nutans develops between 4-12 month of life (prior to the age of 3 years) nystagmus, abnormal head position, head nodding asymmetrical, pendular fine, rapid, usually horisontal Latent nystagmus occurs under condition of uniocular fixation when one eye is occluded both eyes develop nystagmus with the fast phase directed towards the uncovered eye Ataxic nystagmus occurs in the abducting eye in association with internuclear ophthalmoplegia Downbeat nystagmus the fast phase is downwards, pathognomonic of a lesion involving the cervicomedullary junction at the foramen magnum Upbeat nystagmus the fast phase is in the upward direction, cause is drug intoxication (phenytoin) also occur in association with posterior fossa lesions Convergence-retraction nystagmus caused by co-contraction of the extraocular muscles, particularly the medial recti, jerk nystagmus, the fast phase brings the two eyes towards each other in a convergence movement, this is associated with retraction of the globe into the orbit found in lesions affecting the pretectal area, such as vascular accidents and pinealomas, can be one part of Parinaud's syndrome See-saw nystagmus (of Maddox) associated with bitemporal hemianopia is usually caused by chiasmal lesion when one eye rising and intorting the other eye fall and extorts Periodic alternating nystagmus jerk nystagmus that undergoes rhitmic changes in amplitude and direction Usually associated with vascular or demyelinating brainstem disease