Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
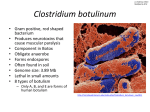
Botulism, Scotland 2015: are we recognising it? M. Day [1], M. G. Booth [1], G. Penrice [2], L. Donaldson [1] 1. Glasgow Royal Infirmary (GRI), Glasgow, UK 2. Public Health Unit, Gartnavel Royal Hospital , Glasgow, UK Botulism is a rare condition caused by the toxin produced by Clostridium botulinum, or germination of C. botulinum spores in wounds. Across Europe, most wound botulism is now associated with drug injection, especially muscle popping [1]. Between 21.12.14 and 20.02.15, there were 24 confirmed, or probable cases of botulism in people who inject drugs (PWIDs) in Scotland. All had recent history of heroin injection with accidental or intentional subcutaneous or intramuscular injection [2]. Epidemiology & Interventions Table 1- Demographic and clinical history of botulism cases, GRI n Sex Age 1 M 35 2 F 41 3 F 40 4 M 30 5 F 39 Clinical features/ skin abscesses Dyspnoea, ataxia, ptosis, dysarthria, dysphagia, hypoxic cardiac arrest Dysphagia, laryngeal flaccid paralysis, ptosis Dyspnoea, dysphagia, stridor, thigh abscess Diplopia, dysarthria, respiratory failure, thigh abscesses Dysarthria, dysphagia, respiratory failure, skin abscesses Mechanical Ventilation Yes Outcome Yes Alive Yes Alive Yes Alive Yes Alive Died As this is a rare condition, suspecting botulism is key to instituting timely treatment. Wound infection has an incubation period of 4-14 days. Symptoms are of progressive central weakness; blurred vision, ptosis, dysphagia, dysarthria and stridor1. Consequently, ICU referral often occurs late e.g. complete airway obstruction in one instance and respiratory arrest in another. Health Protection Scotland (HPS) and the Police are attempting to trace the source of the outbreak, assumed to be a contaminated batch of heroin. Public health measures have included interviewing patients and advising PWIDs to smoke, rather than inject, heroin. Discussion Meanwhile, Botulism should be part of the differential diagnosis in any PWID presenting with blurred vision, ptosis, dysphagia, dysarthria or other muscle weakness and should be referred for prompt Critical Care review. Biological samples should be taken prior to antitoxin and antibiotics administration. Public Health should also be informed of all suspected cases [3]. References 1. European Centre for Disease Prevention and Control. Annual Epidemiological Report 2014. Botulism Pages 10-14. http://www.ecdc.europa.eu/en/publications/Publications/foodwaterborne-diseases-annual-epidemiological-report-2014.pdf 2. Health Protection Scotland. HPS Weekly Report “Botulism alert for people who inject drugs- update. 20th January, 2015. Volume 49 No. 2015/03 ISSN 1753-4224 (Online) http://www.hps.scot.nhs.uk/documents/ewr/pdf2015/1503.pdf 3. Public Health England. Shooting Up: infections among people who inject drugs in the UK, 2014. https://www.gov.uk/government/uploads/system/uploads/attachment_ data/file/370707/Shooting_Up_2014.pdf