Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
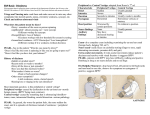
Dizziness David Johnson Staff Specialist, Emergency Medicine Dizziness • Need to decide is this – Vertigo • Central • Peripheral – Lightheadedness/presyncope • Sepsis • Drugs • Cardiac – Anxiety Vertigo • History – Sensation of motion • Room spinning • Patient spinning • “swimming” or “floating” – 1/3 of cases unable to determine Peripheral vs central Peripheral • Sudden onset • Nystagmus – horizontal or rotatory, fixed direction • Fast towards affected ear • Hearing loss • Nausea, diaphoresis • Positive head impulse • Negative skew Central • Slower onset – mostly • Less nystagmus. – May be vertical – Does not fatigue – Persists with fixation • Usually other neuro signs or headache • Often impaired balance • Negative head impulse • Positive skew BPPV • • • • • Most common cause of vertigo Very sudden onset, often after being supine Vertigo on head turning, not when head is still Duration of vertigo <1 min for each episode If this is not the story, do not make the diagnosis Other peripheral causes • Viral labyrinthitis – Constant +/- viral infection +/- hearing loss • Meniere’s – Tinnitus/aural fullness • Acoustic neuroma • Suppurative labyrinthitis Central causes • • • • Cerebellar stroke Brainstem stroke Drug toxicity Lateral Medullary Syndrome Physical exam • • • • Full neurological exam Cerebellar signs Ears, Weber/Rinne HINTS exam – Head impulse – Nystagmus – Test of skew HINTS Exam Investigations • MRI • CT has sensitivity approx 16% for posterior fossa disease • If you are worried get an MRI. If you are not worried do no imaging.