Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Cardiac contractility modulation wikipedia , lookup
Electrocardiography wikipedia , lookup
History of invasive and interventional cardiology wikipedia , lookup
Saturated fat and cardiovascular disease wikipedia , lookup
Jatene procedure wikipedia , lookup
Cardiovascular disease wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
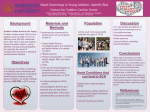
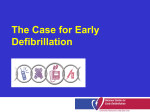
Cardiac surgery wikipedia , lookup
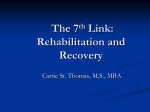
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
DOI: 10.1161/CIRCULATIONAHA.114.011988 Sudden Cardiac Arrest During Sports Activity in Middle Age Running title: Marijon et al.; Sudden Cardiac Arrest during Sports Eloi Marijon, MD, PhD1,2,3; Audrey Uy-Evanado, MD1; Kyndaron Reinier, MPH, PhD1; Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 Carmen Teodorescu, MD, PhD1; Kumar Narayanan, MD1; Xavier Jouven, MD, PhD2,3; MD D1 Karen Gunson, MD4; Jonathan Jui, MD, MPH5; Sumeet S. Chugh, M 1 The Heart Institute, Cedars-Sinai Medical Ce C Center, nter, Los Angeles, C CA; A; 2Cardiology Dept, European Euro Eu ro opean G Georges e rg eo ges Pompidou Pom mpi pido d u Ho do Hosp Hospital, spit sp ital al,, Paris, Pari Pa ris, s,, F France; raance; 3 Pa Paris Pari riss Descartes ri Deesc scar arte tess University, U iv Un iver errsi sity ty,, Pa ty Pari Paris, riis, s F France; ranc ra n e 4 Dept D ept p of Pathology, Paath tholloggy, O Oregon regoon Heal H Health ea th h aand ndd Sci Science ien nce U University, nive ni vers ve rsit rs ity, it y, Po Portland, ortlland,, O OR; R;; 5De Dept D pt off E Emergency mergeency Medicine, Medi Me dicinee, Or Oreg Oregon egon on Healt Health lthh an andd Sc Scienc Science ncee Un Univ University, iver ersity ty, Po Port Portland, r laand nd, OR Address for Correspondence: Sumeet S. Chugh MD Cedars-Sinai Medical Center Advanced Health Sciences Pavilion Suite A3100, 127 S. San Vicente Blvd. Los Angeles, CA 90048 Tel: 310-423-1206 Fax: 310-423-3522 E-mail [email protected] Journal Subject Code: Atherosclerosis:[135] Risk factors 1 DOI: 10.1161/CIRCULATIONAHA.114.011988 Abstract Background—Sports-associated sudden cardiac arrests (SCAs) occur mostly during middle age. We sought to determine burden, characteristics, and outcomes of SCA during sports among middle aged residents of a large US community. Methods and Results—SCA cases aged 35-65 years were identified in a large, prospective, population-based study (2002-2013), with systematic and comprehensive assessment of their lifetime medical history. Of the 1,247 SCA cases, 63 (5%) occurred during sports activities at a Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 mean age of 51.1±8.8 years, yielding an incidence of 21.7 (95%CI 8.1–35.4) per million per among men year. The incidence varied significantly based on sex, with a higher incidence am mong n m en ((RR RR RR 18.68 95%CI 2.50–139.56) for sports SCA, as compared to all other SCA (RR 2.58, 95%CI 2.12–3.13). event 2. .122–3 –3.1 .13) 13) 3).. Sports S orrts SCA Sp SCA was also more likely to o bbee a witnessed eve v nt ((87 ve 87 vs. 53%, P<0.001), with w ith h cardiopulmonary cardiopul ulm monary nary y resuscitation reesus esusccit citati tatioon on (44 (44 vs. vs. 25%, 25%, P=0.001) P=0.00 P= 001) 00 1) and annd nd ventricular venntr tric i ul ic ulaar fibrillation fibr fi bril illa laati tion o (84 on (844 vvs. s. 51%, P<0.0001). 51 1%, P <0.0 <0 .0000 001) 1)). Survival Surv Surv viv val too hospital hoosp spit itaal it al discharge dissch chaarge ge was was hhigher igh her for or sports-associated spo port rtsrt s-aasssoci sociiat ated e SCA ed SCA (23.2 (23.2 vs. vss. P=0.04). Sports with cardiac 11 13.6%, P=0.0 04) 4).. Sp Spor o ts or t SCA CA ccases ases as e ppresented es rese re sent se nted nt ed w itth kknown n wn ppre-existing no re-e re -eexi x sttin ingg ca card rdia rd i c disease ia dise di seas se asee in 16%, as cardiovascular risk factor in 56%, and overall, 36% of cases had typical cardiovascular symptoms during the week preceding SCA. Conclusions—Sports-associated SCA in middle age represents a relatively small proportion of the overall SCA burden, reinforcing the idea of the high benefit-low risk nature of sports activity. Especially in light of current population aging trends, our findings emphasize that targeted education could maximize both safety and acceptance of sports activity in the older athlete. Key words: coronary artery disease, physical exercise, cardiopulmonary resuscitation, cardiac arrest 2 DOI: 10.1161/CIRCULATIONAHA.114.011988 Introduction Sudden Cardiac Arrest (SCA) represents a major public health issue worldwide, accounting for almost half of cardiovascular mortality.1, 2 When occurring in the setting of sports, SCA generates major societal attention and alarm, since the collapse usually occurs in a public setting, in front of many witnesses, striking those considered to be the healthiest in the community. SCA among young competitive athletes has been extensively investigated in the United States,3, 4 allowing significant improvements in the field, notably initiation and optimization of preventive strategies.5-9 However, except for limited data on specific recreational sport Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 activities,10, 11 there are, to the best of our knowledge, no studies evaluating SCA during sports among middle-aged subjects in any United States community. Recent Europeann experience expe p ri rien ence en ce has has a emphasized that, in the community, the largest burden of sports-associated SCA results from ev events ven ents ts aamong mong mo ng m middle-aged iddl id d e-aged participants.12-15 A bbetter dl et er understandin ette understanding in ng off bburden ur urden (absolute as well as relative relative to oother therr nnon-sports th onn-sspoort rtss re rela related laate tedd SC SCAs)) aand nd ccharacteristics haraactter eriistics off SC SCA CA du duri during rinng ri ng ssports port po r s in m rt middleidddleid dl aged ppopulation aged opul op ullat atiion ion is llikely ikeelyy to iinform ik nfo orm ppreventive reeve vent ntiv nt ivee st iv sstrategies. raateegi gies es.. Avail Available lab able l information le inf nfor orrma m tiion hhas as ttraditionally radi ra diiti tion onal on ally al ly y been bee eenn restricted r sttri re r ct cted e tto ed o re resu resuscitation susc su scit sc itat it atio at ionn va io vari variables riab ri able ab l s in the le immediate setting of the event. However, for a study to be meaningful from a clinical perspective a detailed evaluation of the lifetime past medical history is needed, which is particularly challenging to obtain for SCA where the majority will inevitably die in the field, and consequently the information collected by Emergency Medical Services (EMS) is often restricted to data regarding the resuscitation process. Details of the past medical history of SCA patients (especially those that cannot be resuscitated) are thus usually sparse and very rarely considered systematically. In this regard, information concerning prior cardiovascular risk factors, frequency and type of symptoms in the weeks preceding SCA during sports, have not been previously 3 DOI: 10.1161/CIRCULATIONAHA.114.011988 characterized. Using a large 12-year prospective study of SCA in a northwestern US metro region, with a systematic comprehensive evaluation of the lifetime clinical history, we assessed the characteristics and outcomes of SCA during sports in middle age compared to other SCAs (not occurring during sports activity). Methods Setting, Definitions and Survey Methods Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 The Oregon Sudden Unexpected Death Study (Oregon-SUDS) is an ongoing community based 166 prospective study of out-of-hospital SCA. Detailed methods have been published ed d previously. pre r vi viou ousl usl sly. y 16,17 y. Briefly, since February 1, 2002, cases of SCA in the Portland Oregon metropolitan area were identified den nti tifi fied fi ed using usi sinng multiple multiple ul sources that included th the he E Emergency mergency Me Medical edi d caal Services Se (EMS) response, response the he Medical Medical Examiner’s Exaamin Ex iner err’ss office off ffic icce and and emergency emer em errgenncyy departments depa partme pa ment me ntss of of all all ll of of th the he 16 llocal occal hhospitals. osspiitals ls. Th ls T Thee county emergency medical response with advanced co ounty unty hhas as a two-tiered twoo-ttie iere reed em emer rge g nc ncyy me ediica call re esp spoonsse se ssystem ysste tem m wi w th iinvolvement th n olvveme nv ment nt ooff ad adva ancced cardiac life support sup uppo port po rt staffed staaff ffed d fire fir ire engine engi en giine n companies com omppan anie i s as well ie wel elll as a transporting tra rans nspo ns po ort rtin ingg ambulances. in ambu am bu ulaanc nces es. es A comprehensive evaluation is performed for each case of unexpected death, including analysis of the circumstances of arrest recorded by EMS personnel or the medical examiner, prearrest medical records, and available autopsy data. A process of in-house adjudication by three physicians is employed to determine cases meeting criteria for SCA. In the event of a disagreement regarding a specific case, the determination is based on the majority opinion. In the present analysis we included middle-aged men and women, defined as male subjects aged 35–65 years, ascertained from February 2002 to January 2013. This study was approved by the Institutional Review Boards of Cedars-Sinai Medical Center, Oregon Health and Science 4 DOI: 10.1161/CIRCULATIONAHA.114.011988 University and all participating hospitals. Sudden cardiac arrest was defined as a sudden unexpected pulseless condition; if unwitnessed, subjects were included if observed alive and symptom-free within 24 hours of their sudden arrest. During the adjudication process, patients with known non-cardiac causes of arrest (e.g., trauma, overdose, pulmonary embolism, cerebrovascular accident, and terminal illness such as cancer not in remission) were excluded.1, 15 SCA during sports was defined as death occurring during sports activities or within one hour of cessation of sports activity. In most cases, the event occurred as an unexpected collapse during physical exertion. Of note, SCA occurring Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 during physical activity but not in the setting of sports (typically SCA during sexual intercourse) was not considered as sports-associated SCA. Previous medical history was obtained obtai aiineed from from a comprehensive assessment of inpatient as well outpatient medical records/visits obtained from he hospital hosspit ho spit ital al systems syyste teems ms in the Portland metropolita an area. arrea. the metropolitan V arriables ri Asse sessseed ed Variables Assessed Va ari r ab able less considered connsid co nsid derred in in the the pr pres essen entt an anal a ys al ysis is inc ncllude nc uded ed demographics, dem emoogra ogra raph phhiccs, circumstances circcums msta taanc nces es off occurrence occcu curr rreence Variables present analysis included as well as res sus u ci c ta tati tion ti on n ddata. atta. a IIn n ad addi diiti t on n tto o ddetailed etai et a leed in ai info orm rmat atio at ionn ob io oobtained tain ta ined in ed ffrom rom ro m EM EMS, S, iindex ndex resuscitation addition information hospital stay, and medical examiner medical records, a working group of the Oregon-SUDS collected and assessed the lifetime past medical history for both deceased patients and consent survivors, including assessment of symptoms prior to SCA. Variables included: (i) time and location of each event; (ii) clinical and demographic information (age, sex, personal history of known cardiovascular risk factors or heart disease, and any symptoms during the preceding week). Symptom assessment was derived from multiple sources, including family members at the scene of SCA, witnesses, and survivors of SCA. In addition, available hospital and outpatient medical records for all subjects were systematically 5 DOI: 10.1161/CIRCULATIONAHA.114.011988 analyzed for information regarding symptoms. Symptoms were categorized as absent, present or not evaluable based on the extent of information available, and the agreement of investigators. Coronary Artery Disease (CAD) was defined as 50% lumen stenosis on coronary angiogram prior to SCA event or identified at autopsy. In addition, subjects with past history of myocardial infarction or coronary revascularization (either surgical or percutaneous coronary intervention) were categorized as patients with CAD. History of heart failure was defined by a physician based on medical records (in-hospital and/or outpatient visit) and/or low left ventricular ejection fraction from echocardiogram, angiogram, or radionuclide multi-gated acquisition prior and Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 unrelated to cardiac arrest; (iii) data regarding the setting and nature of sports activity at the time of the event; (iv) circumstances of collapse (during sports activity or immediately ly y aafter), f er), llocation ft ocat oc a ion at type ype (sports facility or other area), presence of witnesses; (v) detailed information regarding resuscitation EMS their arrival esuusc scit itat atio tio ionn in iincluding cllud udin i g response time (time from m EM MS call to thei eirr arri riiva vall on the scene), bystander resuscitation initiation, bysttan a der cardiopulmonary card dio opu ulm mon nar aryy re res susccittatiion (CPR) susc (C CPR R) in nitiati tiion, on, the t e presenting th prressen nting tiing ccardiac arddiac ar diac rrhythm hyth hy thm th m (ventricular pulseless return ven entr tric tr icul ic ular ar ttachycardia/fibrillation, achhyc ac hycard card dia ia/f / ib /f ibri riilla lati tion ti on, pu on ulssel eles ess el es eelectrical ecctrric i al aactivity ctiivit ct ivit ityy or o aasystole), sysstoole) sy ole)), re etu turn rn ooff spontaneous circulation (defined palpable conjunction pontaneous ci circ rcul rc ulat ul atio at io on (d (def efin ef ined in ed d aass re rreturn tu urn n ooff a pa palp lp pab ablee ppulse ulse ul se iin n co onj njun unct un ctio ct ionn wi io with th a ssystolic y tolic ys blood pressure of >60 mmHg); (vi) survival status to hospital discharge, available in the majority of admitted cases (96%) — For survivors, neurologic status at discharge was evaluated using the Cerebral Performance Categories (CPC) score from medical records, and a comparative analysis was performed between sports-associated SCA and other SCA;14 (vii) autopsy report if available. Statistical Analysis This report was prepared in compliance with the STROBE checklist for observational studies.18 The objective of the study was to provide comprehensive comparisons between sports SCA and 6 DOI: 10.1161/CIRCULATIONAHA.114.011988 non-sports SCA, including subject characteristics and survival to hospital discharge as well as neurological outcomes. Case characteristics were reported as mean ± standard deviation, proportions, median and Interquartile Ranges (IQR), as appropriate. Comparisons between groups used Ȥ2 test for categorical variables, Fisher Exact test when appropriate and Student’s ttest or Mann-Whitney test for continuous variables. For calculation of incidence rates, the population was limited to Multnomah County, Oregon, the largest subset of the metro area residents (population 679,348, including 135,868 men and 133,598 women, aged 35 to 65 years, 2003 US Census Bureau data for the Multnomah Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 County) and for the 2002–2005 period (where all SCAs were recorded). All Multnomah County esidents, aged 35 to 65, were included for calculation of annual incidence rates iin n mi m ddle dd le-a le -age -a g d ge residents, middle-aged men and women (calculated per year per million residents). Pred Pr edic ed ictors ic rss ooff survival to hospital discharg rg ge w ere studied aamong m ng mo gS C cases with CA Predictors discharge were SCA esuusc s itation attempted atte at teempte tedd (N=936). (N=9 (N =936 =9 36). 36 ). Any Any ny variables variab ab blees inn univariate univa vari va riaate ate analyses anaalyyses an yses with withh a P value val a ue ue <0.15 <0..15 15 were wer ee resuscitation ncl clud uded ud e in ed in the the multivariate mult mu ltiv iv var aria iate t modeling. mod odel elin el ing. in g. The The association asssoc o iattionn of SCA SCA A with witth favorable faavo vora rabble ble ou out tcome tco ome (sur ((survival survvivval va included outcome o hospital discharge) disc di scha sc h rg ha rge) e was e) was a thereafter the here reeaft f err adj djus dj uste us teed fo or th hes e e id iden enti en tifi ti fied fi ed con onfo on foun fo undi un ding di ngg ffactors acto ac to ors in a singlee to adjusted for these identified confounding multivariable logistic regression analysis, allowing estimation of odds ratios (ORs) and their 95% confidence intervals (CIs). As a sensitivity analysis, to better appreciate the likelihood for survival when SCA occurs in the setting of sports activities, we performed additional analysis using propensity score matching.19 We calculated each subject’s propensity score as the predicted probability of having SCA during sports given the subject’s measured covariates (age, gender, history of coronary artery disease, presence of witness, bystander cardiopulmonary resuscitation, ventricular fibrillation, delay of intervention). We matched each case to the control subject (i.e., a patient who suffered a non-sports SCA) with the closest propensity score, which 7 DOI: 10.1161/CIRCULATIONAHA.114.011988 resulted in a dataset with 66 (33/33) SCA matched cases. All data were analyzed using STATA software version v11.0 (Lakeway Drive, TX). Results Patient Characteristics and Circumstances of SCA Occurrence Between February 2002 and January 2013, there were a total of 63 subjects, middle-aged SCA cases that occurred during sports activities (Table 1), mainly during jogging (27%), basketball (17%) and cycling (14%) activities. Other sports activities included gym activities (11%), golfing Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 (8%), volleyball (3%), tennis (3%), soccer (3%), and others (14%). Sports-associated SCA occurred during the actual sports activity in 45 cases (76%) and within the following follow wing ng hour hou ourr in 14 14 (24%). 24%). More than half of the cases (58%) occurred in sports facilities such as a gym or a stadium, whereas tad diu ium m, w m, herreas he ass tthe he remainder (42%) occurredd in i the the field (outside (outsi siide d ooff ssports ports facilities). Among the sports-associated SCAs, which occurred outside occurred he 228 8 sports-as asssocciat ated e S ed CAss, CA s, w h ch hi c oc ccurrre red ou utsidee of of ssports poort rtss ffacilities, aci cili liti li t es, 118 8 oc occu curr cu rrred inn public pu ubllic parks, areas. pa park rks, rk s jjogging s, oggi og ging gi ng ttrails raills or oother therr ddelineated th elin el inea in eate ea tedd ar area eas. ea Of the he overall ove vera rall ra l number ll num u be berr off middle-aged mid ddllee ag aged ed SCA SCA cases cas a es in in this this region reg gio ionn during durrin du ingg the th he 10-year 10-y 10 -year periodd (N=1,247), sports-associated SCA in middle age represented 5% of SCA cases in this age group, yielding an overall incidence of 21.7 (95%CI 8.1–35.4) per million per year compared to 555.0 (95%CI 541.4–568.7) for non-sports-associated SCA. The incidence varied significantly according to sex with a much higher incidence among men (vs. women) for sports-associated SCA (RR 18.68 95%CI 2.50-139.56), as opposed to all other SCA where differences were smaller (RR 2.58, 95%CI 2.12-3.13). Extrapolating to the overall population of the United States, we estimated the total number of sports-associated SCA among the 35-65 year-old agegroup to be 2,269 (95%CI 772–3,773) events among men and 136 (95%CI 0–1,846) events 8 DOI: 10.1161/CIRCULATIONAHA.114.011988 among women per year. The mean age of patients developing SCA during sports was 51.1±8.8 years, without significant difference between men and women (51.1±9.1 vs. 50.3±4.6 years, P=0.86). Although there was an apparent similar overall prevalence of cardiovascular risk factors (1 cardiovascular risk factors, 56.3 vs. 62.7%, P=0.40), sports SCA cases were less likely to present with smoking (31.3 vs. 60.8%, P=0.001) and diabetes mellitus (8.3 vs. 28.4%, P=0.002). Sports SCA cases were also less likely to have known heart disease compared to non-sports SCA (15.9 vs. 30.2%, P=0.013) (Table 1). Among the 44 middle-aged participants with possible assessment of Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 symptoms during the week before the event, 14 (33%) presented with symptoms: typical chest were pain in nine, dyspnea in four, and typical influenza-like symptoms in one. Whilee tthere heeree w eree er significant ignificant sex differences in incidence of sports-associated SCA with higher burden in men, no significant men clinical ign nif ific ican ic an nt differences differren dif encces were identified between m enn and women fo for cl clin iniical in ic characteristics, circumstances and outcomes. ci irccum u stancess an nd ou out tcom omes es. es Bystander CPR, By yst s an ande derr CP de C R, Advanced R, Advvan nce ced d Life-Support Liife fe-S -Sup -S up ppo port rt and and Predictors Preediicttor orss of Survival Surrvi viva vaal data resuscitation survival SCA, association Descriptive da ata oon n re resu susccit su itat atio at ionn an andd su urv viv ival al aafter fte terr SC S A, bbased ased as ed oon n th thee as asso soci so c at ci atio io on wi with t sports, are presented in Table 2. When compared to other SCAs, SCAs during sports were characterized by a greater proportion of witnessed events (87 vs. 52%, P<0.001), bystander CPR (44 vs. 25%, P=0.001), as well as a greater likelihood of presenting with a shockable rhythm (84 vs. 51%, P<0.001). The mean response time (6.8±4 min) was very similar between both groups (P=0.99), with the proportion of patients receiving intervention within 8 min being 77% and 79% in sports SCA and non-sport SCA, respectively (P=0.44). Survival to hospital discharge was higher for sports-associated SCA (23.2%, 95%CI 11.8–34.6) compared to SCA not associated with sports (13.6%, 95%CI 11.6–15.5) (P=0.04) (Figure 1-Panel A). 9 DOI: 10.1161/CIRCULATIONAHA.114.011988 Among overall SCAs with resuscitation attempted, variables independently (multivariate analysis) associated with survival included public location (OR 1.55, 95%CI 1.10–2.17, P=0.011), presence of witness (OR 3.22, 95%CI 1.80–5.77, P<0.0001), and initial shockable rhythm (OR 4.54, 95%CI 2.94–7.14, P<0.0001). SCA in the setting of sports activity was not associated with higher survival after adjustment for resuscitation variables (OR 0.82, 95% CI 0.36–1.82, P=0.62) (Figure 1-Panel B). From the additional sensitivity analysis, the propensityscore matched odds ratio for survival was not significantly associated with sports-SCA: OR 0.84 (95% CI 0.19–3.80, P=0.82). In addition, no significant association was observed for age (50 Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 vs. >50 years) (OR 1.13, 95%CI 0.74–1.74, P=0.55) and delay in EMS response (<8min vs. 8min) (OR 0.96, 95%CI 0.69–1.34, P=0.83). Etiologies of SCA could be identified in 829 cases (66%), without significant difference between be etw wee eenn the the ssports-associated por orrts ts-a -associated and non sports-associated sports-ass sssoc o iated SCA (688 vs. v . 66%, vs 66% 66 %, respectively, P=0.76). P=0.76) The patterns sports are relatively T hee ov ooverall erall pa att tteernns ooff caus ccauses ausses es ooff SC SCA A aamong monng spo orts and nd nnon-sports on-s on -spo poorts SC SCA A ar re re rela lati t ve ti vely ly ssimilar imil im ilar il arr (Figure with coronary disease: among Figu Fi gure gu r 22), re ), w ithh a pr it ppredominance edomin ominan a ce ooff co an oro ona narry ry aartery r ery rt ery di isea isea ease se: am se amo ong th ong thee 8829 299 ccases, asess, 336 ases 6 oout utt ooff 433 (84%) sports-associated SCA CAD, compared out 84%) sports s-aass s oc ocia iate ia teed SC CA we were r aassociated re ssoc ss o ia oc iate tedd wi te with th C AD D, co comp mpar mp a ed ar d tto o 71 7177 ou ut of 7786 8 (91%) forr 86 other SCAs. The phenotype of coronary artery disease among SCA cases, based on the setting of occurrence (sports vs. non-sports) is reported in Table 3, for overall 181 (24%) of cases with typical features of acute coronary syndrome (either on cardiac pathology or coronary angiogram). Among those subjects with known coronary artery disease (517 subjects), 140 (27%) had undergone a revascularization procedure (percutaneous coronary intervention in 46%) prior to developing SCA. Other causes of SCA included dilated cardiomyopathy (30), hypertrophic cardiomyopathy (30), congenital heart disease (6), mitral valve prolapse (3), myocarditis (3), and arrhythmogenic right ventricular dysplasia (2) (Figure 2). 10 DOI: 10.1161/CIRCULATIONAHA.114.011988 Discussion To the best of our knowledge, this study represents the first comprehensive assessment of SCA associated with sports activity among middle-aged participants in a US community. First, our findings emphasize that sports-associated SCA eventually represented a relatively small proportion of overall SCA in this population; a fact that is likely to encourage sports activities among middle-aged athletes, after appropriate attention to any existing musculo-skeletal limitations. Second, the comprehensive assessment of the lifetime past medical history revealed that in almost two third of cases, patients present with either a previously documented significant Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 cardiovascular disease and/or symptoms prior to the event. This latter finding suggests that utilization of educational and general awareness approaches may further decrease see ssportsp rt po rtssassociated SCA burden. An objective obj b eccti tivve ve assessment of sports-associated sports-associiate ated SCA in the community c mm co mun unity outlines the scope of o problem difficult a pr roblem that at ccan an bbee di diff ffic ff icul ic ultt to aassess ul sssesss ddue uee to o a ddisproportionate isspro oport porttio iona natte eemotional moti mo t onall aand nd llay ay ppress ress iimpact. mpact mp The design our study, multiple especially Th he de desi sign gn ooff ou ur st stud uddy,, bbased ased as e oon ed n mu m ult lttip ple ssources ouurc r es off aascertainment, scer sc ertaain er inm ment ment nt,, was was es spe peci c al ci ally ly uuseful sefful ful to to captured. incidence SCA ensure that all all cases c se ca sess off interest int n er eres est were es wer e e ca apt p ur u ed ed.. Th Thee in nci c de denc ncee of ssports-associated nc poort rtss as sasso soci so c at ci ated ed S C estimated CA d in this study is highly similar to recently reported experiences among men in Europe (from 33 to 58 per million per year).12, 13 However, by evaluating sports-associated SCA as well as overall SCAs in the same time period and geographical area, we were able to place the burden of sportsassociated SCA in the context of overall SCA burden, and report that it eventually represented a small proportion of cases (one SCA out of 20). This finding suggests that in the context of SCA, the overall risk-benefit ratio is in favor of sports activity. In our population, the incidence ratio between men and women was 7-fold higher in sports SCA compared to non-sports SCA. Whether this reflects an intrinsic difference in 11 DOI: 10.1161/CIRCULATIONAHA.114.011988 pathophysiology between sexes is still speculative, but some factors merit consideration. First, men may have higher sports participation rates than women, which may contribute to the gender differences in SCA rates. Consistent with this observation, the incidence of SCA in women was transiently elevated during moderate to vigorous exertion but with a RR of only 2.38 (95% CI 1.23 to 4.60), while being almost 20-fold higher (RR 44.9, 95% CI 26.7 to 75.4) during vigorous activity among men enrolled in the Physicians’ Health Study.20, 21 Similar gender differences have also been reported in smaller retrospective studies in Finland and in the United States.22, 23 Second, the duration per sports session as well as the vigor and the method of physical activity Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 could differ between men and women. However, in considering inherent sex differences, potential explanations could include a number of factors, such as differences in vuln vvulnerable uln nerrab able le ubstrate (underlying structural or electrical heart disorder), triggers and/or autonomic substrate modu mo dula du lattors la tors rs.. T hee ag age e-specific prevalence of coro ona n ry heart disease see is kn kno ow to be lower in own modulators. The age-specific coronary known m idddle-aged dd wome wo menn (compared me ( om (c ompa pare pa redd too men), re men), and annd a particularly paartticuularly arly y lo ow pprevalence ow reva vale lennce ha le hass be een n aalso lo ls middle-aged women low been obbse serv rved rv e among ed amo m ngg female feema emale ale victims victtim vi imss of SCA, SCA A, suggesting sugg su gges gg e tiingg that es th hatt w om men m ay hhave av ve lo low wer ra wer rat tess off ssports ports por r ts observed women may lower rates yoca yo c rd ca rdia i l is ia sch hem emia ia aass th he pr prim imar im aryy ca ar caus use. us e 24 A e. Another noth no ther th er interesting intter e es esti t ng fa ti factor fact c or rrelates ct elat el a es to SCA with m myocardial ischemia the primary cause. coronary plaque rupture, which has been associated with a significant proportion of sportsrelated acute coronary syndrome and SCA.25 Overall, women are significantly more likely to have plaque erosions (as opposed to plaque rupture) than men, potentially suggesting an inherently lower likelihood of plaque rupture in the setting of exercise in women. Sex-related differences in ventricular repolarization and vagal tone are also potential factors affecting sports SCA pathophysiology.25 Subjects that suffer SCA during sports activity are generally perceived as previously healthy individuals with the event being considered as truly “unexpected’. Our comprehensive 12 DOI: 10.1161/CIRCULATIONAHA.114.011988 assessment of the past medical history in these cases demonstrates that in more than half, subjects had at least one cardiovascular risk factor. However, it is important to bear in mind that the long-term benefits of regular exercise on cardiovascular health are well established,21, 26 and habitual physical activity has been demonstrated to reduce coronary heart disease events. While existence of a “sports paradox” has been recognized— vigorous activity can also acutely and transiently increase the risk of SCA and acute myocardial infarction, especially in those not habituated to exercise — overall, the long-term benefits outweigh the short-term risks related to physical activity.21 Thus, the findings from this study should in no way discourage patients with Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 cardiovascular risk factors from engaging in regular, appropriate physical exercise within a framework of simple guiding rules from the treating physician. Whether a cautio cautionary onary nar nnote otee ne ot nee needs eds too be raised with respect to sports in those with established coronary artery disease, is a clinical question ques qu esti es tioon ti on tthat hatt need ha needs edss further investigation. Physic ed Physical cal al aactivity ctivity counse counseling eli l ngg m must ust be tailored to the nneeds eed ed ds and circ circumstances cum mstan anccess of tthe he iindividual, ndiv nd ivid iv dual, tthereby hereb by iincreasing ncr crreasi easiingg the the likelihood like keli l hoodd ooff su li success ucc cces e s an es andd 7-2 29 29 decreasing exercise. decr de crea cr easi ea s ng the si the h risk risk of cardiovascular cardi ard ovvasscu cullar ar events eve vent ntss during nt duuri r ng vvigorous ig gorrou ouss ex exe erciise erci se.227-29 In In this th his context, conte on extt, education off patients pat atie ieent ntss with wit recognized rec ecog og gni nize zeed cardiovascular card ca rdio rd io ova vasc s ul sc ulaar di dise seas se asee or rrisk as i k fa is fact ctor ct orss re or rega gard ga rdin rd ingg avoidance in disease factors regarding of extreme exercise may minimize any potential harm,23 while maximizing the acceptance of sports activity as a tool to improve cardiovascular fitness.21 Of interest, the proportion of patients with cardiovascular risk factors may appear higher when compared to the first published community-based report on SCA during sports in France (11%).12 Although differences in subjects’ characteristics may partly explain such differences, the lower rates in Europe may reflect the challenges in retrieving the detailed lifetime medical history in some studies. In addition, a significant proportion of the middle-aged subjects, who eventually died during sports activity, exhibited cardiac symptoms within a short period (one 13 DOI: 10.1161/CIRCULATIONAHA.114.011988 week) preceding the SCA event. Taken together, these findings suggest that careful attention to pre-existing heart disease and warning signs, along with public education and awareness in this regard may have an important place in the overall strategy to reduce SCA associated with sports activity. Overall, only one third of witnessed SCA cases received bystander CPR indicating substantial room for improvement in public knowledge and attitudes towards basic life support.30-33 Bystander-CPR is more likely to be initiated for SCA during sports, and this may have contributed to the higher likelihood of shockable rhythms at arrival of EMS, also extending Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 the window of opportunity for successful defibrillation.34, 35 The sports-associated SCA setting has appeal for the public and can serve as a springboard to efficiently educate the hee ppublic u li ub licc regarding egarding basic life support. Therefore, these findings also have potential implications for prehospital ho osp spit ital it al eemergency m rgen me ncy care policy-making to prom promote mote ote community ed education duc u at atiion in basic life support.36, 37 7 38, 39 A Although l hough SC lt SCA CA duri dduring uring ingg ssport port po rt iiss ass aassociated ssoc sociaated w with ith a hhigher igh her er ssurvival, urvivval,38 urvi itt seems seem se emss that em th hatt this thi h s is mainly ma ain inly ly explained exp xpla laiined la ined d by by the the co conc concomitant nccom mit itan antt asso an aassociation sso soci ciat ci atio ionn wi io with th h ffactors acto ac torss tthat to haat ha have vee a ppositive osit os ittiv i e im impact mpaactt oon n th the he resuscitation esuscitation n pr proc process, o es oc ess, s ssuch s, u h as pre uc presentation rese re s nt se n attio i n wi with th a sshockable hock ho ckab able ab le rrhythm hyth hy thm th m aand nd tthe he ppresence rese re senc se ncee of nc o witnesses during the SCA. Sports facilities have been identified as being particularly suitable for AED deployment,40 and where AED placement has largely been considered advisable.41 Our data further emphasize the need for systematic availability of AEDs in public sports facilities.42 However, since a good proportion of SCA occurred outside sports facilities, there is still room for improvement in public AED deployment. One potential strategy under consideration is AED placement in strategic locations such as public parks and popular jogging trails. Additionally public education to increase awareness also has an important role in improving bystander CPR. Although our data are, to the best of our knowledge, the first to address the issue related 14 DOI: 10.1161/CIRCULATIONAHA.114.011988 to burden and outcomes among the middle age from the general population in a large US community, with a particular efforts to provide data on past medical history, we acknowledge some limitations. Firstly, due to the extremely low incidence of SCA among women, statistical power to assess gender-related differences in sports SCA was limited. Second, we do not have access to information regarding whether or not cases of sports-associated SCA underwent regular training prior to the SCA. Regular training has been shown to reduce the incidence of SCA during sports activity.21 Third, we are not able to provide details regarding the level of exercise at the time of SCA for the entire period. Because there is no evidence to support a triggering effect Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 of light exertion for SCA,20 it may be possible that some of SCAs occurring during sports activities were associated by chance and not related to the activity itself. Hence our our use usee of of the the term erm ‘sports-associated’ rather than ‘sports-related’ SCA. For the SCA cases which occurred between beetw wee eenn 20 2002 02 and nd 22006, 006, an estimated metabolicc eq eequivalent uivalent (MET) T sco T) score, co ore re,, reflecting the intensity off eexercise was x rcise wa xe as cal ccalculated. alcul ulat ul ated ed.43, 44 One ed One M MET ET iss th the he am amount mounnt nt ooff en energy ner erggy gy spe spent pennt bby y a pe pers person rsson ssitting i tiing it ng quietly. quie qu ietl ie tly. tl y. P Physical hysi hy sica call aactivities cti tivviti tiies w were ere cl clas classified assi siffied fied iinto nto o tthree hrreee ggroups: roup ro upss: llight up ighht ((<4 ig < M <4 MET), ET), ET ), m moderate od der erat atee (4 (4-6 4-6 MET), and he heavy eav avyy (> (>66 ME M METS) TS)) sp TS sport por o t ac aactivity. tivi ti vity vi ty.. Ov ty Over Overall, eral er a l, amo al among mong mo ng tthe he 330 0 SC SCA A du dur during rin ng sp spor sports orts or t activities with estimated MET available between 2002 and 2006, light exertion was observed in 14% of SCA cases, whereas moderate and vigorous were observed in 50% and 38%, respectively. Finally, specific coronary pathology examination could provide important information especially details of potential sex-specific abnormalities, but were not routinely performed by the medical examiner in Portland, Oregon. In conclusion, the burden of sports-associated SCA among middle-aged participants is relatively low when compared to the overall SCA burden in the community. Our findings of a high prevalence of established cardiovascular disease as well as symptoms that manifested in 15 DOI: 10.1161/CIRCULATIONAHA.114.011988 advance of SCA highlight a prevention gap that can potentially be closed. The significant prevalence of known cardiovascular disease and prior symptoms in affected participants offers an opportunity for targeted education in order to maximize both safety and acceptance of sports activity in the middle-aged group. Acknowledgments: We gratefully acknowledge the assistance of all Emergency Medical Services personnel (American Medical Response, Portland/Gresham fire departments), the Oregon State Medical Examiner’s office and the 16 hospitals in the Portland Oregon metro area. We thank Professor David Celermajer (Sydney Medical School, Sydney) as well as Doctor Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 Wulfran Bougouin (Paris Sudden Death Expertise Center, Paris) for their helpful and constructive review of the paper. Funding Sources: This work was funded in part by National Heart, Lung, and Blood Institute gran ants tss R 01HL 01 HL10 HL 051 5170 7 and R01HL122492 to Dr.. C h gh. Dr. Chugh ho hu old ldss the Pauline and Harold grants R01HL105170 Chugh. holds Pr ric icee Chair C aiir in Cardiac Ch Car ardi diac ac Electrophysiology Eleect c ro roph phys ph ysio ys iolo logy g at gy at the the Heart Heaart Institute, In nst stit itut it u e,, Cedars-Sinai Cedar edarss-S Sin i ai Medical Med edic ical al C e te en ter, r, Price Center, L os Angeles, A geles, CA An A. E.M M. is a V isit is i in ingg F acultyy S cient ntiist att tthe he C ed darrs-Sina naii Heart na Heart Institute Insttitu titutee fun ndeed Los CA. E.M. Visiting Faculty Scientist Cedars-Sinai funded by rresearch essea e rc rchh gran ggrant rantt supp ssupport upp porrt fr ffrom om tthe he F on nda dati tioon pour ti p ur la po la Recherche Rech Re cher ch erch chee Medicale, ch Medi Me diccale cale l , the the Philip Phhillip ip Fondation Foun Fo unda un dati da tion ti on, an on andd th thee Fr Fren ench en ch S ocie oc iety ie ty ooff Ca Card rdio rd iolo io logy lo gy. gy Foundation, French Society Cardiology. Conflict of Interest Disclosures: None. References: 1. Fishman GI, Chugh SS, Dimarco JP, Albert CM, Anderson ME, Bonow RO, Buxton AE, Chen PS, Estes M, Jouven X, Kwong R, Lathrop DA, Mascette AM, Nerbonne JM, O'Rourke B, Page RL, Roden DM, Rosenbaum DS, Sotoodehnia N, Trayanova NA, Zheng ZJ. Sudden cardiac death prediction and prevention: report from a National Heart, Lung, and Blood Institute and Heart Rhythm Society Workshop. Circulation. 2010;122:2335-2348. 2. Roger VL, Go AS, Lloyd-Jones DM, Benjamin EJ, Berry JD, Borden WB, Bravata DM, Dai S, Ford ES, Fox CS, Fullerton HJ, Gillespie C, Hailpern SM, Heit JA, Howard VJ, Kissela BM, Kittner SJ, Lackland DT, Lichtman JH, Lisabeth LD, Makuc DM, Marcus GM, Marelli A, Matchar DB, Moy CS, Mozaffarian D, Mussolino ME, Nichol G, Paynter NP, Soliman EZ, Sorlie PD, Sotoodehnia N, Turan TN, Virani SS, Wong ND, Woo D, Turner MB. Heart disease 16 DOI: 10.1161/CIRCULATIONAHA.114.011988 and stroke statistics--2012 update: a report from the American Heart Association. Circulation. 2012;125:e2-e220. 3. Harmon KG, Asif IM, Klossner D, Drezner JA. Incidence of Sudden Cardiac Death in National Collegiate Athletic Association Athletes. Circulation. 2011;123:1594-1600. 4. Maron BJ, Doerer JJ, Haas TS, Tierney DM, Mueller FO. Sudden deaths in young competitive athletes: analysis of 1866 deaths in the United States, 1980-2006. Circulation. 2009;119:10851092. 5. Drezner JA, Levine BD, Vetter VL. Reframing the debate: Screening athletes to prevent sudden cardiac death. Heart Rhythm. 2013;10:454-455. 6. Drezner JA. Contemporary approaches to the identification of athletes at risk for sudden cardiac death. Curr Opin Cardiol. 2008;23:494-501. Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 7. Uberoi A, Stein R, Perez MV, Freeman J, Wheeler M, Dewey F, Peidro R, Hadley D, Drezner J, Sharma S, Pelliccia A, Corrado D, Niebauer J, Estes NAM, Ashley E, Froelicher Froelicheer V. V Interpretation nterpretation of the Electrocardiogram of Young Athletes. Circulation. 2011;124:746-757. 2011;124 244:7 7466-7 -757 57.. 57 8. Kaltman JR, Thompson PD, Lantos J, Berul CI, Botkin J, Cohen JT, Cook NR, Corrado D, ShapiroDrezner J, Frick KD, Goldman S, Hlatky M, Kannankeril PJ, Leslie L,, Priori S, Saul JP, Shapiro Mendoza Friedman Mend Me ndooza nd oza CK, CK Siscovick Siisc scov o ick D, Vetter VL, Boineauu R, R, Burns KM, Fri riedma ri maan RA. Screening for Sudden Cardiac Death Young: Report National Heart, Lung, Blood Su uddden Cardi diacc D di eath ea th iin n th thee Yo oun ung: g: R epor ep ortt Fr From om m a Nat attio iona n l He na Hea art,, L ungg, aand un ndd B lood lo od IInstitute n tiitu ns tute te Working Group. Work Wo rking Grou up. Circulation. Circ rcul ulaati ation ion. 2011;123:1911-1918. 20111;12 2011 ;123:19111--19118. 9.. D Drezner Detect, manage, shift the athletes with cardiac reezn z er JJA. A. D A. ettec ectt, t, m anag an ag ge, iinform: nfoorm nf orm: a pparadigm arad adig ad ig gm sh hift iin hift n th he care care ooff at thl hlet etes et ess w ithh ca it ard dia iacc disorders? diso ord rders? s? Br B J Sports Spoort rtss Med. Med 2013;47:4-5. 2013 20 13;4 ;47:4-5. 5. 10. Incidence jogging 10 Thompson Thom Th omps pson on PD, PD Funk Fun unkk EJ, EJ Carleton Carl Ca rlet eton on RA, RA Sturner Stu turn rneer WQ. WQ In Inci cide denc ncee of ddeath eath ea th dduring urin ur ingg jo jogg ggin ingg in Rhode Island from 1975 through 1980. JAMA. 1982;247:2535-2538. 11. Harris KM, Henry JT, Rohman E, Haas TS, Maron BJ. Sudden death during the triathlon. JAMA. 2010;303:1255-1257. 12. Marijon E, Tafflet M, Celermajer DS, Dumas F, Perier MC, Mustafic H, Toussaint JF, Desnos M, Rieu M, Benameur N, Le Heuzey JY, Empana JP, Jouven X. Sports-related sudden death in the general population. Circulation. 2011;124:672-681. 13. Berdowski J, de Beus MF, Blom M, Bardai A, Bots ML, Doevendans PA, Grobbee DE, Tan HL, Tijssen JG, Koster RW, Mosterd A. Exercise-related out-of-hospital cardiac arrest in the general population: incidence and prognosis. Eur Heart J. 2013;34:3616-3623. 14. Marijon E, Bougouin W, Perier MC, Celermajer DS, Jouven X. Incidence of sports-related sudden death in France by specific sports and sex. JAMA. 2013;310:642-643. 17 DOI: 10.1161/CIRCULATIONAHA.114.011988 15. Marijon E, Bougouin W, Celermajer DS, Périer MC, Dumas F, Benameur N, Karam N, Lamhaut L, Tafflet M, Mustafic H, de Deus NM, Le Heuzey JY, Desnos M, Avillach P, Spaulding C, Cariou A, Prugger C, Empana JP, Jouven X. Characteristics and outcomes of sudden cardiac arrest during sports in women. Circ Arrhythm Electrophysiol. 2013;6:1185-1191. 16. Chugh SS, Jui J, Gunson K, Stecker EC, John BT, Thompson B, Ilias N, Vickers C, Dogra V, Daya M, Kron J, Zheng ZJ, Mensah G, McAnulty J. Current burden of sudden cardiac death: multiple source surveillance versus retrospective death certificate-based review in a large U.S. community. J Am Coll Cardiol. 2004;44:1268-1275. 17. Reddy PR, Reinier K, Singh T, Mariani R, Gunson K, Jui J, Chugh SS. Physical activity as a trigger of sudden cardiac arrest: the Oregon Sudden Unexpected Death Study. Int J Cardiol. 2009;131:345-349. 18. Vandenbroucke JP. The making of STROBE. Epidemiology. 2007;18:797-799. Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 19. Austin PC. An Introduction to Propensity Score Methods for Reducing the Effects of Confounding in Observational Studies. Multivariate Behav Res. 2011;46:399-424. 2011;46:399-424 4. Stampfer MJ, Albert 20. Whang W, Manson JE, Hu FB, Chae CU, Rexrode KM, Willett WC, Stampf pfer err M J, A lber lb ertt CM. Physical exertion, exercise, and sudden cardiac death in women. JAMA. 2006;295:13991403. 21. 21 1. Albert Alb rt CM, Albe CM, M, Mittleman Mit i tl tlem em man n MA, MA, Chae Cha h e CU, CU, Lee Lee IM, IM M, Hennekens Henn nnnek eken e s CH, CH, Manson Mans Ma n onn JE. ns JE. Triggering Tri rigg gggerrin i g of o sudden Med. uddden death from fro rom m cardiac card ca r ia rd iacc causes caause sess by vigorous vig goroous exertion. exeert ertionn. N En Engl gl J M ed d. 22000;343:1355-1361. 0000;3 343 43:1 :135 :1 35535 5 13361. 5611 22. Med 1986;711:20522 2. Vuori Vuor Vu orii I. I. The The cardiovascular caardi ardiov ovvas ascu ula l r risks risk ri skss of sk of physical phy hyssica call activity. ca activvity act vi y. Acta Acta M ed d SScand cand can nd SSuppl. uppl up pl.. 19 pl 986 6;7 711 11::20505 214. 4. 23. Siscovick Cardiol 23 Sisc Si scov ovic ickk DS. DS Exercise Exer Ex erci cise se and and its its role rol olee in sudden sud uddden cardiac car ardi diac ac death. dea eath th Ca Card rdio ioll Clin. Clin Cl in 1997;15:467-472. 1997 19 97;1 ;15: 5:46 4677-47 4722 24. Albert CM, McGovern BA, Newell JB, Ruskin JN. Sex differences in cardiac arrest survivors. Circulation. 1996;93:1170-1176. 25. Deo R, Albert CM. Epidemiology and genetics of sudden cardiac death. Circulation. 2012;125:620-637. 26. Dunn AL, Marcus BH, Kampert JB, Garcia ME, Kohl HW, 3rd, Blair SN. Comparison of lifestyle and structured interventions to increase physical activity and cardiorespiratory fitness: a randomized trial. JAMA.1999;281:327-334. 27. Thompson PD, Franklin BA, Balady GJ, Blair SN, Corrado D, Estes NA, 3rd, Fulton JE, Gordon NF, Haskell WL, Link MS, Maron BJ, Mittleman MA, Pelliccia A, Wenger NK, Willich SN, Costa F, American Heart Association Council on Nutrition PA, Metabolism, American Heart Association Council on Clinical C and American College of Sports M. Exercise and acute cardiovascular events placing the risks into perspective: a scientific statement from the American 18 DOI: 10.1161/CIRCULATIONAHA.114.011988 Heart Association Council on Nutrition, Physical Activity, and Metabolism and the Council on Clinical Cardiology. Circulation. 2007;115:2358-2368. 28. Fletcher GF, Ades PA, Kligfield P, Arena R, Balady GJ, Bittner VA, Coke LA, Fleg JL, Forman DE, Gerber TC, Gulati M, Madan K, Rhodes J, Thompson PD, Williams MA, American Heart Association Exercise CR, Prevention Committee of the Council on Clinical Cardiology CoNPA, Metabolism CoC, Stroke N, Council on E and Prevention. Exercise standards for testing and training: a scientific statement from the American Heart Association. Circulation. 2013;128:873-934. 29. Koller A, Shephard RJ, Balady GJ. Exercise as cardiovascular therapy. Circulation. 2000;101:E164. 30. Schober P, van Dehn FB, Bierens JJ, Loer SA, Schwarte LA. Public access defibrillation: time to access the public. Ann Emerg Med. 2011;58:240-247. Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 31. Bobrow BJ, Vadeboncoeur TF, Spaite DW, Potts J, Denninghoff K, Chikani V, Brazil PR, Ramsey B, Abella BS. The effectiveness of ultrabrief and brief educational videoss fo training forr tr trai aini ning ngg lay ay responders in hands-only cardiopulmonary resuscitation: implications for thee future fu utu t ree ooff citizen citi ci tize z n cardiopulmonary resuscitation training. Circ Cardiovasc Qual Outcomes. 2011;4:220-226. 2011;4 ;4:2 :2 220 20-2 226 26. 32. Marijon E, Bougo Bougouin g uin W, Celermajer DS, Perier MC, Benameur N, Lamhaut L, Karam N, Dumas Duma Du mass F, ma F, Tafflet Taf afflet ett M, M, Prugger C, Mustafic H, Rifler Rifl fler fl er JP, Desnos M, Lee Heuzey Heuz He u ey JY, Spaulding CM, P,, Ca Cariou A,, Em Empana X.. M Major disparities after CM M, Avillach A illach Av ch P C riou ri ou uA Empa pana pa n JJP, na P,, JJouven ouve ou venn X ajjorr rregional egiona eg nal di na disp sppar arit i iees in n ooutcomes utco ut come mess af me afte t r te sudden uddden cardiac ac arrest arrres estt during duuri ring ng sports. sport portts. s Eur Eu ur Heart Heaart art J. 2013;34:3632-3640. 2013 20 0 3;3 ;34: 4:33632 3632--3640. 6 40 33. Sasson C,, M Meischke H,, Abel Abella BS, Berg Bobrow BJ, Chan Root ED, Heisler M,, 33 3. Sa Sass s on C ss eissch chkke ke H A bel ella la B S, B ergg RA er RA,, Bo Bobr brrow wB J, C han PS han PS, Roo R oot ot E D, H eissleer er M Levy Masoudi vy JJH, H, Link Lin i k M, M M a ouudi as d F, F, Ong Ong M, Sayre Say ayre re MR, MR, R Rumsfeld Rum umsf sfel eldd JS, JS Rea Rea TD. T . Increasing TD Incr In crea easi sing g cardiopulmonary with cardiopulmon on nar aryy resuscitation resu re s sc su scit i attio ionn provision prov pr ovis ov i io is on in communities com ommu munnit mu i iees wi w th llow ow bbystander ysta ys taand nder e ccardiopulmonary er ardi ar diop di opul op u monary resuscitation rates: American Heart Association esu susc scit itat atio ionn ra rate tes: s: a sscience cien ci ence ce aadvisory dvis dv isor oryy fr from om the the Am Amer eric ican an H eart ea rt A ssoc ss ocia iati tion on ffor or hhealthcare ealt ea lthc hcar aree providers, policymakers, public health departments, and community leaders. Circulation. 2013;127:1342-1350. 34. Herlitz J, Ekstrom L, Wennerblom B, Axelsson A, Bang A, Holmberg S. Effect of bystander initiated cardiopulmonary resuscitation on ventricular fibrillation and survival after witnessed cardiac arrest outside hospital. Br Heart J. 1994;72:408-412. 35. Bobrow BJ, Clark LL, Ewy GA, Chikani V, Sanders AB, Berg RA, Richman PB, Kern KB. Minimally interrupted cardiac resuscitation by emergency medical services for out-of-hospital cardiac arrest. JAMA. 2008;299:1158-1165. 36. Drezner JA, Rao AL, Heistand J, Bloomingdale MK, Harmon KG. Effectiveness of emergency response planning for sudden cardiac arrest in United States high schools with automated external defibrillators. Circulation. 2009;120:518-525. 37. Drezner JA. Preparing for sudden cardiac arrest--the essential role of automated external 19 DOI: 10.1161/CIRCULATIONAHA.114.011988 defibrillators in athletic medicine: a critical review. Br J Sports Med. 2009;43:702-707. 38. Drezner JA, Rogers KJ. Sudden cardiac arrest in intercollegiate athletes: detailed analysis and outcomes of resuscitation in nine cases. Heart Rhythm. 2006;3:755-759. 39. Drezner JA, Chun JSDY, Harmon KG, Derminer L. Survival trends in the United States following exercise-related sudden cardiac arrest in the youth: 2000-2006. Heart Rhythm. 2008;5:794-799. 40. American College of Sports Medicine and American Heart Association joint position statement: automated external defibrillators in health/fitness facilities. Med Sci Sports Exerc. 2002;34:561-564. Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 41. Drezner JA, Courson RW, Roberts WO, Mosesso VN, Jr., Link MS, Maron BJ. Interassociation task force recommendations on emergency preparedness and management of sudden cardiac arrest in high school and college athletic programs: a consensus statement. Heart Rhythm. 2007;4:549-565. 42. Drezner JA, Asif IM, Harmon KG. Automated external defibrillators in healt health lthh an aand d fi ffitness tnes tn esss es facilities. Phys Sportsmed. 2011;39:114-118. 43. Ainsworth BE,, Haskell WL, Whitt MC, Irwin ML, Swartz AM, Strath SJ, O'Brien WL, Bassett KH, Emplaincourt PO, Jacobs Bass Ba sset ss ettt DR, et DR, Jr., Jr., Schmitz Schmitz ch Jacobs DR, Jr., Leon L onn AS. Le AS. Compendium of physical activities: MET Sci Sports Exerc. phhyssic i al act ctiv ivittie iv ies: s an s: an update upda up date da te of of activity acti ac tivi vity ty y ccodes odes od es aand ndd M ET T iintensities. nten nt e siiti tiees. Med Meed Sc ci Sp Spor orts or ts E xeerc r . 2000;32:S498-504. 2000;32:S498 00 8-5 -504 04. 04 44. Mittleman Maclure Tofler Sherwood Goldberg RJ, Muller Triggering 444. Mi Mitt t le tt lema mann MA ma MA,, M acclur clu e M, T ofle of lerr GH GH,, Sh her e wood ood JB JB,, Go Gold l berg ld berg R J, M ulleer JE ulle JE.. Tr rig igge g riing ge g oof acute myocardial physical exertion. Protection triggering regular acut utee my m ocar oc a di d al a iinfarction nfar nf arctio ionn by hheavy eavy phy ea hysi sica call ex exertion on. Pr Prot otec ection on aagainst gainst ga st tr rig gge gering g bby y re regu gulaar exertion. Determinants Med. Dete teerm rmin in nan ants ts of of Myocardial Myoccar My ardi diial a Infarction Infa In farc fa rcti rc tion ti on n Onset Onsset e Study Stu tudy dy Investigators. Inv nvessti t ga gato tors to rs.. N En rs Engl gl J M ed. 1993;329:1677-1683. 1993 19 93;3 ;329 29:1 :167 6777-16 1683 83 20 DOI: 10.1161/CIRCULATIONAHA.114.011988 Table 1. Patient Characteristics for SCA Associated With Sports Versus Not Associated With Sports. Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 Demographic data Age — yr Mean±SD 35–50 50–65 Timing — no. (%) Weekend Timing Morning (6:00 am to 12:00 pm) Afternoon (12:00 pm to 6:00 pm) Night (6:00 pm to 06:00 am) Unknown Seasons Summer Autumn Winter Sppri ring ng Spring Nu umber mb off ca card rdio iova io vasc sccul ular ar risk ris isk k factor f ct fa ctor or Number cardiovascular no (%) — no. Non None One One More than tha hann one on ne More Type of cardiovascular card dio iova vasc va scul sc ular ul ar ris risk isk is k fa factor act ctor orr — no. no (%) (%) Diabetes mellitus Dyslipidemia Systemic hypertension Body mass index (Kg/m2) Smoking Known heart disease — no. (%)* Coronary artery disease Atrial fibrillation Heart failure Pacemaker Implantable Cardioverter Defibrillator Sports-Associated SCA N=63 Non SportsAssociated SCA N=1,184 P Value 51.1±9 39 (62) 24 (38) 53.1±8 648 (55) 536 (45) 0.08 0.26 28 (44) 314 (27) 0.002 <0.001 16 (25) 23 (37) 7 (11) 17 (27) 358 (30) 268 (23) 234 (20) 324 (27) 00.24 0. 24 19 (30) 14 (22) 12 (19) 188 (29) 258 (22) 288 (24) 340 (29) 298 (25) 298 0. .38 0.38 18 8 ((43) 43 3) 9 ((19) 199) (38 38)) 18 (38) 3544 ((33) 35 33) 3 3) 15 59 (1 (15) 5) 159 5 9 (48) 50 (4 48) 509 4 (8) 16 (33) 19 (40) 29±6 10 (31) 10 (16) 5 (8) 3 (5) 3 (5) 3 (5) 0 (0) 315 (28) 290 (26) 528 (47) 30±8 451 (61) 358 (30) 220 (19) 64 (5) 185 (16) 56 (5) 2 (0) 0.002 0.27 0.28 0.21 0.001 0.01 0.03 0.82 0.02 0.95 1 SD denotes Standard Deviation. Percentages were calculated on the basis of the total number of known events. * Among consent survivors or deceased patients with medical records available (N=583, including 45 sportsassociated SCA). 21 DOI: 10.1161/CIRCULATIONAHA.114.011988 Table 2. Setting and Outcomes of SCA Associated With Sports Versus Not Associated With Sports. Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 Public occurrence — no. (%) Sudden death witnessed — no. (%) Bystander CPR — no. (%) First rhythm recorded on preadmission electrocardiogram — no. (%) Ventricular fibrillation Asystole Pulseless electrical activity Undetermined Call-to-EMS arrival — no. (%) Mean±SD 8min ROSC — no. (%) Survival to hospital discharge — % (95% 95% % cconfidence onfide on dencce in de interval) Sports-Associated SCA N=63 55 (90) 55 (87) 28 (44) Non SportsAssociated SCA N=1,184 242 (22) 614 (52) 300 (25) 42 (84) 4 (8) 4 (8) 0 (0) 437 (51) 180 (21) 228 (27) 9 (1) 6.79±4 34 (77) 24 (39) 23.2 (11.8-34.6) 6.80±4 631 (79) 9) 241 (29)) 13.6 (11.6-15.5) EM EMS MS de deno denotes n tees Em Emer Emergency rge genccy Medical Services; ROSC, Return rn O Off Spontaneous Ci Circulation irculat atio i n io Percentages erceentages en were were ccalculated alcu al cula cu late teed on tthe h bbasis he asis as is ooff th thee to ttotal taal nu numb number mbeer ooff known kn now ownn events. even ev nts ts. 22 P Value <0.001 <0.001 0.001 <0.001 0.99 0.99 00.44 .444 .4 0.11 11 0.11 0.04 DOI: 10.1161/CIRCULATIONAHA.114.011988 Table 3. Coronary Artery Disease Associated With Sudden Cardiac Arrest: Sports Versus Not Associated With Sports. Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 Sports-Associated SCA N=63 SCA with cause assessed — no. (%) 43 (68) Frequency of CAD — no. (%) 36 (84) Coronary presentation Acute MI — no. (%) 12 (33) History of CAD — no. (%) 3 (25) No history — no. (%) 9 (75) No Acute MI — no. (%) 24 (66) History of CAD — no. (%) 17 (71) No history — no. (%) 7 (29) History of CAD — no. (%) 20 (56) Prior revascularization 2 (10) Surgical 1 (5) PCI 1 (5) History of angina 0 (0) History Hist Hi sttor oryy of MI MI 122 (60) (60 6 ) Mean 48.1±18 Mean EF F 48.1 48 .11±18 Non Sports-Associated P Value SCA N=1,184 786 (66) 0.89 717 (91) 0.10 0.23 169 (24) 69 (41) 100 (59) 548 (76) 428 (78) 120 (22) 497 (69) 0.08 138 (28) 0.12 0.1 .12 74 (15) 64 (13) 22 (4) 0.99 246 24 (49) 0.37 47.1±16 0.84 47.1±1 47 ±166 0 84 0. 8 CAD denotes coronary CAD co oro ona n ry y aartery rter rt eryy di dis disease; seas seas asee; e; EF, EF, ejection eje ject ctiion fr frac fraction ction n off thee le left eft vventricle; en ntr tric icle le; MI MI,, my myocardial yocar ardi ar dial di al iinfarction; nfar nf a ct ar ctio i n;; P io PCI, C, CI percutaneous pee cutaneous coronary perc coronaaryy intervention. intterv ventioon.. Percentages Peerc r en entages were weere ca calculated alcculateed oon n tthe he bbasis a is ooff th as thee total to nu number umbeer ooff known knoown kn own events. ev ventss. 23 DOI: 10.1161/CIRCULATIONAHA.114.011988 Figure Legends: Figure 1. Panel A – Proportion of patients with return of spontaneous circulation and survival to hospital discharge, according to sudden cardiac arrest (SCA) occurring during sports or not during sports; Panel B – Odds ratio for survival to hospital discharge of Sports SCA compared to Non-Sports SCA (crude and adjusted for age, sex, initial rhythm, response time, presence of witness, bystander cardiopulmonary resuscitation, ventricular fibrillation). Error bars indicate upper 95% confidence interval. Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 Figure 2. Distribution of Cardiovascular Abnormalities Associated With Suddenn Cardiac Car a di diac acc Arrest Arr r es et SCA) in the 1,247 Subjects, According to Sports SCA (Upper Pie, N=63) and Non-Sports SCA (SCA) Low ower er Pie, Pie ie,, N=1,184). N 1, N= 1,1184). 18 (Lower 24 Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 Figure 1A Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 3 2.5 2 1.5 1.5 1 0.5 0.5 5 0 Crude OR for Survival Figure 1B Adjusted OR for Survival Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 Figure 2 Sudden Cardiac Arrest During Sports Activity in Middle Age Eloi Marijon, Audrey Uy-Evanado, Kyndaron Reinier, Carmen Teodorescu, Kumar Narayanan, Xavier Jouven, Karen Gunson, Jonathan Jui and Sumeet S. Chugh Circulation. published online April 6, 2015; Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 2015 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7322. Online ISSN: 1524-4539 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circ.ahajournals.org/content/early/2015/03/17/CIRCULATIONAHA.114.011988 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation is online at: http://circ.ahajournals.org//subscriptions/