Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
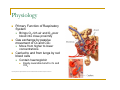
Respiratory System in a Breath June 21, 2012 Anna Spirkina, B.Sc.Pharm, ACPR Objectives By the end of this presentation the participants should be able to… Name the different anatomical structures that make up the respiratory system Describe the primary and secondary functions of the respiratory system Identify the main causes, symptoms, and mechanisms of disease for COPD and Asthma Anatomy Respiratory System Respiratory airways – tubes carrying air between the atmosphere and lungs Lungs Structures of the chest involved in producing air movement Anatomy http://www2.estrellamountain.edu/faculty/farabee/biobk/biobookrespsys.html Anatomy Nasal Passages Pharynx “Throat” Passage for respiratory and digestive systems Tonsils – lymphoid tissue (part of immune system) Trachea and esophagus Larynx Cartilage structure connecting pharynx and trachea Protects air passages Contains vocal folds Produce sound through vibration Prevent air entry when fully closed Anatomy Trachea and Bronchi Rigid, non-muscular tubes Cartilage-like rings Keep airways open Subdivide into smaller bronchioles Alveoli Thin-walled, inflatable air sacs Smallest working units http://www.nlm.nih.gov/medlineplus/ency/imagepages/8675.htm Anatomy Lungs Branched airways, alveoli, blood vessels, elastic connective tissue Volume – mostly air, weight – mostly blood No muscle to inflate/deflate during breathing Done through dimension changes of the chest cavity Diaphragm Separates chest cavity from abdominal cavity Main muscle involved in breathing Downward movement=inhalation, upward movement=exhalation Physiology Respiration Exchange of oxygen (O2) and carbon dioxide (CO2) between the external environment and the cells of the body Four steps Breathing – moving air in and out of lungs Exchange of O2 and CO2 between air in the alveoli and blood in the lung blood vessels Blood transport or O2 and CO2 between lungs and body Exchange of O2 and CO2 between body tissues and blood Respiratory System – first 2 steps Physiology Primary Function of Respiratory System Brings O2-rich air and O2-poor blood into close proximity Gas exchange by passive movement of O2 and CO2 Move from higher to lower concentrations Carried to and from lungs by red blood cells Contain haemoglobin Easily reversible bond to O2 and CO2 http://www.goldiesroom.org/Note%20Packets/13%20Human%20Other/00%20Human%20Other%20Systems--WHOLE.htm Physiology Non-respiratory Functions of Respiratory System Water loss and heat elimination Acid-base balance maintenance Speech, signing, vocalization Defence against inhaled foreign material Sense of smell Removal, modification or activation of materials added to blood by body tissues Common Disease States Chronic Obstructive Pulmonary Disease (COPD) Chronic bronchitis Emphysema Asthma COPD Chronic and recurrent obstruction of airflow Progressive disease Mostly preventable Most common cause – smoking Also chronic irritation by polluted air, allergens Some people – genetic component Lack of pronounced symptoms until advanced disease Increasing mortality (deaths) over past three decades Fourth leading cause of death – U.S. Combination of asthma, COPD and sleep apnea – 4th leading cause of death in Canada COPD Two types Emphysema Bronchitis destruction of walls between alveoli obstruction of small airways by mucus and changes in lining Both types usually overlapping Diagnostic tests Spirometry – measures the amount of air entering and leaving lungs http://www.nhlbi.nih.gov/health/health-topics/topics/copd/ COPD Symptoms Chronic cough Sputum production Difficulty breathing – shallow, more frequent breaths Barrel chest, pursed lips during expiration Symptoms of rapidly worsening COPD (x 48 hours) Increase in sputum production; change in colour of sputum Chest tightness Increasing difficulty breathing Decreased exercise tolerance Fever Requires timely medical attention COPD Treatment No cure, only symptom management Smoking cessation – the only strategy to slow progression of COPD Treatment approaches depend on disease severity COPD Severity Symptoms Treatment Mild Shortness of breath when hurrying on the level or walking up a slight hill Short-acting bronchodilators (eg. Ventolin® ± Atrovent® ) Moderate Shortness of breath causing the patient to stop walking after ~100m on the level Short-acting bronchodilators (eg. Ventolin®) + Long-acting bronchodilators (eg. Serevent® or Spiriva®) Severe and Very Severe Patient too breathless to leave the house, breathless after dressing; heart failure due to COPD Short-acting bronchodilators (eg. Ventolin®) + Combination steroid/bronchodilator (eg. Advair® or Symbicort®) ± Theophylline ± Oxygen Asthma Reversible episodic airway inflammation and obstruction Triggered by variety of stimuli Genetic component Childhood asthma The number of people diagnosed with asthma have been increasing over several decades Over 2 million Canadians reported history of asthma in 2010 No proportional increase in mortality (deaths) or hospitalizations over the past years Allergens Cold air, exercise, drugs, air pollution, respiratory infections Asthma Pathogenesis (how it happens) Thickening of airway walls due to inflammation Excessive secretion of thick mucus Constriction of the smaller airways Diagnostic tests Spirometry - measures the amount of air entering and leaving lungs http://www.asthmacuretoday.com/wp-includes/images/522asthma.jpg Asthma Symptoms Episodes of dry hacking coughing, chest tightness, wheezing, whistling sound when breathing Often associated with exercise or known allergens, but may be spontaneous Severe asthma attack Progresses over days or hours Severe presentation of the usual symptoms Can only speak few words at a time Non-responsive to rescue inhaler Pale or ash-coloured skin Increased heart rate Requires immediate medical attention Asthma Characteristic Frequency or Value Daytime symptoms <4 days/week Night-time symptoms <1 night/week Physical activity Normal Asthma attacks Mild, infrequent Absence from school or work None Need for rescue inhaler <4 doses/week Treatment Varies depending on how well symptoms are controlled Asthma education Action plans Asthma Dispensing Medications for Asthma and COPD Class of Medication Examples Mechanism of Action Things to Remember Short-acting Bronchodilators Ventolin® Bricanyl® Relax muscle lining of bronchi quickly but short term Ventolin® - Shake inhaler before use Long-acting Bronchodilators Serevent® Oxeze® Relax muscle lining of bronchi long term Inhaled steroids Flovent® Pulmicort® Decrease inflammatory response Rinse mouth after use to prevent thrush Combination products Symbicort® Advair® Relax bronchi, decrease inflammation Rinse mouth after use to prevent thrush Anticholinergics Atrovent® Spiriva® Inhibit chemical receptors responsible for bronchocostriction and mucus production Spiriva® - capsules not for oral ingestion; expire 5 days after foil opened Atrovent® - Shake inhaler before use Summary Respiratory system consists of respiratory airways, lungs, and structures of the chest cavity that are involved in air movement The primary function of the respiratory system is to facilitate gas exchange between oxygen-rich atmosphere and oxygen-poor blood Asthma and COPD are two of the common disease states of the respiratory system References “Asthma, by age group and sex”. Summary Tables. 11 June 2011. Statistics Canada. 18 December 2011. http://www40.statcan.gc.ca/l01/cst01/health49a-eng.htm “Centre for Chronic Disease Prevention and Control”. Chronic Disease. 25 October 2011. Public Health Agency of Canada. 18 December 201. http://www.phac-aspc.gc.ca/ccdpccpcmc/index-eng.php Kelly, William., Sorkness, Christine. “Asthma” Pharmacotherapy: A Pathophysiologic Approach. 7th Ed. Ed.Joseph Dipiro et al. China: The McGraw-Hill Companies, Inc., 2008. 463-95. Print. Moore, Keith L., Agur, Anne M.R. “Thorax” Essential Clinical Anatomy. 3rd Ed. Baltimore, MD:Lippincott Williams and Wilkins, 2007. 70-80. Print. Moore, Keith L., Agur, Anne M.R. “Neck” Essential Clinical Anatomy. 3rd Ed. Baltimore, MD:Lippincott Williams and Wilkins, 2007. 611-20. Print. Porth, Carol. “Disorders of Ventilation and Gas Exchange” Essentials of Pathophysiology: Concepts of Altered Health States. 2nd Ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2007. 491-505. Print. Sherwood, Lauralee. “The Respiratory System” Human Physiology: From Cells to Systems. 6th Ed. Ed. Peter Adams. Belmont,CA: Thomson Brooks/Cole, 2007. 451-99. Print. Williams, Dennis., Bourdet, Sharya. “Chronic Obstructive Pulmonary Disease” Pharmacotherapy: A Pathophysiologic Approach. 7th Ed. Ed.Joseph Dipiro et al. China: The McGraw-Hill Companies, Inc., 2008. 495-518. Print.