Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Compounding wikipedia , lookup
Discovery and development of cyclooxygenase 2 inhibitors wikipedia , lookup
Plateau principle wikipedia , lookup
Drug design wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Prescription drug prices in the United States wikipedia , lookup
Drug discovery wikipedia , lookup
Pharmacognosy wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Psychopharmacology wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Neuropharmacology wikipedia , lookup
Prescription costs wikipedia , lookup
Theralizumab wikipedia , lookup
Drug interaction wikipedia , lookup
Dydrogesterone wikipedia , lookup
Discovery and development of beta-blockers wikipedia , lookup
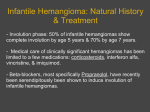
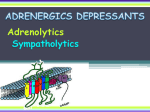
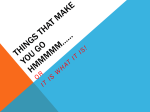
SPECIAL ARTICLE Clinical Pharmacology of Propranolol By ALAN S. NIES, M.D., AND Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 ONE OF THE more significant advances in cardiovascular therapeutics in the past decade has been the introduction of 3-adrenergic blocking drugs. This review is prompted by the expanding indications and more widespread use of this group of drugs. Although several compounds have been developed, propranolol was the first to gain wide acceptance and remains the only one available for general use in the United States. We shall therefore concentrate on the clinical pharmacology of propranolol and make only passing reference to some of the other drugs which, in time, will undoubtedly become available. DAVID G. SHAND, M.D. the systemic circulation has been termed presystemic (or "first pass") hepatic elimination. Because of this effect, the disposition of propranolol is critically dependent on the route of administration. We shall therefore consider the determinants of propranolol concentrations in the blood after intravenous administration before discussing the more complex situation that arises following oral administration. Intravenous Administration The three major biological determinants of propranolol disposition are the activity of the drug metabolizing enzymes in the liver, hepatic blood flow, and plasma-drug binding. The hepatic uptake process is so great that the hepatic extraction ratio for the drug is very large after intravenous administration of normal therapeutic doses. An hepatic extraction in excess of 90% has been demonstrated directly in the dog2 and by inference in man, as its clearance from the blood (about 1.2 L/min) approaches a value for hepatic blood flow.3 This very high hepatic extraction results in a drug half-life in man of two to three hours after an i. v. dose. The apparent volume of distribution in blood is about 250 L. The relationship between drug clearance (Cl), apparent volume of distribution (Vd), and half-life (T½/2) is given by Determinants of Circulating Drug Concentration A fundamental principle of pharmacology is that a drug's effect is a function of its concentration at the receptor. However, when a given dose is administered to patients, several factors govern the amount of drug that eventually reaches its site of action which may vary considerably from patient to patient. These dispositional factors of absorption, distribution, and elimination therefore become as important therapeutically as does the effectiveness of the drug itself. For this reason great emphasis has recently been placed on measuring plasma drug concentrations, as these are generally in equilibrium with drug at the receptors. In the case of propranolol, it was soon recognized that some six to ten times larger doses were required by mouth to match the effects of intravenously administered drug. This occurs despite complete absorption across the gut' and is an unavoidable consequence of the fact that the liver is the major organ of elimination and removes drug from the portal blood before it can ever reach the systemic circulation, and thence its target organs. The removal of drug by the liver during its transfer from the gut to Cl = Vd x 0T693 Because of the very high hepatic extraction ratio of propranolol, its clearance is sensitive to alterations in hepatic blood flow.4 Since the beta-blocking effects of propranolol result in reduced cardiac output,5 hepatic blood flow is lowered during administration of this drug and hepatic elimination is reduced.5 Thus dlpropranolol, by its pharmacologic action, affects its own clearance by decreasing delivery of drug to the liver. Dextro-propranolol, which does not affect hepatic blood flow, is cleared more rapidly in the unanesthetized monkey than the racemate.4 This effect may explain the shorter half-life of d-propranolol than dl- or 1-propranolol in man.6 It has also been shown that propranolol can decrease the elimination of other highly extracted compounds, like lidocaine, by reducing hepatic blood flow.7 Although only investigated in From the Division of Clinical Pharmacology, Departments of Medicine and Pharmacology, Vanderbilt University Medical School, Nashville, Tennessee. Supported in part by Public Health Service Grant GM 15431. Address for reprints: Dr. Alan S. Nies, Division of Clinical Pharmacology, Departments of Medicine and Pharmacology, Vanderbilt University Medical School, Nashville, Tennessee 37232. 6 Circulation, Volume 52, July 1975 CLINICAL PHARMACOLOGY OF PROPRANOLOL Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 animals so far, such hemodynamic drug interactions are of likely clinical relevance, especially in patients requiring acute intensive care with cardioactive drugs given intravenously.8 The effect of plasma-binding of propranolol on drug elimination differs from the traditional teaching that decreased plasma-binding shortens half-life by increasing free drug concentration available for metabolism. With propranolol, the hepatic extraction ratio greatly exceeds the free drug fraction, and thus both bound and free forms are available for metabolism and are extracted from plasma by the liver. With such nonrestrictive elimination, total drug clearance is unaffected by binding in the circulation and half-life is proportional to the "volume of distribution" which is an index of tissue stores of a drug. The volume of distribution of propranolol increases as plasma-binding decreases because more drug escapes from the plasma into the tissues. Plasma-binding thus acts as a drug delivery system to the liver, and low propranolol plasma-binding lengthens half-life, and conversely, high binding shortens half-life.9' 10 Oral Administration As a result of the anatomical arrangement of its portal circulation, the liver can remove drug from the portal venous blood during its transfer from the gut to the systemic circulation (fig. 1). The fraction of the dose removed during presystemic hepatic elimination is equal to the hepatic extraction ratio, E, so that the fraction that passes on into the systemic circuit is given by (1 - E). The greater the extraction ratio, the smaller will be the fraction of the dose that is available to produce systemic effects. This fraction is termed the bioavailability of the drug. Drugs with high extractions, like propranolol, can therefore never be fully 7 bioavailable even though their alimentary absorption is complete. As might be predicted from its very high clearance after i.v. administration, the availability of small single oral doses of propranolol is very small. However, as the single oral dose is increased above about 30 mg, the avid removal process becomes saturated and hepatic extraction falls, resulting in a larger fraction of an oral dose reaching the systemic circulation and a longer half-life, of three to six hours, in normal subjects.3 Furthermore, this avid hepatic uptake remains saturated throughout the usual sixhour dosage interval, so that drug concentrations in the blood accumulate during chronic oral administration." Finally, when steady state is reached during continuous oral administration, drug concentrations are essentially proportional to dose, in contrast to the situation following single oral doses.3 However, even during chronic oral administration of the hepatic extraction is still relatively high (0.5-0.8) so that only 20-50% of the dose reaches the systemic circulation. Not only is the bioavailability low but it is highly variable among patients. Plasma levels after oral administration vary more widely than those after intravenous administration in the same subjects. 12 In our clinical practice 20-fold differences in plasma concentration have been seen at the end of the dosage interval in patients receiving the same oral dose (fig. 2). Again, this is a necessary consequence of the large presystemic elimination that occurs with highly extracted drugs.` Thus, compared to patients with low hepatic extraction ratios, those with higher extraction ratios not only permit less drug to reach the systemic circulation but also clear the drug more efficiently, resulting in even lower concentrations than the differences in extraction ratio might suggest. 1 L LIVER INTRAVENOUS -V E RF . . . (1 . ORAL Figure 1 Presystemic "first pass" effect. A diagrammatic representation of intravenous and oral administration of propranolol. The shading represents drug concentration and the arrows represent route of administration. Since the major organ of elimination is the liver, the drug can be extracted from portal venous blood prior to reaching the systemic circulation during oral administration. Circulation, Volume 52, July 1975 NIES, SHAND 8 600 C7 c 1 0 400 0 0 z 1 0 0 0 (I) a 200 0* n_ o 1 I S 0l 0 40 20 6-HOURLY DOSE,mg Figure 2 80 Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 Plasma propranolol levels (ng/ml) obtained during various doses of the drug orally. Each dot represents the level of a single patient. Note the wide range of values at a given dose. Drug Half-life and Duration of Action Perhaps one of the most important uses of pharmacokinetic data is in devising appropriate dosage regimens on the basis of drug half-life. There has been some confusion concerning the relationship of duration of action and half-life of beta-adrenergic blocking drugs. Duration of action is determined by the dose administered (or initial plasma concentration) as well as by drug half-life. Furthermore, drug effect and plasma concentrations do not necessarily decline in parallel. In the case of beta-blockade with practolol14 and propranolol after intravenous administration,` the reduction in exercise heart rate is a function of the logarithm of the plasma concentration. Thus, this effect declines as a linear function of time as the plasma concentration declines exponentially (i.e., first order). It is therefore to be expected that drug effect should decline less rapidly than plasma concentration when exercise tachycardia is used to judge efficacy. On the other hand, the efficacy of propranolol can be determined from the antagonism of isoproterenol-induced tachycardia. This antagonism is competitive and therefore can be overcome by increasing isoproterenol dosage, that is, the dose/response curve for isoproterenol is shifted to the right in parallel fashion by propranolol. Such an effect can be quantified by calculation of the dose ratio (DR) for isoproterenol (the dose needed for a given response in the presence of propranolol divided by that found under control conditions). When betaadrenergic blockade is defined by the dose ratio to isoproterenol (DR), then log (DR-1) is a function of log plasma propranolol concentration.'6 In this case (DR-1) theoretically falls in parallel with plasma con- centration and both decline exponentially with time consistent with the data of Paterson et al.' It should be mentioned that over the range of dose ratios usually achieved clinically, a plot of dose ratio against log plasma concentration is in fact essentially linear,'5 and deviations appear only at low drug concentrations.17 While these considerations may seem somewhat esoteric, they do serve to show how an inappropriate measure of drug efficacy can lead to erroneous conclusions concerning the duration of drug action. It may be concluded that, excluding the effects of active metabolites, there is no evidence that the effects of beta-adrenergic blockade become dissociated from the plasma drug levels, and it is generally accepted that patients should be maintained at minimally effective plasma levels at the end of a dosage interval. The half-life of propranolol in normal subjects depends on the route and duration of drug administration but is always short and rarely exceeds six hours. Accordingly, the recommended oral dosage interval was set at about six hours. Although few systematic studies have been made, there are several reasons to believe that longer intervals with larger doses could be used, so that effective levels would still be present at the time another dose is administered, with the proviso that the higher peak levels were not associated with toxicity. Since occurrence of toxicity is not related to dosage, it would seem possible to administer the drug less often to individual patients, especially when compliance is a problem. Indeed investigators have recently found adequate antihypertensive effect with twice daily propranolol administration. 18, 19 Interest in the duration of beta blockade has heightened recently with the suggestion by Viljoen et al.20 that the effect of propranolol may take some time to dissipate and that coronary artery surgery is unsafe for two weeks after withdrawal. While their opinion is shared by some, others have disagreed.2' 22 Two groups have investigated this problem in surgical patients. Faulkner et al.23 could not detect propranolol or note any effects on atrial muscle response to norepinephrine 48 hours after drug withdrawal. These findings were extended by Coltart et al.24 who showed that neither metabolites nor the drug were detectable as early as 12-24 hours postwithdrawal. More important perhaps are several anecdotal reports that severe arrhythmia, angina, and even infarction can occur following withdrawal. 25-27 The important question may well be whether it is advisable to discontinue propranolol at all in such cases. Until the argument is resolved each case should be treated individually and drug withdrawal carefully monitored in a hospital. If the patient's condition worsens it may well be safer to Circulation, Volume 52, July 1975 CLINICAL PHARMACOLOGY OF PROPRANOLOL operate while minimally effective doses of propranolol are present. Effects of Disease Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 An important consideration in drug elimination is the presence of disease. In the case of propranolol, drug half-life is known to be prolonged by a reduction in liver blood flow, decreased activity of the hepatic enzymes, and by reduced plasma drug-binding. Patients with heart failure and liver disease should be expected to handle the drug abnormally, though it is recognized that the drug is contraindicated in heart failure. In patients with liver disease, propranolol half-life is variable: it may be relatively normal or prolonged to as much as 35 hours in cirrhotic patients with surgically-induced portocaval anastomoses and reduced plasma drug-binding.3 In addition, such patients will have very high oral bioavailability of drugs such as propranolol since the presystemic hepatic elimination is bypassed by the porto-systemic shunt. In the presence of renal disease half-life is relatively unaffected and in some cases is even shortened.28 The shortened half-life and higher plasma concentrations reported in renal failure29 probably reflect a reduced volume of distribution resulting from loss of muscle mass. Drug Concentration and Effect The most important clinical problem is that of the very great variation in propranolol dosage required in patients being treated for the same condition. For example, patients with angina and hypertension may require as much as 2000 mg daily, while some respond to as little as 40 mg. If we can determine that variable bioavailability accounts for the wide range of dosage required for clinical effect, the question of appropriate dosage could be answered by monitoring plasma concentrations and adjusting the dose accordingly. In order to establish a therapeutic range of plasma propranolol concentration we must examine the evidence showing that the effects of propranolol are indeed a function of its plasma concentration and exclude other explanations for dosage variation such as the involvement of active metabolites and differences in receptor sensitivity. Finally and most important, the mechanism of action of the drug in treating a diversity of conditions must be considered, as it is by no means established that all the drug's effects are the result of peripheral beta-blockade. Beta-adrenergic Blockade In attempting to relate plasma concentrations of an antagonist drug like propranolol to its effects, a suitable test stimulus is required. Both isoproterenol and exercise-induced tachycardia have been investigated. 17-1, 30-38 Several groups have demonstrated Circulation, Volume 52, July 1975 9 that the isoproterenol dose ratio, i.e., the amount of shift of the isoproterenol dose-response curve, is a predictable function of plasma propranolol concentration.16' 31 This test procedure has been standardized32 and is useful to determine relative potencies for comparison of beta-adrenergic blocking drugs, but suffers the disadvantage that there is no fixed end point because there is no limit to the amount of isoproterenol that can be given. Thus, with isoproterenol as the stimulus, the dose ratio becomes a continuous variable within the limits of toxicity of the antagonist. For endogenous stimuli, there should be a limit to the degree of beta-adrenergic stimulation achievable. It was therefore important to assess the effects of beta blockers on an endogenous beta-adrenergic stimulus, and exercise-induced tachycardia was investigated by Coltart and Shand who compared the effects of three doses of propranolol and a placebo.15 They demonstrated that there was a maximum attainable degree of blockade in the sense that increasing the dose of propranolol produced no further reduction in heart rate at all exercise grades studied.15 As might be expected from a competitive antagonist, the effects of a submaximal dose of propranolol could be overcome by increasing the severity of the exercise, that is, more drug would be required to produce a given effect in subjects who exercise more strenuously. Although this was clearly a cause of individual variation in dose requirements, doubling the submaximal dose was sufficient to give a maximal effect in each case. The study by Coltart and Shand showed that there was a straight line relationship between block of exercise tachycardia and the log of plasma propranolol concentration, but that the propranolol level associated with a given effect two hours after a single oral dose was one half that required after intravenous administration. 15 A ready explanation for this discrepancy is available from the data of Paterson et al.1 who showed that an active metabolite of propranolol, 4-hydroxypropranolol, can be detected in the plasma only after oral administration. This metabolite is not measured by the standard propranolol assay, but since it is equipotent to propranolol34 and achieves approximately the same circulating concentrations as the parent drug shortly after an oral dose,' the effects of the metabolite will add to those of propranolol. Thus the presence of this metabolite produced after single oral, but not intravenous doses, of propranolol can account for the twofold difference in effective propranolol concentration by the two routes of administration. While the presence of an active metabolite clearly makes interpretation of plasma concentrations of the parent drug difficult, recent evidence suggests that this may not be a problem with NIES, SHAND 10 Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 the clinical use of propranolol. Thus, 4-hydroxypropranolol has a shorter half-life than propranolol' so that by the end of a six hour dosage interval all of the effects of a single dose of the drug can be accounted for by the parent compound.3' In addition, during chronic oral administration, propranolol accumulates in the plasma, and as early as two hours after the dose, most of the resultant effect can be accounted for by propranolol itself. If an active metabolite is present, its contribution to beta-adrenergic blockade is minor.3' This is supported by the data of Bodem et al.'6 who found levels of at least 100 ng/ml were required for maximal effect after chronic oral administration, the same amount that is required after i.v. administration in which no active metabolite can be detected in plasma. While it is the consensus that there is a clear relationship between plasma propranolol concentration and effect in any given individual, there is some interindividual variation in the plasma level required to produce a given effect. For example, George et al.33 found as much as a fourfold difference in normals. Zacest and Koch-Weser'7 have described two populations of hypertensive patients, one of which required 2.5 times the propranolol concentration to achieve comparable isoproterenol antagonism during chronic oral administration, in spite of the fact that within each population the correlation between drug concentration and effect was excellent. The less sensitive subjects also tended to show higher plasma levels with a given oral dose, and it was suggested that they might produce less 4-hydroxypropranolol. 17 While this conclusion seems unlikely in view of the literature already cited, a final judgment will only be possible if a dependable technique of measuring this unstable active metabolite becomes available. Variations in receptor sensitivity might also be a cause of the interindividual variation, and George et al.35 have shown that after i.v. administration in dogs, when no 4-hydroxypropranolol was present and plasma propranolol concentrations were comparable, those animals most sensitive to isoproterenol were also most sensitive to propranolol. Another explanation for differences in response to a given plasma level of propranolol is variation in plasma drug-binding. Data obtained from cardiac tissue in vitro suggest that with propranolol, as with other drugs, only the unbound fraction of drug has access to the receptor and is active (Faulkner, Boerth and Shand, unpublished observations). In man the bulk (> 90%) of propranolol in plasma is proteinbound and hence inactive, and yet both free and bound propranolol are measured by the plasma propranolol assay. Small differences in plasmabinding can result in substantial variation in free drug concentration. In normal subjects the plasma binding of propranolol varies from 90% to 95%.9 While this may seem a trivial individual difference, in fact the free or active drug will vary from 5% to 10%, and this twofold variation is a factor which might account for a modest individual variation in the effectiveness of a given total drug concentration. Therapeutic Effects Finally, we should consider the evidence that all the effects of propranolol have a common mechanism. In this context plasma drug concentration measurements can supply valuable clues. Animal studies have shown that propranolol can decrease the rate of rise of the cardiac action potential, an effect which has been described as nonspecific myocardial depression or "quinidine-like" activity and this property is often quoted as contributing to the antiarrhythmic effect of the drug clinically. However, evidence is available that these nonspecific effects do not contribute importantly to the therapeutic or adverse effects with propranolol in man. In vitro data indicates that 10,000 ng/ml are required to slow the rate of rise of the action potential of human papillary muscle.36 As plasma drug binding in vivo would lower effective free concentrations by a factor of 10-20, it would seem that the quinidine-like effect requires concentrations two or three orders of magnitude higher than those giving beta-blockade, and such concentrations are unlikely to ever occur in patients even with the largest doses employed clinically. Supportive evidence is obtained from the use of the d-isomer of propranolol which is devoid of betablocking properties yet which retains the nonspecific "quinidine-like" effects.36 Coltart et al.37 found that four patients who had responded to i.v. infusion of dlpropranolol with abolition of premature ventricular beats failed to respond to the d-isomer even though higher plasma concentrations were achieved (60-75 ng/ml with dl-propranolol compared with 180-310 ng/ml with d-propranolol: fig. 3). The failure of dextro-propranolol to suppress ventricular ectopic beats follows published experience with dextroisomers of other beta-adrenergic blocking drugs38 and with the antiarrhythmic efficacy of beta-adrenergic blocking drugs which do not have quinidine-like effects.39 The findings conflict, however, with the results of Howitt et al.40 who reported that racemic and dextro-propranolol had approximately equivalent effects on supraventricular and ventricular ectopic beats and tachycardia. The reason for this discrepancy is not clear, but it may reflect differences in the etiology of the arrhythmias studied or the criteria by which effectiveness was assessed. Nevertheless, the over-all results support the conclusion that proCirculation, Volume 52, July 1975 CLINICAL PHARMACOLOGY OF PROPRANOLOL F DL- PROPRANOLOL SUCCESS FAI LURE D-PROPRANOLOL SUCCESS FAILURE z 11 model the quinidine-like effects are probably important. However the fact that the doses used are much higher than those effective in man46 indicates that extrapolation of findings in acute digitalis toxicity in animals to those appearing during chronic administration of the glycosides in man should be done only with great caution. 0 z 24 01 C,) -Jr 0: F- CLL Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 ;g 3 ir 4 W :c Figure 3 Effect of d-propranolol (circles) or dl-propranolol (triangles) on ventricular contractions. Dl-propranolol was infused intravenously until the arrhythmia was abolished (closed symbols) or until 20 mg was given. Plasma levels were obtained when the arrhythmia was abolished or at the end of the infusion. In four patients responding to dl-propranolol, d-propranolol was infused to a dose of 40 mg intravenously with no effect on the arrhythmia. Plasma levels obtained are in the upper half of the figure. Sinus rate at rest is in the lower half of the figure. The slowing of sinus rate is indicative of 3-adrenergic blockade which does not occur with dpropranolol. premature pranolol is an antiarrhythmic drug of clinical importance by virtue of its beta-adrenergic blocking activity, and that its nonspecific effects play no more than a minor part. A similar conclusion can be reached in other situations for which propranolol is used. Dextropropranolol is not effective in angina or hypertension41' 42 while beta-adrenergic blockers without quinidine-like activity are effective.41 43- These considerations also support the contention that the nonspecific cardiac depressant effects contribute little to precipitation of heart failure in patients. Rather, the drug's action in blocking reflex beta-adrenergic stimulation which compensates for incipient failure is an effect of any beta-adrenergic blocker and not related to nonspecific effects. It should be mentioned that in animals the i.v. doses of dl- and d-propranolol required to reverse acute ouabain-induced arrhythmias are about the same (1-3 mg/kg), and in this Circulation, Volume 52, July 1975 Hypertension is another condition in which consideration of dose is important and in which mechanism of action is unclear. There is little doubt that propranolol is an effective antihypertensive in patients with essential hypertension, and offers the great advantage of lowering both supine and standing pressure equally. There is a great deal of controversy, however, as to the mechanism of action and the type of patients likely to respond. Recently, Buhler et al.47' 48 suggested that patients with initially high renin activity responded best to modest doses (average 240 mg daily) and that the antihypertensive effect was related to the reduction of plasma renin activity that the drug produces. Although plasma propranolol concentrations were not measured, the doses used would likely be associated with levels of about 100 ng/ml levels which were found by Michelakis and McAllister49 to be associated with lowered plasma renin activity (PRA). Despite the enormous appeal of this specific approach to the treatment of a definable subset of hypertensives, there is some contradictory evidence. Several workers have failed to confirm specificity, in that the hypotensive effects of the drug were not associated with the fall in PRA.50 Further, the large clinical experience in Europe51"53 suggests that most patients will respond provided large enough doses are given (up to 2000 mg daily). There are several explanations for the need of high doses in some patients. Either compliance was poor, the patients were inadvertently overtreated, or large doses were required to give the high plasma levels needed to produce hypotension by an effect other than that on PRA. Failure to comply has been ruled out in eight patients selected from Prichard's experience whose blood pressure was controlled with 400-2000 mg daily as outpatients, in that high plasma levels, from 125-2000 ng/ml, were measured (Prichard and Shand, unpublished observations). Consideration of all the available data suggests that propranolol may have two modes of action as an antihypertensive one lowering PRA level and one acting on the central nervous system. Recently, some evidence has been accumulating in animals that propranolol may act on the central nervous system to produce hypotension.54' ` Lowering of PRA requires only modest doses giving plasma levels in the range of 50-100 ng/ml. A similar, peripheral effect potentiates NIES, SHAND 12 Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 the action of hydralazine by preventing the reflex tachycardia and PRA elevation56 and that of diuretics by limiting the consequent rise in PRA.`7 The possible effect on the central nervous system may require high doses and is presumably capable of lowering pressure in patients with low plasma renin levels. While definitive studies are still required, the hypothesis is attractive since its confirmation would resolve the apparent conflict in the data. In the case of the treatment of angina pectoris, it is unclear why some patients obtain further relief from doses larger than necessary to produce effective beta blockade.58 It is interesting that angina, hypertension, and arrhythmia are not disease entities but rather signs and symptoms which are likely associated with variable pathophysiology and the elucidation of the mechanism of action of a drug like propranolol may provide clues to the underlying disease process and aid in the definition of subsets of patients with a common syndrome. While the multiple effects of the factors that have been discussed make it difficult to define a therapeutic plasma propranolol concentration with great precision, all the published data would suggest that 100 ng/ml should confer a very high degree of blockade of cardiac receptors and will be essentially maximal for some patients. Significant beta blockade is produced by lower propranolol levels which appear to be sufficient for therapeutic effects in many patients. If plasma levels are measured at the end of a dosage interval, these should represent the low end of the range of plasma levels and should not be affected by the presence of 4-hydroxypropranolol, which will probably have dissipated. Similar concentrations in the range of 50-100 ng/ml have been associated with reduction in plasma renin activity,49 prevention of reflex tachycardia due to hydralazine,7' 56 abolition of sensitive ventricular arrhythmias,37 alleviation of anginal pain,59 60 mild hypertension,17' 56 and in patients with hypertrophic cardiomyopathy.61-62 A further fact in support of this therapeutic range is that in all conditions save hypertension, propranolol is effective after the intravenous administration of modest doses (1-5 mg) which actually give lower plasma concentrations than those recommended. Finally, of all the variables, differences in bioavailability appear to be the greatest and therefore probably the most important in determining variable dosage requirements. Adverse Reactions The adverse reactions to propranolol are not related to dose63' 64 but appear with small doses early in the course of treatment. Thereafter, dosage can usually be increased without fear of dramatic or sudden toxicity. The life-threatening adverse reaction is one of sudden and profound hypotension resulting from heart failure or heart block. As mentioned, such an effect results from the sudden blockade of reflex sympathetic tone which has maintained cardiac output in the face of a failing myocardium. It is most commonly seen following rapid i.v. administration in the intensive care of very sick patients. Until recently, the use of propranolol in acute myocardial infarction was therefore contraindicated. However, experimental data in animals has suggested that beta-adrenergic blockade may reduce the size of infarction.`6 Clinically, however, early results on the effects of propranolol on mortality in the presence of myocardial infarction were conflicting and this whole area is the subject of intensive investigation. Until the problem is resolved we feel that propranolol should be avoided in this situation. The greater safety of other beta-adrenergic blocking drugs has received much publicity, some, in our opinion, unjustified. Two of the pharmacological properties other than beta-blockade that have been considered important are intrinsic sympathomimetic (or partial agonist) activity and quinidine-like effects. We have already discussed the fact that the clinical effects, both positive and negative, of quinidine-like action are probably unimportant. The quinidine-like action of these drugs may play at most a minor role in the development of heart failure. While intrinsic activity of some drugs has been shown, since tachycardia in reserpinized animals can be produced, a positive chronotropic effect has never been shown in man. In addition, there is also an excellent correlation between reduction in rate and cardiac output, irrespective of whether the drug used shows this property or not.66 The one exception is practolol, which is relatively cardio-selective with less influence on peripheral receptors in the circulation and in the bronchial smooth muscle. With practolol, there is almost no reduction in cardiac output at rest though bradycardia is obvious.66 Whether this favorable property results from intrinsic activity or cardio-selectivity is unclear. Intrinsic activity does not appear to be important to the pharmacology of nonselective agents, and in fact, cardiac output is lowered by another cardio-selective agent, ICI 66082. At the present time, it is impossible to make a judgment on the possible role that some of the newer agents may play. Certainly they all appear effective in the same conditions. In terms of safety, all the evidence suggests that profound cardiovascular collapse is due to beta-blockade, a property that is shared by all nonselective drugs, and that lack of appearance of this serious side effect with these newer agents is due as much to the fact that i.v. administration in sick patients is now avoided as to their particular pharmacology. The one clearly desirable Circulation, Volume 52, July 1975 CLINICAL PHARMACOLOGY OF PROPRANOLOL property is cardioselectivity which allows betablocking drugs to be used in asthma. Whether other subtle differences in the properties of these agents will make them more desirable as therapeutic agents remains to be seen. Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 Summary This review of recent developments in the clinical pharmacology of beta-adrenergic blocking drugs has emphasized the individual variability in patient response and how a knowledge of drug disposition can provide some explanation for this. Plasma level estimates may be helpful in overcoming these variables and can be of some help clinically, provided their limitations are clearly understood, and they are not used to replace accurate clinical assessment in the individualization of patient therapy. From the practical point of view, treatment should be started with small doses (e.g., 40-80 mg daily), which can be increased stepwise until the desired effect is obtained or until 320 mg daily are administered. If only a partial response has been obtained (for example, in the treatment of angina), it would seem reasonable to increase the dose further. If there has been little or no effect, then a plasma concentration determination at the end of the usual dosage interval may be useful. Levels at this time of 100 ng/ml or greater are strongly suggestive of a therapeutic failure inasmuch as this represents a very high degree of beta-adrenergic blockade and therapeutic effects are usually seen at plasma levels below this level. Several alternate drugs are available for the treatment of arrhythmias or hypertension and surgery can be considered in the case of angina and obstructive cardiomyopathy. In this context it should be emphasized that in only two rare conditions (i.e., arrhythmia due to pheochromocytoma and obstructive cardiomyopathy) can propranolol be considered the drug of first choice. If plasma levels of less than 100 ng/ml are found, then poor bioavailability or lack of compliance are possible causes of apparent therapeutic failure and may be distinguished by increasing the dosage when failure to increase plasma concentration may indicate poor compliance. In the treatment of hypertension, it would seem premature not to try diuretics as a first choice of treatment or to confine the drug's use to those patients with high plasma renin activity. At the present time we would favor adding hydralazine to the regimen in patients who had failed to respond to propranolol at a plasma concentration of 100 ng/ml. This should be sufficient to overcome the reflex effects of the vasodilator and avoids the problem of poor patient compliance when very large doses are administered. However, should the hypothesis that high plasma Circulation, Volume 52, July 1975 13 renin activity be associated with increased cardiovascular morbidity and mortality67 be confirmed, then the ability of propranolol to lower plasma renin may make it a most desirable therapy irrespective of its hypotensive effects. References 1. PATERSON JW, CONOLLY ME, DOLLERY CT, HAYES A, COOPER RG: The pharmacodynamics and metabolism of propranolol in man. Pharmacologia Clinica 2: 127, 1970 2. SHAND DG, EVANS GH, NIES AS: The almost complete hepatic extraction of propranolol during intravenous administration in the dog. Life Sci 10: 1417, 1971 3. SHAND DG, RANGNO RE: The disposition of propranolol. Elimination during oral absorption in man. Pharmacology 7: 159, 1972 4. NIEs AS, EVANS GH, SHAND DG: The hemodynamic effects of beta-adrenergic blockade on the flow-dependent hepatic clearance of propranolol. J Pharmacol Exp Ther 184: 716, 1973 5. NIEs AS, EVANS CH, SHAND DG: Regional hemodynamic effects of beta-adrenergic blockade with propranolol in the unanesthetized primate. Am Heart J 85: 97, 1973 6. GEORGE CF, FENYVESI T, CONOLLY ME, DOLLERY CT: Pharmacokinetics of dextro, laevo and racemic propranolol in man. Eur J Clin Pharmacol 4: 74, 1972 7. BRANCH RA, SHAND DG, WILKINSON GR, NIES AS: The reduction of lidocaine clearance by dl-propranolol: An example of hemodynamic drug interaction. J Pharmacol Exp Ther 184: 515, 1973 8. NIEs AS, SHAND DG, BRANCH RA: Hemodynamic drug interactions: The effects of altering hepatic blood flow on drug disposition. In Drug Interactions, edited by MORSELLI PL, GARATTINI S, COKER SN. New York, Raven Press, 1974, pp 231-240 9. EVANS GH, SHAND DG: Disposition of propranolol. VI. Independent variation in steady state circulating drug concentration and half-life as a result of plasma drug binding in man. Clin Pharmacol Ther 14: 494, 1973 10. EVANS GH, NIES AS, SHAND DG: The disposition of propranolol, III, decreased half-life and volume of distribution as a result of plasma binding in man, monkey, dog and rat. J Pharmacol Exp Ther 186: 114, 1973 11. EVANS GH, SHAND DG: Disposition of propranolol. V. Drug accumulation and steady-state concentrations during chronic oral administration in man. Clin Pharmacol Ther 14: 487, 1973 12. SHAND DG, NUCKOLLS EM, OATES JA: Plasma propranolol levels in adults. Clin Pharmacol Ther 11: 112, 1970 13. ROWLAND M: Influence of route of administration on drug availability. J Pharm Sci 61: 70, 1974 14. CARRUTHERS SG, KELLY JG, McDEVITT DG, SHANKS RG: Blood levels of practolol after oral and parenteral administration and their relationship to exercise heart rate. Clin Pharmacol Ther 15: 497, 1974 15. COLTART DJ, SHAND DG: Plasma propranolol levels in the quantitative assessment of beta-adrenergic blockade in man. Br Med J 3: 721, 1970 16. BODEM G, BRAMMELL HL, WEIL JV, CHIDSEY CA: Pharmacodynamic studies of beta-adrenergic antagonism induced in man by propranolol and practolol. J Clin Invest 52: 747, 1973 17. ZACEST R, KOCH-WESER J: Relation of propranolol plasma level to beta-blockade during oral therapy. Pharmacology 7: 178, 1972 NIES, SHAND 14 Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 18. WILKINSON PR, DIXON N, HUNTER KR: Twice-daily propranolol treatment for hypertension. J Intern Med Res 2: 220, 1974 19. BERGLUND G, ANDERSSON 0, HANSSON L, OLANDER R: Propranolol given twice daily in hypertension. Acta Med Scand 194: 513, 1973 20. VILJOEN JF, ESTAFANOUS F, KELLNER GA: Propranolol and cardiac surgery. J Thorac Cardiovasc Surg 64: 826, 1972 21. KOPRIVA CJ: Anesthesia and propranolol. N Engl J Med 290: 1205, 1974 22. CARALPS JM, MULET J, WIENKE R, MORAN JM, PIFARRE R: Results of coronary artery surgery in patients receiving propranolol. J Thorac Cardiovasc Surg 67: 525, 1974 23. FAULKNER SL, HOPKINS JT, BOERTH RC, YOUNG JL, JELLETT LD, NIES AS, BENDER HW, SHAND DC: Time required for complete recovery from chronic propranolol therapy. N Engl J Med 289: 607, 1973 24. COLTART DJ, CAYEN MN, STINSON EB, DAVIES RO, HARRISON DC: Determination of the safe period for withdrawal of propranolol therapy. Circulation 48 (suppl IV): IV-7, 1973 25. SLOME R: Withdrawal of propranolol and myocardial infarction. Lancet 1: 156, 1973 26. NELLEN M: Withdrawal of propranolol and myocardial infarction. Lancet 1: 558, 1973 27. DIAZ RG, SONBERC JC, GREEMAN E, LEVITT B: Withdrawal of propranolol and myocardial infarction. Lancet 1: 1068, 1973 28. THOMPSON FD, JOEKES AM, FOULKES DM: Pharmacodynamics of propranolol in renal failure. Br Med J 2: 434, 1972 29. LOWENTHAL DT, BRIGGS WA, GIBSON TP, MATRESIK G, DEMAREEE G: Propranolol half-life in chronic renal disease. Pharmacologist 15: 188, 1973 30. BRICK I, HUTCHINSON KJ, MCDEVITT DG: Comparison of the effects of ICI 50172 and propranolol on the cardiovascular responses to adrenaline, isoprenaline and exercise. Br J Pharmacol 34: 127, 1968 31. CLEAVELAND CR, SHAND DG: Effect of route of administration the relationship between beta-adrenergic blockade and plasma propranolol level. Clin Pharmacol Ther 13: 181, 1972 CLEAVELAND CR, RANGNO RE, SHAND DG: A standardized isoproterenol sensitivity test. The effects of sinus arrhythmia, atropine and propranolol. Archives Intern Med 130: 47, 1972 GEORGE CF, FENYVESI T, DOLLERY CT: Pharmacological effects of propranolol in relation to plasma levels. In Biological effects of drugs in relation to their plasma concentrations, edited by DAVIES DS, PRICHARD BNC. University Park, Maryland, University Park Press, 1973, pp 123-133 FITZGERALD JD, O'DONNELL SR: Pharmacology of 4hydroxypropranolol, a metabolite of propranolol. Br J Pharmacol 43:222, 1971 GEORGE CF, DOLLERY CT: Plasma concentrations and pharmacological effect of beta-receptor blocking drugs. In Proc 5th Congr Pharmacology, Vol 3. Basel, Karger, 1973, on 32. 33. 34. 35. pp 86-97 36. COLTART DJ, MELDRUM S: The effect of racemic propranolol, dextro-propranolol and racemic practolol on the human and canine cardiac transmembrane action potential. Arch Intern Pharmacodyn 192: 188, 1971 37. COLTART DJ, GIBSON DG, SHAND DG: Plasma propranolol levels associated with suppression of ventricular ectopic beats. Br Med J 1: 490, 1971 38. LINKo E, RUSOTEENOJA R, SIITONEN L: A clinical study on the mechanism of the antiarrhythmic action of a new antagonist to beta-adrenergic receptor. Am Heart J 75: 138, 1968 39. PRAKASH R, PARMLEY WW, ALLEN HN, MATLOFF JM: Effect of sotalol on clinical arrhythmias. Am J Cardiol 29: 397, 1972 40. HOWITT G, HUSAINII M, ROWLAND DJ, LOGAN WFWE, SHANKS RG, EVANS MG: The effect of the dextro isomer of propranolol on sinus rate and cardiac arrhythmias. Am Heart J 76: 736, 1968 41. WILSON AG, BROOKE OG, LLOYD HJ, ROBINSON BF: Mechanism of action of beta-adrenergic receptor blocking agents in angina pectoris; comparison of action of propranolol with dexpropranolol and practolol. Br Med J 4: 399, 1969 42. WAAL-MANNING HJ: Comparative studies on the hypotensive effects of beta-adrenergic receptor blockade. N Z Med J 71: 383, 1970 43. HORN ME, PRICHARD BNC: A variable dose comparative trial of propranolol and sotalol in angina pectoris. Br Heart J 35: 555, 1973 44. SOWTON E, SMITHEN C, LEAVER D, BARR I: Effect of practolol on exercise tolerance in patients with angina pectoris. Am J Med 41: 63, 1971 45. PRICHARD BNC, BOAKES AJ, DAY G: Practolol in the treatment of hypertension. Postgrad Med J (suppl) 47: 84, 1971 46. GIBSON D, SOWTON E: The use of beta-adrenergic blocking drugs in dysrhythmias. Prog Cardiovasc Dis 12: 16, 1969 47. BUHLER FR, LARAGH JH, BAER L, VAUGHAN ED, BRUNNER HR: Propranolol inhibition of renin secretion. N Engl J Med 287: 1209, 1972 48. BUHLER FR, LARACH JH, VAUGHAN ED, BRUNNER HR, GAVRAS H, BAER L: Antihypertensive action of propranolol. Am J Cardiol 32: 511, 1973 49. MICHELAKIS AM, McALLISTER RG: The effect of chronic adrenergic receptor blockade on plasma renin activity in man. J Clin Endocrinol Metab 34: 386, 1972 50. STOKES GS, WEBER MA, THORNELL IR: Beta-blockers and plasma renin activity in hypertension. Br Med J 1: 60, 1974 51. PRICHARD BNC, GILLAM PMS: The use of propranolol in the treatment of hypertension. Br Med J 2: 725, 1964 52. PRICHARD BNC, GILLAM PMS: Treatment of hypertension with propranolol. Br Med J 1: 7, 1969 53. ZACHARIAS FJ, COWEN KJ, PRESTT J, VICKERS J, WALL BG: Propranolol in hypertension. A study of long-term therapy, 1964-1970. Am Heart J 83: 755, 1972 54. STERN S, HOFFMAN M, BRAUN K: Cardiovascular responses to carotid and vertebral artery infusions of propranolol. Cardiovasc Res 5: 424, 1971 55. MYERS MG, LEWIS PG, REID JL, DOLLERY CT: Cardiovascular effects of centrally administered d-1 and dl-propranolol in the conscious rabbit. Eur J Clin Invest 3: 257, 1973 56. ZACEST R, GILMORE E, KOCH-WESER J: Treatment of essential hypertension with combined vasodilation and betaadrenergic blockade. N Engl J Med 286: 618, 1972 57. HOLLANDER W: Hypertension, antihypertensive drugs and atherosclerosis. Circulation 48: 1112, 1973 58. PRICHARD BNC, GILLAM PMS: An assessment of propranolol in angina pectoris. A clinical dose response curve and the effect on the electrocardiogram at rest and on exercise. Br Heat J 33: 473, 1971 59. MCLEAN CE, DEANE BC: Propranolol dose determinants including blood level studies. Angiology 21: 536, 1970 60. GRANT RHE, KEELAN P, KERRNOHAN RG, LEONARD JC, NANCEKIEVILL L, SINCLAIR K: Multicenter trial of propranolol in angina pectoris. Am J Cardiol 18: 361, 1966 61. SHAND DG, SELL CG, OATES JA: Hypertrophic obstructive cardiomyopathy in an infant propranolol therapy for three years. N Engl J Med 285: 843, 1971 62. HUBNER PJB, ZIADY GM, LANE GK, HARDARSON T, SCALES B, OAKLEY CM, GOODWIN JF: Double-blind trial of propranolol and practolol in hypertrophic cardiomyopathy. Br Heart 35: 1116, 1973 - Circulation, Volume 52, July 1975 CLINICAL PHARMACOLOGY OF PROPRANOLOL 63. GREENBLATT DJ, KOCH-WESER J: Adverse reactions to propranolol in hospitalized medical patients. Am Heart J 86: 478, 1973 64. GREENBLATT DJ, KOCH-WESER J: Adverse reactions to betaadrenergic receptor blocking drugs: A report from the Boston collaborative drug surveillance program. Drugs 7: 118, 1974 65. MAROKO PR, BRAUNWALD E: Modification of myocardial Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 Circulation, Volume 52, July 1975 15 infarction size after coronary occlusion. Ann Intern Med 79: 720, 1973 66. GIBSON DG: Pharmacodynamic properties of beta-adrenergic blocking drugs in man. Drugs 7: 8, 1974 67. BRUNINER HR, LARAGH JH, BAER L, NEWTO.N MA, GOODWIN FT, KRAKOFF LR, BARD RH, BUHLER FR: Essential hypertension: renin and aldosterone, heart attack and stroke. N Engl J Med 286: 441, 1972 Clinical pharmacology of propranolol. A S Nies and D G Shand Circulation. 1975;52:6-15 doi: 10.1161/01.CIR.52.1.6 Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1975 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7322. Online ISSN: 1524-4539 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circ.ahajournals.org/content/52/1/6.citation Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation is online at: http://circ.ahajournals.org//subscriptions/