Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Coronary artery disease wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Myocardial infarction wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
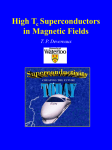
European Heart Journal – Cardiovascular Imaging (2013) 14, 366–373 doi:10.1093/ehjci/jes196 Age, gender, blood pressure, and ventricular geometry influence normal 3D blood flow characteristics in the left heart Daniela Föll 1, Steffen Taeger 1, Christoph Bode 1, Bernd Jung 2, and Michael Markl 3,4* 1 Department of Cardiology and Angiology, University Heart Center Freiburg, Hugstetterstr.55, Freiburg 79106, Germany; 2Department of Diagnostic Radiology, Medical Physics, Albert-Ludwigs-University Hospital Freiburg, Freiburg, Germany; 3Department of Radiology, Feinberg School of Medicine, Northwestern University, 737 N. Michigan Avenue Suite 1600, Chicago, IL 60611, USA; and 4Department of Biomedical Engineering, McCormick School of Engineering, Northwestern University, 737 N. Michigan Avenue Suite 1600, Chicago, IL 60611, USA Received 27 June 2012; accepted after revision 24 August 2012; online publish-ahead-of-print 21 September 2012 Aims The aim of this study was to assess the effect of age, gender, physiological, and global cardiac function parameters on differences in normal 3D blood flow in the left ventricle (LV) and atrium (LA) using 4D flow magnetic resonance imaging (MRI). ..................................................................................................................................................................................... Methods Four-dimensional flow MRI was acquired in healthy volunteers of two age and gender groups: ,30 years (6 women, and results n ¼ 12) and .50 years (6 women, n ¼ 12). Systolic and early to mid-diastolic vortex flow (number of vortices, duration, area, peak velocity inside the vortex) in the LA and LV was assessed using intra-cardiac flow visualization based on 3D particle traces and velocity vector fields. A larger number of vortices in the LA were found in young compared with older individuals (number of diastolic vortices: 1.6 + 0.8 vs. 0.7 + 0.7, P ¼ 0.01) with higher velocities (54 + 12 cm/s vs. 41 + 11 cm/s in systole, 47 + 13 vs. 31 + 8 cm/s in diastole, P , 0.05). Vortices in the LV base were smaller in women compared with men (369 + 133 vs. 543 + 176 mm2, P ¼ 0.009), while vortex size was increased in mid-ventricular locations (maximum area: 546 + 321 vs. 293 + 174 mm2, P , 0.05). Correlation analysis revealed significant relationships (P ¼ 0.005 –0.048, correlation coefficients ¼ 0.44–0.84) between LA and LV vortex characteristics (number, size, vortex velocities) and blood pressure as well as end-diastolic volume, LV length, and ejection fraction. ..................................................................................................................................................................................... Conclusions Flow patterns in the left heart demonstrated differences related to age, gender, blood pressure, and ventricular geometry. The findings constitute a prerequisite for the understanding of the impact of cardiac disease on intra-cardiac haemodynamics. ----------------------------------------------------------------------------------------------------------------------------------------------------------Keywords Blood flow † 4D flow MRI † Ageing † Gender † Vortex Introduction Blood flow through the beating heart is complex and normal physiological as well as pathologically altered blood flow conditions are difficult to assess in vivo. Alterations of blood flow can carry important consequences in congenital or valvular heart disease, in remodelling of the left ventricle (LV) in ischaemic heart disease or in aortic diseases.1,2 To date, a comprehensive analysis of intra-cardiac 3D flow patterns is not performed in clinical routine and only limited data on normal atrial and ventricular flow patterns are available. Blood flow measurements are limited to 2D Doppler echocardiography or phase contrast magnetic resonance imaging (MRI) which acquires flow velocities within a user-selected 2D plane.3,4 Both techniques are limited to measurements at predefined locations and often assess only a single velocity component of the underlying threedirectional blood flow. Routinely used phase contrast MRI or Doppler ultrasound do not offer the possibility to measure and visualize the temporal evolution of complex flow patterns within a 3D volume encompassing the beating human heart. * Corresponding author. Tel: +1 312 695 1799, Email: [email protected] Published on behalf of the European Society of Cardiology. All rights reserved. & The Author 2012. For permissions please email: [email protected] 367 3D blood flow characteristics in the left heart To overcome these limitations, 4D flow MRI (ECGsynchronized 3D phase contrast MRI with three-directional velocity encoding) has been applied in a number of studies for the analysis of 3D blood flow with full volumetric coverage of the left atrium (LA)5 and left ventricle (LV).6 – 8 Vortical flow within the cardiac chambers has been described in healthy volunteers1,5,7 – 10 as well as in patients with cardiomyopathy,6,11 mitral valve insufficiency,12 and after heart transplantation.13 Fourdimensional MRI data have been used for the quantification of flow within cardiac chambers,14 through the heart valves,15 and in pulmonary arteries in patients with Fontan circulation.1 Although it is known that age and gender alter LV myocardial tissue properties16 and function,17,18 a systematic evaluation of normal physiological LA and LV flow formation in relation to age, gender, and other influencing factors such as blood pressure or heart rate is missing. The aim of this study was to test the hypothesis that age, gender, physiological, and global cardiac function parameters correlate with the presence and extent of left atrial and left ventricular systolic and diastolic vortex flow patterns in healthy volunteers. Methods Study population We included 24 healthy volunteers in two age and gender groups: ,30 years (n ¼ 12, mean 23.3 + 1.6 years, 6 women) and .50 years (n ¼ 12, 58.3 + 4.2 years, 6 women). The cut-off age was chosen based on the assumption that a large difference between the age-group cut-offs (20 years) would provide a clear separation of both groups and result in an improved separation of flow characteristics given the small number of individuals in each cohort. All volunteers were without history, symptoms, or medication of cardiovascular or pulmonary disease, diabetes, arterial hypertension, or peripheral arterial disease. All volunteers had a normal echocardiography and ECG findings. Written informed consent was obtained from all participants and the study was approved by our local ethics board. The volunteers’ characteristics are summarized in Table 1. MR imaging All examinations were performed using a standard 12-element torso coil (3T, Magnetom TRIO, Siemens, Erlangen, Germany). We employed flow-sensitive MRI with volumetric 3D coverage of the whole heart and three-directional velocity encoding (4D flow MRI) to systematically identify and evaluate the existence and extent of characteristic flow patterns in the left heart.19 The imaging sequence consisted of a previously described, k-space segmented, rf-spoiled gradient echo sequence with interleaved three-directional velocity encoding.1,20 Other imaging parameters were: TE ¼ 2.4 ms, TR ¼ 4.8 ms, flip angle ¼ 78, field of view ¼ 320 × 240 mm, spatial resolution ¼ 2.5 × 2.5 × 2.8 mm3, temporal resolution ¼ 38.4 ms, scan time 15 – 25 min, and parallel imaging with reduction factor R ¼ 2.21 Magnetic resonance imaging acquisitions were synchronized to the heart and breathing cycle using prospective ECG gating and adaptive diaphragm navigator gating.20 Prospective ECG gating resulted in 4D flow data covering about 80 – 90% of the heart cycle, i.e. including systole, early, and mid-diastole. Data analysis All 4D flow data underwent pre-processing including noise masking, eddy current correction, Maxwell corrections, and calculation of a 3D phase contrast MR angiogram as described previously.22 – 24 To visually identify and grade intra-cardiac flow patterns, 3D visualization was employed (EnSight v. 8.2, CEI, Apex, NC, USA). Flow analysis included the calculation of time-resolved 3D particle traces originating from emitter planes which were manually placed in the pulmonary veins. The resulting traces provide a visual representation of the temporal dynamics and spatial distribution of 3D blood flow (Figure 1). In addition, vector fields in the two- and fourchamber planes were calculated for each time point (Figures 2 and 3). In order to identify and grade intra-atrial and intra-ventricular vortex flow, particle traces were first used to identify vortices and their directions of rotation. In the following, vector graphs were analysed as follows: † Left atrium (two-chamber and four-chamber view): number, duration, maximum area, and peak velocities inside the vortex. The analysis was performed separately for both systole and early to mid-diastole. † Left ventricle (two-chamber and four-chamber view): peak diastolic LV in-flow velocity and systolic and early to mid-diastolic vortex formation (number, duration, maximum area, and peak velocity inside the vortex) at base, mid, and apex of the LV. Vortex duration was defined as the time between the onset of visible vortical flow to its disappearance. Vortical flow in the LA was assessed as viewed from behind, LV flow was evaluated as viewed from above (four-chamber view) or from the left side (two-chamber view). If not stated otherwise, the results given in the text refer to the analysis in two-chamber view. Statistical analysis All data are presented as mean + standard deviation unless stated otherwise. Comparisons between age groups and genders were performed by unpaired Student’s t-test for normally distributed values and the Mann– Whitney U-test for values not normally distributed. Systolic and diastolic vortex formation in the LA and LV (number, duration, maximum area, and peak velocity inside the vortex) were correlated with physiological parameters, such as age, heart rate, and blood pressure and with LV geometry and function. Correlations were calculated by the Pearson Product Moment for values normally distributed, and Spearman’s test was used to calculate correlations for values not normally distributed. The Kolmogorov – Smirnov test was used to test for normality. A. Kruskal – Wallis one-way analysis of variance (‘on Ranks’ for not normally and equally distributed values) followed by the Holm– Sidack (or Dunn’s) procedure for pairwise multiple testing was used for the comparisons between the flow characteristics within the three levels of the LV. Statistical testing was performed using SigmaStat for Windows Version 3.10. Two-tailed tests with P , 0.05 were considered statistically significant. Results Study cohort The clinical characteristics for all subjects are summarized in Tables 1 and 2. Older volunteers had higher systolic blood pressure (P ¼ 0.01) and shorter LV length (P ¼ 0.02). Older men had higher heart rates (P ¼ 0.01), systolic blood pressures (P ¼ 0.04), and higher LV mass (P ¼ 0.02) compared with young men. Women had a higher LVEF and reduced left ventricular end-diastolic volume (LVEDV), LVESV, and LV mass compared with men (P , 0.05, Table 2). 368 Table 1 D. Föll et al. Study cohort Age group 1 .................................................................... All (n 5 12) Men (n 5 6) Women (n 5 6) Age group 2 .................................................................... All (n 5 12) Men (n 5 6) Women (n 5 6) ............................................................................................................................................................................... Age (years) 23 + 2 24 + 1 23 + 2 58 + 4* 59 + 4* 58 + 4* Heart rate (b.p.m.) 66 + 9 61 + 5 70 + 10 67 + 6 70 + 5* 64 + 7 113 + 5 74 + 4 113 + 7 75 + 4 123 + 10* 77 + 8 128 + 9* 80 + 10 120 + 9 75 + 4 BP sys. (mmHg) BP dia. (mmHg) LVEF (%) LVEDV (mL) LVESV (mL) LV length (mm) LV mass (gm) LVSV (mL) 113 + 3 72 + 4 65 + 3 64 + 2 65 + 3 65 + 4 62 + 2 68 + 3** 139 + 21 146 + 18 132 + 21 127 + 17 138 + 14 116 + 12** 49 + 9 95 + 6 52 + 8 99 + 5 45 + 8 91 + 3** 45 + 10 86 + 7* 52 + 8 90 + 7 37 + 6** 83 + 5 118 + 27 138 + 21 97 + 12** 134 + 37 174 + 7* 103 + 15** 91 + 13 94 + 12 82 + 8 86 + 6 87 + 13 78 + 8 BP, blood pressure; LVEF, ejection fraction; LVEDV, left ventricular end-diastolic volume; LVESV, left ventricular end-systolic volume; LVSV, left ventricular stroke volume. All values are means + 1 standard deviation. *P , 0.05 vs. age group 1. **P , 0.05 vs. men. Figure 1 3D visualization of diastolic left atrial and ventricular inflow characteristics with substantial vortex formation in the LA and laminar ventricular filling with clearly separated left and right pulmonary vein flow channels. LV, left ventricle; LPV, left pulmonary veins; rPV, right pulmonary veins. Three-dimensional particle traces In all volunteers, vortical flow was found in the LA und LV. Systolic and diastolic vortical flow in the LA was evident in 92% of the young and 83% of the older volunteers (Figure 1). Most LA vortices (81% in young and 74% in older subjects) were directed clockwise as viewed from the back. Twenty-eight percent of the vortices in men and only 16% in women were anti-clockwise. (151 + 60 vs. 124 + 74 ms; P ¼ 0.055 in two-chamber view; 171 + 90 vs. 96 + 56 ms in four-chamber view, P ¼ 0.005). Younger individuals showed an increased duration (P ¼ 0.023) and higher velocities (P ¼ 0.012) inside the vortices in the LA for both systole and diastole compared with the older group. Diastolic LA vortices occurred less frequently in older volunteers (five subjects showed no vortex compared with one subject ,30 years) (P , 0.013). Left atrial flow In 75% of subjects, systolic and diastolic vortex flow in the LA was evident as shown in Figure 1 and summarized in Tables 3 for vector plot analysis. Compared with early to mid-diastolic vortex flow, systolic vortex flow occurred more frequently (systole vs. diastole: 2.2 + 1.0 vs. 1.1 + 0.9, P , 0.001), and had longer duration Left ventricular flow The results of LV flow analysis are summarized in Tables 4. The maximum area of vortices decreased from base to apex for both men and women. Larger vortices were found at the base (472 + 196 vs. 299 + 112 mm2 in mid-ventricular and 214 + 3D blood flow characteristics in the left heart 369 Figure 2 Vector graph visualization of intra-cardiac blood flow in a young (A) and an old (B) healthy volunteer. The formation of diastolic vortex flow in the LA and LV is evident and indicated by the dashed circles. Note the reduced diastolic in-flow velocities (colour coding) and less-prominent vortex flow in the older volunteer. RV, right ventricle; Ao, aorta. 128 mm2 in apical parts of the LV, P ¼ 0.002). Peak velocities within the vortices decreased from base to apex (base 6.1 + 1.7 cm/s, mid 4.5 + 1.0 cm/s, apex 3.3 + 0.8 cm/s, P , 0.001). The smallest numbers of vortices were found in apical parts of the LV (0.3 + 0.4 vs. 2.0 + 0.4 in basal or 2.0 + 0.7 in midventricular segments, P , 0.001). The majority subjects presented with two vortices in the LV base (88%) and mid-ventricular LV (54%) irrespective of age. Peak vortex velocities were significantly higher in the younger compared with older volunteers in the LV base (6.9 + 1.4 vs. 5.2 + 1.6 cm/s; P ¼ 0.005) as exemplary illustrated in Figure 2. In the mid-ventricular LV, older participants demonstrated less vortices compared with the younger individuals (in four-chamber view: 1.7 + 0.7 vs. 1.1 + 0.7, P ¼ 0.002). Gender-related differences At the LV base, women revealed smaller vortices (369 + 133 vs. 543 + 176 mm2, P ¼ 0.009) (Figure 3), while vortex size was increased at the mid-ventricular location compared with men (maximum area: 546 + 321 vs. 293 + 174 mm2, P ¼ 0.033). In addition, apical vortices had increased duration in women compared with men (98 + 38 vs. 48 + 19 ms; P ¼ 0.038). Correlation with physiological data, LV function, and morphology There was an inverse relationship between increasing age and systolic vortex velocities [correlation coefficient (CC) ¼ 20.51, P ¼ 0.01] and number of diastolic vortices (CC ¼ 20.45, P ¼ 0.03) in the LA. Furthermore, age was inversely correlated with the maximum area (CC ¼ 20.49, P ¼ 0.02) and velocity (CC ¼ 20.48, P ¼ 0.02) of basal LV vortices. Heart rate did affect the number of diastolic LA vortices (CC ¼ 20.55, P ¼ 0.007) and was also correlated with the duration (basal: CC ¼ 20.46, P ¼ 0.03; mid-LV: CC ¼ 20.57, P ¼ 0.005) and area (mid-LV: CC ¼ 20.45, P ¼ 0.03) of LV vortices. Increased systolic blood pressure resulted in a larger size of diastolic LA vortices (CC ¼ 0.50, P ¼ 0.046) but reduced vortex peak velocity (CC ¼ 20.54, P ¼ 0.03) and less basal LV vortices (CC ¼ 20.44, P ¼ 0.048) with lower peak velocities (CC ¼ 0.57, P ¼ 0.007). Diastolic blood pressure correlated with mid-ventricular and apical LV vortex velocities (CC ¼ 20.74, P , 0.001, respectively, CC ¼ 20.84, P ¼ 0.03). Left ventricular end-diastolic volume influenced the number of LA vortices in diastole (CC ¼ 0.49, P ¼ 0.03) and LV length correlated with the number of LV vortices (mid-LV: CC ¼ 0.52, P ¼ 370 D. Föll et al. Figure 3 Vector graph visualization of intra-cardiac blood flow in a female participant (A) and a male participant (B) of the young age group. Note the reduced diastolic vortex flow in the base of the LV in women compared with men. Vortices in the LV base and mid-ventricle are indicated by the dashed circles. LA, left atrium; RV, right ventricle; Ao, aorta. Table 2 Genders’ characteristics Men (n 5 12) Women (n 5 12) 0.04, apical: CC ¼ 20.69, P ¼ 0.003). A higher LVEF was associated with a decreased area of basal vortices (CC ¼ 20.49, P ¼ 0.03) and more apical vortices (CC ¼ 0.421, P ¼ 0.05). ................................................................................ Age (years) Heart rate (b.p.m.) 41 + 18 66 + 7 39 + 18 66 + 9 BP sys. (mmHg) 120 + 11 117 + 8 BP dia. (mmHg) LVEF (%) 77 + 8 63 + 3* 74 + 4 66 + 3 142 + 17* 127 + 19 52 + 8* 95 + 8* 42 + 8 87 + 6 154 + 24** 100 + 14 90 + 10 85 + 12 LVEDV (mL) LVESV (mL) LV length (mm) LV mass (gm) LVSV (mL) BP, blood pressure; LVEF, left ventricular ejection fraction; LVEDV, left ventricular end-diastolic volume; LVESV, left ventricular end-systolic volume; LVSV, left ventricular stroke volume. All values are means + 1 standard deviation. *P , 0.05 vs. women. *P , 0.001 vs. women. Discussion The maintenance of a stable blood flow is fundamental for human life and the ultimate measure of adequate cardio-vascular function. The results of this study demonstrate the potential of 4D flow MRI with whole heart coverage for the detailed analysis of intra-cardiac vortex flow. The results of our semi-quantitative analysis of flow patterns demonstrated significant age as well as gender-related differences in intra-atrial and intra-ventricular flow patterns. Flow characteristics in the LA have previously been analysed by others and anti-clockwise vortex formation in the LA has been reported before (as viewed from the front).7 In our study, previously not described vortex formation in the opposite direction was found in 54% of the individuals mainly from blood flow originating in the upper pulmonary veins. Similar to findings in other 371 3D blood flow characteristics in the left heart Table 3 Cumulative results of vortex analysis in the LA for the young (<30 years) and the older age group (>50 years) analysed in the two-chamber view and in the four-chamber-view Number Duration (ms) Area max. (mm2) Vmax (cm/s) ............................................................................................................................................................................... Analysis based on two-chamber view Systole ,30 years (n ¼ 12) .50 years (n ¼ 12) Diastole ,30 years (n ¼ 12) .50 years (n ¼ 12) Analysis based on four-chamber view 2.2 + 1.0 178 + 63* 338 + 142 54 + 12* 2.3 + 1.1# 124 + 44 354 + 268 41 + 11 1.6 + 0.8* 134 + 88 319 + 283 47 + 13* 0.7 + 0.7 110 + 47 332 + 164 31 + 8 1.9 + 0.9 2.0 + 1.2 174 + 68# 169 + 112# 350 + 279 259 + 167 41 + 11 36 + 12 1.7 + 1.0 1.0 + 1.2 111 + 5 70 + 50 219 + 194 157 + 100 37 + 8 27 + 11 Systole ,30 years (n ¼ 12) .50 years (n ¼ 12) Diastole ,30 years (n ¼ 12) .50 years (n ¼ 12) Data represent mean values + standard deviation. Vmax, peak velocity; Area max., maximum area. *P , 0.05 vs. older age group. # P , 0.05 vs. diastole (same age group). Table 4 Cumulative results of vortex analysis in the LV for the young (<30 years) and the older age group (>50 years) analysed in the two-chamber view and in the four-chamber view Number Duration (ms) Area max. (mm2) Vmax (cm/s) 2.1 + 0.3 2.0 + 0.4 154 + 68 116 + 52 538 + 164 406 + 206 69 + 14 52 + 16* 2.3 + 0.7 1.8 + 0.6 170 + 81 123 + 55 286 + 110 312 + 118 48 + 6 43 + 14 0.3 + 0.4 0.3 + 0.5 153 + 66 89 + 89 149 + 108 260 + 152 30 + 10 37 + 6 Base ,30 years (n ¼ 12) 1.8 + 0.4 126 + 37 473 + 200 65 + 9 .50 years (n ¼ 12) 1.9 + 0.3 131 + 55 438 + 155 52 + 10* ............................................................................................................................................................................... Analysis based on two-chamber view Base ,30 years (n ¼ 12) .50 years (n ¼ 12) Mid ,30 years (n ¼ 12) .50 years (n ¼ 12) Apex ,30 years (n ¼ 12) .50 years (n ¼ 12) Analysis based on four-chamber view Mid ,30 years (n ¼ 12) .50 years (n ¼ 12) 1.7 + 0.7 155 + 103 452 + 333 54 + 19 1.1 + 0.7* 130 + 89 381 + 219 43 + 14 Apex ,30 years (n ¼ 12) 0.5 + 0.7 72 + 33 152 + 51 26 + 6 .50 years (n ¼ 12) 0.5 + 0.7 84 + 50 124 + 55 28 + 8 Data represent mean values + standard deviation. Vmax, peak velocity; Area max., maximum area. *Significant differences between both age groups (P , 0.05). 372 studies and probably due to the more cranial location of the left pulmonary veins, vortex formation in flow path ways originating from the left side was more prominent.5 In contrast to a previous study,5 we did not find a relationship between LA vortex flow duration and heart rate. In addition, we found shorter durations of LA vortices which might be related to the higher temporal resolution in our study. As reported by Kilner et al.,7 the heart’s vortical flow characteristics in conjunction with the looped formation of the heart itself seem to be fundamental for a stable blood flow, prevention of energy losses, and optimal atrial –ventricular coupling especially with increased heart rate under exercise. Furthermore, vortex flow is meant to play an important role in the valves’ closure25 and in preventing blood flow stasis and thromboembolic risk. The asymmetric vortical inflow in the cardiac chambers has been reported in healthy volunteers using phase contrast MRI5,7 and ultrasound vectorparticle image velocimetry.26,27 Vortices have been described in basal LV locations at the anterior mitral leaflet and near the posterior mitral leaflet.7,28 It is assumed that vortices play an important role in redirecting the inflowing blood flow towards the aortic valve. Previous 4D flow MRI studies have demonstrated that in the healthy heart 30% of the blood in the LVEDV passes the LV directly within one cardiac cycle in the shortest way and with least energy losses,14 whereas this percentage of ‘direct flow’ in the LV is strongly reduced in the failing heart.6,11 Studies with vector particle image velocimetry also revealed altered LV vortices in patients with systolic LV dysfunction,27 stressing the importance of an undisturbed vortical flow for optimal cardiac function. However, none of these studies based their findings on a systematic age- and gender-related comparison of LA and LV flow characteristics including other influencing factors such as blood pressure or heart rate. As we could demonstrate, ageing resulted in a reduced number of diastolic LA vortices as well as lower velocities and durations of systolic LA vortices. These findings could not be explained by heart rate or LVEF, which did not differ between the age groups. Shorter LV lengths and higher systolic blood pressures might have contributed to the reduced numbers of mid-ventricular vortices and the reduced diastolic vortical velocities in the LA and LV base but do not explain the other differences of LA vortical flow. It is known that ageing alters LA29 and LV function17 due to changes of myocardial structure and differences in Ca channel handling, alterations in the sympathic nervous system, and a reduction in arterial compliance and endothelial function.16 In this context, altered Doppler inflow characteristics in the LA30 and LV31 have been described with ageing. In line with our finding of reduced LA diastolic vortices, the inflow in the LA decreases in diastole with increased age, whereas inflow in systole increases.30 Our finding of reduced diastolic vortex formation in the LA and LV in older volunteers might therefore reflect age-related diastolic dysfunction of these individuals. Women revealed smaller vortices in the LV base and a higher number of vortices in the mid-ventricular LV. In addition, apical vortex formation lasted longer compared with men. Geometric differences such as reduced LVEDV or LV length in women did not explain these gender differences. The higher LVEF in older D. Föll et al. women might have contributed to smaller vortices in basal parts in women. Similar to our findings, gender differences in LV inflow measured by Doppler echo have been described.31 However, the increased extent of mid-ventricular vortices in women is a previously unreported finding and might be caused by increased vascular and ventricular stiffness in women as previously reported by Redfield et al.32 Limitations A limitation of our study is related to the prospective ECG gating of our 4D flow MR sequence. As a result, only data representing about 80 –90% of the heart cycle were acquired within the RR interval. Therefore, atrial contraction with consecutive second filling of the LV could only be visualized in four of the older individuals despite sinus rhythm in all volunteers. It should be noted that, as a result of prospective ECG gating, late diastole is variably included in the results. As a result, the findings of this study need to be interpreted with care and represent flow characteristics during early and mid-diastole only. A further drawback of the data analysis methodology is related to the use of velocity vector fields from conventional two- and three-chamber views which minimize the ‘three-dimensional’ aspect of our findings, even though these were based on threedirectional data. Another limitation of the study is that we did only perform a semi-quantitative analysis without evaluation of intra- and interobserver variability. In addition, no data on inter-study variability are currently available to provide information on the test-retest reliability of cardiac 4D flow MRI and the analysis methods presented here. The small size of the study cohort constitutes a major limitation and underlines the feasibility character of this study. In our current study, we have analysed the impact of the haemodynamic state of an individual (heart-rate, blood pressure, etc.) on the resulting cardiac flow characteristics using correlation analysis. The small number of volunteers might explain the significant but moderate correlations (r ¼ 0.4 –0.8) found in our cohort between flow characteristics and cardiac function parameters, blood pressure, heart rate, and age. The evaluation of intra-cardiac 3D blood flow in larger cohorts is warranted to confirm our results and clarify the degree of correlation between the haemodynamic state of an individual and the observed flow characteristics. In addition, further studies with increased sample sizes and including patient data are essential to evaluate the influence of cardiac disease on the flow characteristics of the left heart. Further, an investigating of the reproducibility of the flow characteristics indices and semi-quantitative flow pattern grading used in this study are needed. Although we did not evaluate the observer variability of the semi-quantitative flow pattern grading, previous work by our group has demonstrated the reliability of flow pattern grading based on 4D flow MRI data. In a recent study assessing aortic flow patterns in patients with Marfan syndrome using 4D flow MRI, we found substantial inter-observer agreement (kappa ¼ 0.7) for the visual grading of helix and vortex flow in the ascending aorta, the aortic arch, and descending aorta.33 A further drawback is related to the relatively long 4D flow MRI acquisition times and the effective averaging of velocity 373 3D blood flow characteristics in the left heart measurements over many heart cycles, only flow characteristics that occur consistently through successive beats are recorded and analysed. The peak local velocities and numbers of vortices identified may underestimate those occurring in real time in any given beat. Nevertheless, our study describes the feasibility of blood flow imaging in the healthy heart and offers new insights into intra-cardiac blood flow characteristics. Conclusions Cardiac 4D flow MRI in a small cohort of healthy subjects demonstrated that heart rate, blood pressure, LV geometry, age, and gender can affect intracardiac blood flow characteristics. These findings might have the potential to improve our understanding of physiological and pathological processes of cardiovascular function. Future studies including data on reproducibility and larger patient cohorts are needed to assess the impact of intra-cardiac flow patterns on cardiovascular disease and their diagnostic value related to disease progression and therapy monitoring. 14. 15. 16. 17. 18. 19. 20. Funding 21. M.M. is supported by the NMH Excellence in Academic Medicine (EAM) Program ‘Advanced Cardiovascular MRI Research Center’. D.F. is supported by the Deutsche Forschungsgemeinschaft (DFG). Grant # FO 507/2-1, FO 507/3-1. 22. Conflict of interest: none declared. 23. References 24. 1. Markl M, Geiger J, Kilner PJ, Föll D, Stiller B, Beyersdorf F et al. Time-resolved three-dimensional magnetic resonance velocity mapping of cardiovascular flow paths in volunteers and patients with Fontan circulation. Eur J Cardiothorac Surg 2011;39:206 –12. 2. Clough RE, Waltham M, Giese D, Taylor PR, Schaeffter T. A new imaging method for assessment of aortic dissection using four-dimensional phase contrast magnetic resonance imaging. J Vasc Surg 2012 [Epub ahead of print]. 3. Pelc NJ, Sommer FG, Li KC, Brosnan TJ, Herfkens RJ, Enzmann DR. Quantitative magnetic resonance flow imaging. Magn Reson Q 1994;10:125 – 47. 4. Chai P, Mohiaddin R. How we perform cardiovascular magnetic resonance flow assessment using phase-contrast velocity mapping. J Cardiovasc Magn Reson 2005;7:705 –16. 5. Fyrenius A, Wigstrom L, Ebbers T, Karlsson M, Engvall J, Bolger AF. Three dimensional flow in the human left atrium. Heart 2001;86:448 – 55. 6. Bolger AF, Heiberg E, Karlsson M, Wigstrom L, Engvall J, Sigfridsson A et al. Transit of blood flow through the human left ventricle mapped by cardiovascular magnetic resonance. J Cardiovasc Magn Reson 2007;9:741–7. 7. Kilner PJ, Yang GZ, Wilkes AJ, Mohiaddin RH, Firmin DN, Yacoub MH. Asymmetric redirection of flow through the heart. Nature 2000;404:759–61. 8. Kim D, Gilson WD, Kramer CM, Epstein FH. Myocardial tissue tracking with twodimensional cine displacement-encoded MR imaging: development and initial evaluation. Radiology 2004;230:862 –71. 9. Wigstrom L, Ebbers T, Fyrenius A, Karlsson M, Engvall J, Wranne B et al. Particle trace visualization of intracardiac flow using time-resolved 3D phase contrast MRI. Magn Reson Med 1999;41:793 –9. 10. Fredriksson AG, Zajac J, Eriksson J, Dyverfeldt P, Bolger AF, Ebbers T et al. 4-D blood flow in the human right ventricle. Am J Physiol Heart Circ Physiol 2011;301: H2344 –50. 11. Carlhall CJ, Bolger A. Passing strange: flow in the failing ventricle. Circ Heart Fail 2010;3:326 –31. 12. Dyverfeldt P, Kvitting JE, Carlhall CJ, Boano G, Sigfridsson A, Hermansson U et al. Hemodynamic aspects of mitral regurgitation assessed by generalized phasecontrast MRI. J Magn Reson Imaging 2011;33:582 –8. 13. Markl M, Geiger J, Arnold R, Stroh A, Damjanovic D, Föll D et al. Comprehensive 4-dimensional magnetic resonance flow analysis after successful heart 25. 26. 27. 28. 29. 30. 31. 32. 33. transplantation resolves controversial intraoperative findings and reveals complex hemodynamic alterations. Circulation 2011;123:e381 –3. Eriksson J, Carlhall CJ, Dyverfeldt P, Engvall J, Bolger AF, Ebbers T. Semi-automatic quantification of 4D left ventricular blood flow. J Cardiovasc Magn Reson 2010;12:9. Roes SD, Hammer S, van der Geest RJ, Marsan NA, Bax JJ, Lamb HJ et al. Flow assessment through four heart valves simultaneously using 3-dimensional 3-directional velocity-encoded magnetic resonance imaging with retrospective valve tracking in healthy volunteers and patients with valvular regurgitation. Invest Radiol 2009;44:669 –75. Lakatta EG, Levy D. Arterial and cardiac aging: major shareholders in cardiovascular disease enterprises: part II: the aging heart in health: links to heart disease. Circulation 2003;107:346 –54. Föll D, Jung B, Schilli E, Staehle F, Geibel A, Hennig J et al. Magnetic resonance tissue phase mapping of myocardial motion—new insights in age and gender magnetic resonance tissue phase mapping of myocardial motion- new insights in age and gender. Circ Cardiovasc Imaging 2010;3:54–64. Föll D, Jung B, Staehle F, Schilli E, Bode C, Hennig J et al. Visualization of multidirectional regional left ventricular dynamics by high-temporal-resolution tissue phase mapping. J Magn Reson Imaging 2009;29:1043 –52. Markl M, Kilner PJ, Ebbers T. Comprehensive 4D velocity mapping of the heart and great vessels by cardiovascular magnetic resonance. J Cardiovasc Magn Reson 2011;13:7. Markl M, Harloff A, Bley TA, Zaitsev M, Jung B, Weigang E et al. Time-resolved 3D MR velocity mapping at 3T: improved navigator-gated assessment of vascular anatomy and blood flow. J Magn Reson Imaging 2007;25:824 – 31. Griswold MA, Jakob PM, Heidemann RM, Nittka M, Jellus V, Wang J et al. Generalized autocalibrating partially parallel acquisitions (GRAPPA). Magn Reson Med 2002;47:1202 – 10. Walker PG, Cranney GB, Scheidegger MB, Waseleski G, Pohost GM, Yoganathan AP. Semiautomated method for noise reduction and background phase error correction in MR phase velocity data. J Magn Reson Imaging 1993;3: 521 –30. Bernstein MA, Zhou XJ, Polzin JA, King KF, Ganin A, Pelc NJ et al. Concomitant gradient terms in phase contrast MR: analysis and correction. Magn Reson Med 1998;39:300 –8. Bock J, Kreher BW, Hennig J, Markl M. Optimized pre-processing of time-resolved 2D and 3D phase contrast MRI data. In Proceedings: 15th Scientific Meeting International Society for Magnetic Resonance in Medicine Berlin, Germany 2007; p. 3138. Bellhouse BJ. Fluid mechanics of a model mitral valve and left ventricle. Cardiovasc Res 1972;6:199 – 210. Sengupta PP, Khandheria BK, Korinek J, Jahangir A, Yoshifuku S, Milosevic I et al. Left ventricular isovolumic flow sequence during sinus and paced rhythms: new insights from use of high-resolution Doppler and ultrasonic digital particle imaging velocimetry. J Am Coll Cardiol 2007;49:899 – 908. Hong G, Pedrizzetti G, Tonti G, Li P, Wei Z, Kim JK et al. Characterization and quantification of vortex flow in the human left ventricle by contrast echocardiography using vector particle image velocimetry. JACC Cardiovasc Imaging 2008;1: 705 –17. Kim WY, Walker PG, Pedersen EM, Poulsen JK, Oyre S, Houlind K et al. Left ventricular blood flow patterns in normal subjects: a quantitative analysis by threedimensional magnetic resonance velocity mapping. J Am Coll Cardiol 1995;26: 224 –38. Germans T, Gotte MJW, Nijveldt R, Spreeuwenberg MD, Beek AM, Bronzwaer JGF et al. Effects of aging on left atrioventricular coupling and left ventricular filling assessed using cardiac magnetic resonance imaging in healthy subjects. Am J Cardiol 2007;100:122–7. Gentile F, Mantero A, Lippolis A, Ornaghi M, Azzollini M, Barbier P et al. Pulmonary venous flow velocity patterns in 143 normal subjects aged 20 to 80 years old. An echo 2D colour Doppler cooperative study. Eur Heart J 1997;18: 148 –64. Daimon M, Watanabe H, Abe Y, Hirata K, Hozumi T, Ishii K et al. Gender differences in age-related changes in left and right ventricular geometries and functions. Echocardiography of a healthy subject group. Circ J 2011;75:2840 –6. Redfield MM, Jacobsen SJ, Borlaug BA, Rodeheffer RJ, Kass DA. Age- and genderrelated ventricular-vascular stiffening: a community-based study. Circulation 2005; 112:2254 –62. Geiger J, Markl M, Herzer L, Hirtler D, Loeffelbein F, Stiller B et al. Aortic flow patterns in patients with Marfan syndrome assessed by flow-sensitive fourdimensional MRI. J Magn Reson Imaging 2012;35:594 – 600.