Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Marine microorganism wikipedia , lookup
Bacterial cell structure wikipedia , lookup
Neglected tropical diseases wikipedia , lookup
Germ theory of disease wikipedia , lookup
Triclocarban wikipedia , lookup
Gastroenteritis wikipedia , lookup
Sociality and disease transmission wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
Marburg virus disease wikipedia , lookup
Transmission (medicine) wikipedia , lookup
Bacterial morphological plasticity wikipedia , lookup
Infection control wikipedia , lookup
Globalization and disease wikipedia , lookup
Clostridium difficile infection wikipedia , lookup
Bioterrorism wikipedia , lookup
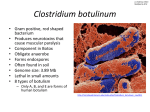
Botulism By Cicely Quade Name and history: Botulism; Scientific name: Clostridium botulinum, it is a bacterium that is part of the Clostridium family and it is an endospore- it forms gram-positive bacilli8. There are several common names for botulism including botulinum toxin as well as Botox8. There are seven types of botulism bacteria that have been discovered and the have been identified with the letters A-G but only the strains A, B, E and F can manifest themselves in humans as an illness8. The taxonomy of the C. botulinum in the order of domain, kingdom, phylum, class, order, family, genus and species is as follows: Bacteria, Bacteria, Firmicutes, Clostridia, Clostridiales, Clostridiaceae, Clostridium and Clostridium botulinum14 The bacterium is rod shaped and they grow best in environments that are low in oxygen1. John Muller, who thought that the onset of symptoms was linked to eating sausage, first discovered this disease in 1870. Thus, the name of botulism was derived from the Latin word for sausage2. Transmission: Botulism is unique from other infectious diseases in that it is not transmitted directly from human to human1. There are two main types of botulism: wound botulism and foodborne botulism1. Wound botulism occurs when a person ingests food that has been infected by the bacterium’s spores that can grow into bacteria in the intestines of both adults and infants1. The bacteria release toxins in the intestines that affect the nerves of the host1. Wound botulism occurs when a wound becomes infected with the Clostridium botulinum bacterium and it produces toxins within the wound that travel through the body to the nerves of the host1. Reservoir: Clostridium botulinum can be found within soil1. Most cases of foodborne botulism transmission occur when home-processed foods are not processed correctly and they do not have very much acid in their preservation solutions that allow the bacteria to become active3. Botulism toxins in canned foods are more frequently present in the toxins that are not very acidic3. When the human digests the food it can become infected with spores of the bacteria. Wound botulism occurs most frequently from illegal drug use, especially black tar heroin from Mexico that can contain the Clostridium botulinum spores7. When the heroin is injected into the body the spores are absorbed into the blood stream and circulated around the body7. The bacteria is extremely heat resistant8. General Characteristics: Laboratory: It is often difficult to confirm the presence of botulism when trying to diagnose a patient, but routine tests are often helpful for ruling out other diseases for the diagnosis5. Boutlism is positively identified by finding botulinum neurotoxin in the serum of feces, vomit, or in a sample of the contents of the gastrointenstinal fluids or if a sample of the food that was ingested if it is available5. They perform either mouse toxicity or a neutralization bioassay.5 In the mouse toxicity test, a mouse is injected with the serum of the patient and observed for signs of botulism5. If that is not conclusive then the serum from the patient is added to six test tubes and then antibotulinum toxin (one for A, B, E and F and a combination of all four) are added to each test tube and then injected into the mouse and the mouse is observed for signs of botulism5. Clinical: The physician obtains a log of all the food ingested by the patient for the past five days1. The physician tests the individuals’ muscle and neurological responses and looks for signs of muscle paralysis1. Signs and Symptoms: In foodborne botulism the onset of symptoms is usually eighteen- thirty-six hours after ingesting the infected food1. But, signs have been known to occur as early as six hours and as delayed as ten days1. There are several symptoms of botulism that include double vision as well as blurry vision, droopy eyelids, muscle weakness, slurred speech, dry mouth as well as difficulty swallowing1. In infants the symptoms include difficulty eating, poor muscle tone as well as being constipated and having a weak cry1. All of these symptoms indicate that the bacterial toxin is causing muscle paralysis1. If botulism is diagnosed early on the patient can take a botulism antitoxin but if the symptoms are left untreated the toxin could spread to the respiratory muscles and the abdominal muscles as well as the muscles of the limbs1. Virulence Mechanisms: The Clostridium botulinum bacteria reproduce by spores that can remain dormant until it is in anaerobic conditions that are ideal for the bacteria to reproduce3. For foodborne botulism the food is ingested that has been contaminated with the toxin and it is absorbed through the gastrointestinal tract into the blood stream3. The toxin circulates through the body until it reaches a peripheral neuromuscular synapse and the toxin will bind to the presynaptic terminals and that blocks the release of the acetylcholine3. The release of acetylcholine is essential for the stimulation of muscle contractions3. Prevention: Botulism is most commonly transmitted through infected food and water13. To prevent botulism in infants (under twelve months of age) it is recommended to not allow them to eat honey12. In adults and children, a common source is home-canned foods that have a low acid content but can also be found in commercially canned foods if it is improperly done13. If canning foods at home it is important to follow proper canning methods13. If you are wounded, proper treatment of the wound by seeking medical attention or cleaning the wound can prevent wound botulism13. Control/Treatment: Botulism has a high mortality rate if it is not treated quickly after the onset of symptoms3. The antibotulinum toxin can be used to treat the patient but it will not be effective if the botulinum toxin has already reached the neuromuscular synapses3. If the toxin reaches the toxins then the individual still has a chance to recover but it is a very long and expensive process3. The body never naturally becomes immune to the toxin and a vaccine has not been developed due to the incredibly rare nature of the disease3. Infants can be protected from the disease by not exposing them to solid food before twenty weeks of age3. Adults can protect themselves from botulism by practicing safe canning practices and or eating canned food that has been processed as well as by not injecting black tar heroin into their blood stream5. A faster diagnosis test is currently being researched5. Current Information: United States: In the United States there are an average of 145 cases reported each year1. Approximately 15% of these are foodborne, and the majority is represented by infant botulism and approximately 20% of cases are wound botulism1. In 2015, there was an outbreak in Ohio that was the largest outbreak in recent history11. The outbreak originated from a church potluck where there were over 52 foods available11. The most likely source of the toxin was from a potato salad that was prepared using potatoes that had been canned at home11. The individual used a boiling water canner instead of a pressure canner, which kills the Clostridium botulinum bacteria11. For most of the individuals at the potluck their symptom onset was approximately 2 days after eating at the potluck11. There were approximately 29 individuals affected during the outbreak but there were no casualties11. Global information: Outbreaks of botulism are rare but the WHO considers infection a public emergency because it can be spread rapidly, especially if a large group of individuals are eating the same food8. There was a massive outbreak of botulism in Northern Thailand in 200610. The outbreak was due to contaminated home-canned bamboo shoots10. This outbreak affected 209 individuals and 134 of them were hospitalized10. The response was overwhelming to prevent the outbreak from spreading further out of the village and to prevent any deaths10. Also, Italy tends to have more outbreaks of botulism in general compared to other countries around the world9. Of the outbreaks recorded, 57% are the result of vegetable canning and about 15% are the result of contaminated ham or sausage9. The most recent outbreak was in 2011 in Finland but was the result of imported jars of olives that were canned in Italy; there were three cases detected and one death9. Work cited: 1. "Botulism."CentersforDiseaseControlandPrevention.CenterforDisease ControlandPrevention,25Apr.2014.Web.26Feb.2016. <http://www.cdc.gov/nczved/divisions/dfbmd/diseases/botulism/#diagno se>. 2. “Botulism."OntarioMinestryofHealthAndLongTermCare.N.p.,2013.Web. 25Feb.2016. <http://health.gov.on.ca/en/public/publications/disease/botulism.aspx>. 3. "Botulism."PathogenProfileDictionary.N.p.,n.d.Web.26Feb.2016. <http://ppdictionary.com/bacteria/gpbac/botulinum.htm>. 4. ClostridiumBotulism.ByAlbertJ.Nantel.Erfurt:INTOX12,2000.Print. 5. "LaboratoryConfirmationofBotulism."N.p.,n.d.Web.26Feb.2016. <https://saki.ohsu.edu/access/content/public/Botulism/Experts/Laborator y%20Confirmation%20of%20Botulism.pdf>. 6. Payne,Ed,andAshleyFantz."1DeadinBotulismOutbreakLinkedtoOhio ChurchPotluck."CNN.CableNewsNetwork,22Apr.2015.Web.26Feb. 2016.<http://www.cnn.com/2015/04/22/health/church-potluckbotulism/index.html>. 7. Schoenstadt,Arthur,MD."HowDoesBotulismTransmissionOccur?" EMEDTV.Clinaero,Inc.,13July2013.Web.26Feb.2016. <http://diseases.emedtv.com/botulism/botulism-transmission-p2.html>. 8. WorldHealthOrganization.ClostridiumBotulism.ByAlbertJ.Nantel.Erfurt: INTOX12,2000. http://www.who.int/csr/delibepidemics/clostridiumbotulism.pdf 9. BotulisminItaly.(2014,March30).RetrievedMay12,2016,from http://www.gideononline.com/tag/botulism/ 10. Ungchusak,K.,Chunsuttiwat,S.,Braden,C.,Aldis,W.,Ueno,K.,Olsen,S.,& Wiboolpolprasert,S.(2007,March).Theneedforglobalplannedmobilization ofessentialmedicine:LessonsfromamassiveThaibotulismoutbreak. RetrievedMay12,2016,from http://www.who.int/bulletin/volumes/85/3/06-039545/en/ 11. McCarty,C.,PhD,Angelo,K.,DO,Beer,K.D.,Cibulskas-White,K.,Quinn,K.,De Fijter,S.,...Walz,E.(2015,July31).NotesfromtheField:LargeOutbreakof BotulismAssociatedwithaChurchPotluckMeal—Ohio,2015.Retrieved May12,2016,from http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6429a6.htm 12. BotulismPrevention&Control.(2016,May3).RetrievedMay12,2016,from http://www.cdc.gov/botulism/prevention.html 13. Botulism.(n.d.).RetrievedMay12,2016,from http://www.foodsafety.gov/poisoning/causes/bacteriaviruses/botulism/ 14. Strandwitz,P.(2008,April17).Classification.RetrievedMay12,2016,from http://bioweb.uwlax.edu/bio203/s2008/strandwi_phil/schedule.htm