Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Psychopharmacology wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Adherence (medicine) wikipedia , lookup
Neuropharmacology wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Discovery and development of ACE inhibitors wikipedia , lookup
Discovery and development of angiotensin receptor blockers wikipedia , lookup
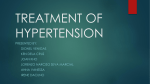
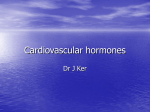
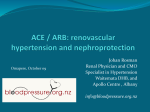
Comparison of the angiotensin II antagonist losartan with the angiotensin converting enzyme inhibitor enalapril in patients with essential hypertension Ilkka Tikkanen, Per Omvik* and Henrik Æ. Jensen† for the Scandinavian Study Group‡ Objective: To evaluate the blood pressure lowering efficacy as well as tolerability and safety of the angiotensin II antagonist losartan compared with that of the angiotensin converting enzyme inhibitor enalapril in patients with rnild-to-moderiate essential hypertension. Design and methods: The study was a multicentre, double-blind, double-dummy, randomized, parallel study. Patients (n = 407) with diastolic blood pressure >95 and < 120 mmHg at the end of a 2-week baseline placebo period were randomly allocated to receive either 50 mg losartan once a day or 20 mg enalapril once a day for 12 weeks. Blood pressure, clinical and laboratory safety, specific symptoms including coughing determined using a symptoms questionnaire and metabolic variables were examined at baseline and at weeks 6 and 12. Results: Both losartan and enalapril decreased systolic and diastolic blood pressure from baseline at weeks 6 and 12. Blood pressure changes from baseline at trough (22-26 h after the dose) did not differ between the two groups in the per-protocol analysis. Response to treatment at trough was excellent or good (diastolic blood pressure < 90 mmHg or reduction in diastolic blood pressure of 10 mmHg) in 51 and 53% of the patients in the losartan and enalapril groups, respectively. Enalapril administration increased dry coughing symptoms whereas losartan did not. The incidence of dry coughing was 1.0 and 1 2.2% as a spontaneously reported discomfort at week 12 and 3.0 and 15.1% as a clinical adverse experience in the losartan and enalapril groups, respectively. The difference from baseline at week 12 in the incidence of dry coughing between the two groups was 1 4.9% as a specific symptom in the symptoms questionnaire, Losartan reduced serum uric acid concentration, whereas effects on other metabolic parameters did not differ between the groups. Conclusions: Losartan is an effective and well-tolerated antihypertensive drug showing similar blood-pressure-lowering efficacy to that of enalapril at trough. However, in contrast to enalapril, losartan does not increase the incidence of dry coughing. Thus, the angiotensin lI antagonist losartan provides a promising new approach to treatment of hypertension. Journal of Hypertension 1995, 13:1343 -1351 Keywords: angiotensin II antagonist, losartan, angiotensin converting enzyme inhibitor, enalapril, blood pressure, cough, side effects, essential hypertension Introduction Inhibition of the renin-angiotensin system by means of angiotensin converting enzyme inhibitors has proved efficacious in the treatment of hypertension and other cardiovascular diseases. The development of specific type 1 angiotensin II receptor (AT 1 ) antagonists [1,2] has recently provided a new tool to inhibit the renin—angiotensin system. Experimental data and preliminary clinical experience suggest that the efficacy From the Department of Medicine, Helsinki University Central Hospital, Helsinki, Finland, the *Medical Department A, Haukeland Hospital, Bergen, Norway, and the †Hvidovre University Hospital, Denmark. ‡See Appendix. Requests for reprints to Dr I. Tikkanen, Department of Medicine, Helsinki Universjty Central Hospital, Unioninkatu 38, FIN-00170 Helsinki, Finland. Date of receipt: 6 March 1995; revised: 7 August 1995; accepted: 9 August 1995. © Rapid Science Publishers ISSN 0263-6352 1343 1344 Journal of Hypetension 1995, Vol 13 No. 11 of angiotensin II antagonists in the treatment of hypertension is similar to that of angiotensin converting enzyme inhibitors [3,4]. However, those two drug categories also have potential differences because of different mechanisms of action. The anigiotensin converting enzyme inhibitors may have actions that are not related to inhibition of the renin-angiotensin system by preventing the breakdown of bradykinin and other biologically active peptides [5,6]. However, a more complete blockade of the renin-angiotensin system may be achieved by treatment with angiotensin II antagonists, compared with angiotensin converting enzyme inhibitors, because it has been suggested that significant amounts of angiotensin II are also generated by non-angiotensin converting enzymes not affected by angiotensin converting enzyme inhibitors [7]. In clinical practice, the possible differences between angiotensin converting enzyme inhibitors and angiotensin II antagonists may concern not only antihypertensive efficacy but also tolerability and side effects. In particular, dry coughing, which is a typical class-specific side effect of angiotensin converting enzyme inhibitors associated with accumulation ofbradykinin and substance P [8—10], is not expected during treatment with angiotensin II antagonists. Thus, whereas angiotensin converting enzyme inhibitors in general have proved to be well tolerated, treatment with angiotensin II antagonists could provide an additional advantage over angiotensin converting enzyme inhibitors. The objective of the present multicentre trial was to evaluate the efficacy of the first angiotensin II antagonist losartan compared with the angiotensin converting cnzymje inhibitor enalapril in lowering of blood pressure in patients with mild-to-moderate essential hypertension. In addition, special attention was paid to evaluating the tolcrability and safety with particular reference to coughing and effects on metabolic variables. Methods Patients Male or female patients aged 20-75 years with mild-tomoderate essential hypertension (sitting diastolic blood pressure > 95 and < 120 mmHg after 2 weeks of placebo) were included in the study. Patients were either not treated previously or had been treated with the concomitant use of up to two different antihypertensive drugs. Patients with secondary hypertension of any aetiology, significant renal impairment [serum creatinine level >150 mol/l and proteinuria >1+ by Albustix (Bayer Diagnostics, Puteaux, France)], cerebrovascular accidents, transient ischaemic attacks or hypertensive encephalopathy during the past year, myocardial infarction during the last 6 months, or angina pectoris were excluded from the study. Pregnant or nursing women and women of child-bearing potential were also excluded. Other reasons for exclusion were present use ot non-steroidal anti-inflammatory corticosteroids, or drugs known to affect blood pressure, uncontrolled diabetes mellitus (fasting blood glucose level >11 mmol/1), obesity (arm circumference > 41 cm serum potassium level < 3.5 or > 5.5 mmol/l, abnormal liver function tests (serum glutamate oxaloacetate transaminase/serum glutamate pyruvate transaminase twice the upper limit of normal), blood haemoglobin level < 100 g/dl, or any other clinically important disease or condition that might interfere with participation in the study, confound the results of the study, or produce a significant risk to the patient. In addition, patients who had previously been treated with angiotensin converting enzyme inhibitors were excluded if that treatment had been stopped because of adverse reactions or an unsatisfactory effect on blood pressure, or both. Study protocol The study was a multicentre, double-blind, doubledummy randomized, parallel study. The study protocol was approved by the local ethics committees. All of the patients gave their written informed consent to participate. Those who were currently being treated for hypertension were withdrawn from antihypertensive drugs for at least a 2-week washout period. Patients who satisfied the eligibility criteria received placebo during a single-blind 2-week baseline period. Patients with sitting diastolic blood pressure 95-120 mmHg at the end of the baseline period were randomly allocated to receive either 50 mg losartan once a day or 20 mg enalapril once a day for a period, of 12 weeks. Five clinical visits were scheduled during the study: one at screening, two at baseline, one at week 6 and one at week 12. The patients were asked to take their daily dose of the study drug in the morning. However, in order to ensure trough blood pressure values (i.e. after 24 h) the patients were instructed not to take their study drug on the days of clinical visits until after the blood pressure measurement. Blood pressure, clinical safety and specific symptoms including a cough were monitored at each clinical visit (Table 1). Patients maintained their usual diet throughout the baseline and treatment periods. Clinical and laboratory evaluations At each visit, sitting systolic (Korotkoff phase I) and diastolic (Korotkoff phase V) blood pressures were measured from the non-dominant arm using a standard mercury sphygmomanometer and an appropriate cuff size. Blood pressure values recorded were the means of three measurements taken at 1 min intervals atter 10 min of supine rest. The pulse rate was recorded at the same times. Physical examination, complete blood counts, a blood chemistry profile and urine analysis were performed at the screening visit, and abbreviated laboratory evaluations at visits shown in Table 1. Evaluation of side effects and safety Evaluation of side effects and safety was approached in three different ways. First, the incidence of cough ana other symptoms was evaluated at baseline and at weeks Losartan versus enalapril in essential hypertension Tikkanen et. al. Table 1. Study design. Trough blood pressure (22-26 h after last dose) Physical examination Laboratory examinationa Lipidsb Adverse experience Questionnaire for specific symptoms (i.e. coughing) -4 X X -2 X X x X X Weekc 0 X X X X X X 6 X X X X X 12 X X X X X X a Haemoglobin, white blood cells, serum glutamate pyruvate transaminase (aspartate transaminase), serum glutamate oxaloacetate transaminase (alanine transaminase), serum potassium, creatinine and uric acid levels, fasting blood glucose level, urinanalysi s [pH, protein, glucose by Albustix (Bayer Diagnostics, Puteaux, France)]. bSerum total cholesterol, triglycerides and high-density lipoprotein cholesterol levels. cScreening/washout period = weeks -4 to -2; placebo = weeks -2 to 0; therapy = weeks 0 to 12: losartan 50 mg once daily (n=202), enalapril 20 mg once daily (n = 205). 6 and 12 (Table 1) using a symptoms questionnaire [11]. The patients had to respond 'Yes' or 'No' to the general question: 'Have you felt any kind of discomfort during the past week?', and if 'Yes', describe 'what kind of discomfort' they felt (spontaneously reported discomfort). Second, information concerning the occurrence of the following specific symptoms during the previous week was requested separately (specific symptoms questionnaire): headache, dizziness/vertigo, dizziness on standing, weakness on exercising, muscle pain, swollen ankles, cold hands/feet, flushing, rash/itching, breathing disturbances, nasal stuffiness, dry coughing, dry mouth, taste disturbance, nausea, diarrhoea, constipation, palpitations/tachycardia, nervousness/restlessness, reduced sexual activity and other possible symptoms. Finally, clinical and laboratory adverse experiences were monitored and reported by the investigators with respect to intensity, seriousness and estimated relationship to the treatment, at timepoints (Table 1). Data analysis Primary end-points were change from baseline in the incidence of coughing as assessed by the appropriate question of the symptoms questionnaire and change from baseline in sitting diastolic blood pressure. Secondary outcome variables were change from baseline in sitting systolic blood pressure, change from baseline in the incidence of symptoms from the questionnaire, response to antihypertensive treatment in diastolic blood pressure (excellent: 90 mmHg; good: > 9.0 mmHg and reduction l0 mmHg; fair: > 90 mmHg and reduction SmmHg but < 10 nimHg; poor: > 90 mmHg and reduction < 5 mmHg) and change from baseline in metabolic parameters. Within-group changes in blood pressure variables (effi-. cacy) were reported by the use of mean change from baseline and its associated 95% confidence interval on the basis of the one-sample t-test. Between-group changes in efficacy variables were analysed by an analysis of variance model with treatment, country and study centre within country as factors. Consistency of the itreatment effect among countries was tested at the level 0.10 in an analysis of variance model with treatment country interaction in addition to the main factors. The normality of the residuals and the homogeneity of variance assumption for analysis of variance were examined graphically and tested by the Shapiro—Wilk test and Levene's test. For analysis of blood pressure variables, an additional 'perprotocol' approach was used excluding protocol violators. The exclusion criteria applied for the per-protocol analysis were violation of baseline blood pressure entry criteria, violation of the trough (22-26 h after the dose window) blood pressure measurement (data excluded at that timepoint), concomitant antihypertensive therapy during the study, not having taken the drug 2 or more days before blood pressure measurement (data excluded at that timepoint) and rounding of blood pressure measurements (data excluded at that timepoint). The analysis of symptoms (coughing) was based on the change from baseline in the percentage of patients who responded to the specific symptom question in the symptoms questionnaire, A generalized linear model (SAS/CATFMOD) was used with time, treatment and time treatment interaction. The latter term tested for between-treatment differences in the proportion of positive answers. The within-group test was based on McNernar’s test. For analysis of safety, the treatment groups were compared with regard to the incidence of clinical and laboratory adverse events by using Fishers exact test. Primarily, changes outside predefined limits in the laboratory; safety test were compared between groups using Fisher’s exact test. Secondarily, mean changes from baseline were compared between groups with an analysis of variance model and within-group comparisons were made by the use of confidence intervals on the basis of Students redistribution. All of the statistical tests are two-tailed and P-values are rounded to two decimal places. P<0.05 was considered statistically significant. 1345 1346 Journal of Hypertension 1995, Vol 13 No 11 Results Patient characteristics Four hundred and seven patients were randomly allocated in 32 centres in four countries (Denmark, Finland, Iceland and Norway) to treatment with losartan (n=202) or enalapril (n=205). The distribution of patients among centres was similar in the two treatment arms. All of the patients were white. The treatment groups were similar with respect to sex, age, secondary diagnoses and previous antihypertensive treatment (Table 2). The most common secondary diagnoses were a headache (5%) and eczema (4.5%) in the losartan group and a headache (5.9%) and menopausal disorder (4.4%) in the enalapril group. There were no significant differences between the two treatment groups with regard to the baseline mean blood pressures and pulse, or the incidence of dry coughing. Nine patients discontinued in the losartan group (six for adverse clinical experiences) and 16 in the enalapril group (14 for adverse clinical experiences during treatment). Two hundred patients were, evaluated for efficacy in the losartan group and 199 patients in th enalapril group in the 'all-patients-treated' approach (corresponding to the 'intention-to-treat' approach), an 142 and 133 patients in the 'per-protocol' approach respectively. The majority (95% at week 6 and 96%: week 12) of exclusions from the 'per-protocol' approach was due to measurements taken outside the trough (22-26 h after the dose) blood pressure measurement window. Efficacy (blood pressure) Change in diastolic blood pressure Both losartan and enalapril treatments decreased the si ting diastolic blood pressure of the patients from baseline at week 6 (P<0.01) and week 12 (P<0.01, Tab 3). The mean decrease (all-patients-treated approach) at week 12 was 8.4 mmHg in the losartan group an 10.6 mmHg in the enalapril group (P<0.01, Fig. 1) In the per-protocol approach (see data analysis), the corresponding mean changes in diastolic blood pressure at week 12 were 8.4 and 9.7 mmHg (between-group difference NS) in the losartan and the enalapril group respectively (Fig. 1). Table 2. Summary of patient characteristics. Losartan Enalapril n % 80 122 % n % n 39.6 60.4 71 • 134 34.6 65.4 151 256 37.1 62.9 8 43 75 48 28 4.0 21.3 37.1 23.8 13.9 11 27 77 62 28 5.4 13.2 37.6 30.2 13.7 1.9 70 152 110 56 4.7 17.2 37.3 27.0 13.8 130 32 13 11 2 3 11 64.4 15.8 6.4 5.5 1.0 1.5 5.5 143 25 15 7 0 2 13 69.8 12.2 7.3 3.4 0.0 1.0 6.3 273 57 28 18 2 5 24 67.1 14.0 6.9 4.4 0.5 1.2 5.9 123 79 60.9 39.1 126 79 61.5 38.5 249 158 61.2 38.8 Sex Female Male Age (years) < 35 35-44 45-54 55-64 > 64 Previous antihypertensive treatment None ACEI -Blocker Calcium antagonist Central antihypertensive Diuretic More than one Secondary diagnoses Yes No Total - ACEI, angiotensin converting enzyme inh ibitor. Table 3. Mean change from baseline in diastolic blood pressure at week 12 in patients treated with either losartan (50 mg once a day) enalapril (20 mg once a day). Approach Treatment n Baseline Week 12 Change from baseline All patients treated Losartan 200 103.1 ± 6.0 94.7 + 9.0 -6.4 ± 7.1(-94; -7.5)** Per protocol Enalapril Losartan Enalapril 199 142 133 103. 7 ± 6.1 102. 9 ± 6.0 103. 4 ± 5. 9 93.0 ± 17.9 94,4- ± 8,7 93.7 ± 7.8 -10.6 ± 7.2(-11.6;"9.6)** †† -6.4 ± 6.6 (-9.5; -7.3)** -9.7 ± 7.2 (-10.9; -6.5)** Values are expressed as means SD (95% confidence limits).**P<0.01, versus baseline; ††P<0.01, versus losartan treatment. Losartan versus enalapril in essential hypertension Tikkanen et al. 1347 Table 4. Mean choree from baseline in systolic blood pressure at week 12 in patients treated with either losartan or enalapril. Approach Treatment n Baseline Week 12 Change from baseline All patients treated Per protocol Losartan Enalapril Losartan Enalapril 200 199 142 133 157.5 ± 17.1 158.8 ± 16.5 156.5 ± 16. 4 158.3 + 16.7 Values are expressed as means SD (95% confidence limits).**P<0.01, versus baseline; Change in Diastolic Blood Pressure at 12 weeks Fig. 1. The mean change in sitting diastolic blood pressure from baseline at week 1 2 in patients treated with either losartan (50 mg once a day) or enalapril (20 mg once a clay). Results based on the 'all-patientstreated' approach and the 'per-protocol' approach are shown. 146.9 ± 18.3 146.0 ± 16.9 145.6 ± 17.1 145.5 ± 16. 6 ††P<0.01, -10.6 ± 13.0 (-12.4; -8.8)** -12.9 ± 12.9 (-14.7; -11.1)**† -10.9 ± 12.0 (--12. 9; -8.9)** -12.8 ±1 2.1 (-14.8; -10.7)** versus losartan treatment. Change in Systolic Blood Pressure at 12 weeks Fig. 2. The mean change in sitting systolic blood pressure from baseline at week 1 2 in patients receiving either losartan (50 mg once a day) or enalapril (20mg once a day). Results based on the 'all-patients-treated' approach and the 'per-protocol' approach are shown. When the actual time of. after-dose blood pressure measurements was taken into account, it was found that, the diastolic blood pressure lowering effect of enalapril was more pronounced if measured before 22 h after the dose (mean time 8.3 h after the last dose) compared with losartan (P<0.05). However, at trough (22-26 h after the dose, mean 24.6 h), the two treatments did not differ with respect to change in diastolic blood pressure from baseline. Response to treatment In the all-patients-treated analysis, the distribution of patients among the three categories of. response (excellent or good, fair, poor) was significantly different in favour of enalapril (P<0.05). In the per-protocol analysis, the treatment groups were similar with respect to the distribution of patients in the three categories of response. The efficacy in lowering diastolic blood pressure (response to treatment) at trough was excellent or good in 51% of the patients in the losartan group and in 53% of the patients in the enalapril group (Table 5). Change in systolic blood pressure The mean decrease in sitting systolic blood pressure from baseline was also statistically significant both in the losartan and in the enalapril groups at weeks 6 (P<0.01) and 12 (P<0.01, Table 4). The mean decrease in systolic blood pressure (all-patients-treated approach) at week 12 was 10.6 mmHg in the losartan group and 12.9 mmHg in the enalapril group (P<-0.05 for between-groups difference; Fig. 2). In the per-protocol approach at week 12, the change in mean systolic blood pressure was 10.9 mmHg in the losartan group and 12.8 mmHg in the enalapril group (P—0.08 for between-groups difference; Fig. 2). Incidence of symptoms Coughing The incidence of a dry cough given as a spontaneous symptom was 2.0% at baseline, 2.0% at week 6 and 1.0% at week 12 in the losartan group, whereas it was 3.9% at baseline, 9.3% at week 6 and 12.2% , ac week 12 in the enalapril group (P <0.01, versus losartan treatment at weeks 6 and 12). The incidence of dry coughing reported as a specific symptom in the symptoms questionnaire increased from baseline by 11.4% (P<0.01) at week 12 in the enalapril group whereas no change (-3.5%, NS) occurred in the losartan group (Fig. 3). The two groups were significantly 1348 Journal of Hypertension 1995, Vol 13 No. 11 Table 5. Response to treatment with either losartan (50 mg once a day) or enalapril (20 mg once a clay) with respect to diastolic blood pressure (DBP) lowering efficacy at week 12. Excellent/good Normalized DBP (< 90 mmHg) Reduction in DBP 10 mmHg) Fair Reduction in DBP 5 DBP 10 mmHg Poor or no response Reduction in DBP < 5 mmHg Comparison between groups (excellent or good/fair/poor) All patients tested Losartan Enalapril (n = 200) (n = 199) 51 59 34 37 17 22 Per protocol Losartan Enalapril (n = 142) (n = 133) 51 53 34 29 17 24 20 23 21 25 29 18 28 22 P 0.05 NS Values are expressed as percentages. NS, not significant. Fig. 3. The incidence of coughing reported as a specific symptom in the symptoms questionnaire at baseline and at week 12 in the losartan and enalapril groups. The change from baseline in the incidence of coughing (-3.5% in the losartan group, NS, and +11.4% in the enalapril group, P<0.01) was significantly different (14.9%, P<0.01) between the groups. different with respect to the change from baseline in the incidence of dry coughing at week 6 (between-groups difference 13.8%, P<0.01) and at week 12 (14.9%, P<0.01) in favour of losartan. The incidence of dry coughing as a clinical adverse experience reported as possibly, probably or definitely related to treatment was higher in the enalapril group (15.1%), P<0.01) than in the losartan group (3.0%)). Fig. 4. The incidence of any kind of symptoms reported at baseline and at week 12 in the losartan and enalapril groups. Table 6. Clinical adverse experiences (AE) reported by the investigators in patients treated with either losartan or enalapril. Losartan Enalapril (n = 202) (n-205) At least one AE 65 93** AE related to treatment Withdrawals caused by AE Withdrawals caused by AE related to treatment 23 6 52** 14 3 12* *P<0.05, **P<0.001, versus losartan treatment. Any symptom reported The incidence of any kind of symptom decreased from 43.3% at baseline to 29.8% at week 12 (P<0.01) in the losartan group, and from 42.8 to 35.5% (NS) in the enalapril group, respectively (Fig. 4). The difference hi the change from baseline between the two groups was not statistically significant. Symptoms other than a cough The incidence of headaches decreased significantly from baseline during treatment in both groups; the difference between the groups was not significant. No change in the incidence of other specific symptoms as reported in the symptoms questionnaire was found. However, the change from baseline in the incidence of swollen ankles at week 12 (2.5% increase in the losartan group and Losartan versus enalapril in essential hypertension Tikkanen et al. 1349 Table 7. Mean changes (%) in metallic parameters at the end or the study in patients treated with either losartan ( 50 mg once a day) or enalapril (20mg once a day) for 12 weeks. Losartan Enalapril Before After A% Glucose level Cholesterol level High-density lipoprotein cholesterol level Triglycen'des level Uric acid level Creatinine level 5,11 6,02 1.10 1.68 333 88.7 5.07 5,91 1.37 1 ,63 322 88.6 -0.8 1.8** 2.1 -3.0 -3.5** † † -0.1 ϯϯ <0.01 between groups. *P<0.05, **P<0.01, within group; 2.5% decrease in the enalapril group) differed (P<0.05) between the two groups. A marginal difference between the groups was found with respect to the incidence of a rash/itching at week 6 (P=0.07, NS) in favour of losartan. However, the absolute numbers were small and no support for such difference was found in previous publications. Safety Sixty-five patients (32.2%) in the losartan group and 93 (45.4%) in the enalapril group (P<0.01, versus losartan) had at least one clinical adverse experience during the treatment phase. Twenty-three (11.4%) adverse experiences in the losartan group and 52 (25.4%) in the enalapril group (P<0.01, versus losartan) were considered possibly, probably or definitely related to treatment. When those treatmentrelated adverse experiences were further analysed according to the body system, the two treatment groups were significantly different with respect to respiratory adverse experiences (P<0.01), and with respect to coughing in particular (P<0.01). Six patients (3.0%) were withdrawn from the therapy in the losartan group and 14 (6.8%) in the enalapril group because of clinical adverse experiences; of them three (1.5%) in the losartan group and 12 (5.9%) in the enalapril group (P<0.05, versus losartan) were considered to be drug-related (Table 6). One serious adverse experience (lipothymia considered probably not to be related to treatment) was reported in the losartan group and one (a dry cough considered definitely to be related to treatment) in the enalapril group. No serious laboratory adverse experiences were reported and treatment of no patient was discontinued because of adverse laboratory experiences. Metabolic parameters Losartan reduced the serum uric acid concentration at the end of the study compared with baseline (P<0.01) whereas enalapril did not (P<0.01 for between-groups difference). The two groups did not differ concerning the other metabolic parameters studied (Table 7). A small but significant decrease in serum total cholesterol level was observed in the losartan group (P<0.01). A slight increase in serum creatinine level was found in the enalapril group (P<0.05) whereas no change was observed in the losartan group. Before 5.09 6.06 1.37 1.77 347 90.3 After 5.09 6.05 1.35 1.73 354 91.8 A% 0 -0.2 1.5 2.3 2.2 1.7* Discussion The present study is the largest double-blind, randomized multicentre trial so far to have compared an angiotensin II antagonist and an angiotensin converting enzyme inhibitor in patients with essential hypertension. It shows that the blood pressure-lowering efficacy of losartan, a specific AT1-type angiotensin II receptor antagonist, is similar to that of enalapril, a previously well documented angiotensin converting enzyme inhibitor [12,13], It was also found that treatment with losartan is associated with a significantly lower incidence of adverse experiences, notably coughing, than is treatment with enalapril. Thus, although angiotensin converting enzyme inhibitors in general are considered to be tolerated well [13,14], treatment with the angiotensin II antagonist losartan appears to provide additional benefits. The comparison of angiotensin II antagonists and angiotensin converting enzyme inhibitors in the treatment of hypertension is of special interest because both drugs act by inhibiting the renin-angiotensin system [3], which is the key system involved in the regulation of blood pressure and sodium and water balance [15]. However, there are also potential differences between those two types of drugs because of their different mechanisms of action. Being inhibitors of kininase II, angiotensin converting enzyme inhibitors have been shown to potentiate bradykinin-mediated effects, which may contribute both to the efficacy and to the side effects of angiotensin converting enzyme inhibitors [3-6]. However, specific angiotensin II antagonists, unlike angiotensin converting enzyme inhibitors, are able to antagonize the effects of angiotensin II regardless of the enzymatic pathway by which angiotensin II is generated [3-6]. According to a recent theory that has not been demonstrated to be valid in hypertensive patients, significant amounts of angiotensin II may also be generated by enzymes other than angiotensin converting enzyme, such as chymase [7]. It should be added that the majority of the effects of angiotensin II are mediated by AT 1 receptors whereas the biological significance of AT 2 receptors remains largely unknown At the doses used in the present study namely 50 mg losartan once a day versus 20 mg enalapril once a day, 1350 Journal of Hypertension 1995, Vol 1 3 No 11 enalapril was marginally more effective in reducing diastolic blood pressure than was losartan as judged by blood pressure changes in all of the treated patients. However, at trough, the two drugs were equally effective, in accord with earlier observations [16-18]. According to the present data, enalapril seemed to be more effective approximately 3 h after the close compared with blood pressure values obtained at trough. A similar trend was not found in the losartantreated patients. That is compatible with ambulatory blood pressure measurements showing a smooth blood pressure lowering profile over 24 h with losartan [18,19], and the documented long duration of action of losartan resulting in peak: trough ratios consistently above 50% [16,18]. The present study design compared 20 mg enalapril once a day with 50 mg losartan once a day. It should be noted that the enalapril dose used was relatively high, exceeding the average dose of enalapril used in the treatment of hypertension. In previous studies comparing losartan with other antihypertensive drugs, losartan has been reported to be as effective as atenolol [20], hydrochlorothiazide [21] and felodipine (Merck Sharpe & Dohme Ltd, Whitehouse Station, New Jersey, USA, data on file, 1994). An important finding in the present, study was that enalapril increases the incidence of dry coughing whereas losartan does not. The higher incidence of coughing in the enalapril-treated patients compared with losartan was demonstrated by three different methods used to evaluate cough symptoms: coughing as a spontaneously reported discomfort, dry coughing as a specific symptom in the symptoms questionnaire, and dry coughing reported as a clinical adverse experience. Dry coughing is now considered to be a class-specific side effect of angiotensin converting enzyme inhibitors depending on their ability to potentiate bradykininmediated responses [5,8—10]. The present data prove that inhibition of the renin—angiotensin system by a specific angiotensin II antagonist is not associated with increased incidence of dry coughing. Previous studies have shown that the incidence of dry coughing in hypertension treatment trials varies considerably according to the methodology applied for evaluation of that adverse effect [9]. In accord with that, the occurrence of coughing at baseline varied from 2.0% as a spontaneously mentioned discomfort to 17.9% when patients were asked specifically in a symptoms questionnaire in the present study. However, the difference in incidence of dry cough between the enalapril group and the losartan group was found to be remarkably constant ranging from 11.2 to 14.9% at week 12 irrespective of the method used to estimate that side effect. Thus, those drugs with different mechanisms of action to inhibit the renin-angiotensin system are clearly different with respect to specific side effects in patients with essential hypertension. It was interesting to find that losartan treatment decreased even the total proportion of symptoms compared with the baseline placebo period. Thus, the present data support the view [16,17,22] that losartan could be an exceptionally well tolerated antihypertensive drug. Further studies exploring the effects of losartan on side eflects and other aspects of the quality of life in comparison with other antihypertensive drugs are warranted. Losartan induced fewer clinical adverse experiences than did enalapril and the treatment was discontinued less often, because of drug-related side effects in the losartan group than in the enalapril group. Neither drug had clinically significant effects on plasma glucose levels or lipid parameters. The present data also confirmed the previous findings that losartan lowers the serum uric acid concentration [17,19]. That effect appears to be a consequence of a uricosuric action of losartan [17], which is not shared by all angiotensin II antagonists [23]. Neither the exact mechanism nor the possible clinical significance of that finding arc clear. In summary, losartan, a novel angiotensin II antagonist, is an effective and safe antihypertensive drug and appears to be tolerated especially well. Compared with the angiotensin converting enzyme inhibitor enalapril, losartan showed similar blood pressure-lowering efficacy evaluated at trough , whereas it was marginally less effective when all of the treated patients were analysed. However, in contrast to enalapril, losartan did not increase the incidence of dry coughing. Thus, losartan provides a promising new approach to treatment of hypertension. In the future, studies exploring effects of losartan on morbidity and mortality are needed to assess the long-term benefits of that angiotensin II antagonist as an antihypertensive agent. Acknowledgements We thank F. Mercier, statistician, for excellent assistance in statistical work. References 1. 2. 3. 4. 5. 6. 7. Duncia JV, Carini DJ, Chiu AT, Johnson AL, Pice WA, Wong PC, et a/.: The discovery of DuP 753, a potent, orally active nonpeptide angiotensin H receptor antagonist. Med Res Rev 1992, 12:149-191. Bernstein KE, Berk BC: The biology of angiotensin II receptors. Am ] Kidney Dis 1993, 22:745-754. Eberhardt RT, Kevak RM, Kang PM, Frishman WH: Angiotensin II receptor blockade: an innovative approach to cardiovascular pharmacology, J Clin Pharmacol 1993, 33:1023-1038. Timmermans PBMWM, Wong PC, Chiu AT, Herblin WF, Benfield P, Carini DJ, et al: Angiotensin II receptors and angiotensin II receptor antagonists. Pharmacol Rev 1993, 45:205-251. Gavras I: Bradykinin-rnediated effects of ACE inhition. Kidney Int 1992, 42:1020-1029. Dzau Vj, Mukoyama M, Pratt RE; Molecular biology of angio tensin receptors: target for drug research? J Hypertens 1994 12 (suppl 2):S1-S5. Husain A: The chymase-angiotensin system in humans. J Hypertens 1993, 11:1155-1159. Losartan versus enalapril in essential hypertension Tikkanen et al. 1351 8. Fletcher A E, Palmer AJ, Bulpitt CJ: Cough with angiotensin converting enzyme Inhibitors; how much of a problem? J Hypertens 1994, 12 (suppl 2):S43-S47. 9. Lacourciére Y, lefebvre J, Nakhle G, Faison EP, Snavely DB, Nelson EB: Association between cough and angiotensin converting enzyme inhibitors versus angiotensin II antagonists: the design of a prospective, controlled study. J Hypertens 1994, 12 (suppl 2):S49-S53. 10. lacourciére Y, Brunner H, Irwin R, Karlberg BE, Ramsay LE, Snavely DO, et al.: Effects of modulators of the renin-angiotensin-aldosterone system on cough. J Hyperions 1994, 12:1387-1393. 11. Os I, Bratland B, DahlÖf B, Gisholt K, Syvertsen J-Q, Tretli S: Lisinopril or nifedipine in essential hypertension? A Norwegian multicenter study on efficacy, tolerability, and quality of life in 828 patients, J Hypertens 1991, 9:1097-1104. 12. Todd PA, Heel RC: Enalapril, A review of its pharmacodynamic and pharmacokinetic properties, and therapeutic use in hypertension and heart failure. Drugs 1986, 31:198-248. 13. Johnston Cl: Angiotensin-converting enzyme inhibitors, in The Renin—Angiotensin System. Edited by Robertson JIS, Nicholls MG. London: Cower Medical Publishing; 1993:87.1-87.15. 14. Fletcher AE, Dollery CT: Side effects associated with inhibitors of angiotensin-converting enzyme. In The Renin-Angiotensin System. Edited by Robertson JIS, Nicholls MG. London: Cower Medical Publishing; 1993:99.1-99.4, 15. Sealey JE, Laragh JH: The reninn-angiotensin-aldosterone sys tem for normal regulation of blood pressure and sodium and potassium homeostasis. In Hypertension: Pathophysiology, Dia gnosis, and Management, Edited by Laragh JH, Brenner BM, New York: Raven Press: 1990:1287-1317. 16. Weber MA: Clinical experience with the angiotensin H receptor antagonist losartan; a preliminary report. Am J Hypertens 1992, 5:2475-251S. 17. Burnier M, Waeber B, Brunner HR: The advantages of angiotensin II antagonism. J Hypenens 1994, 12 (suppl 2);S7-S15. 18. Weber MA, Byyny RL, Pratt JH, Faison EP, Snavely DB, Gold berg A), el al,: Blood pressure effects of the angiotensin II receptor blocker, losartan. Arch Intern Med 1995, 155:405-411. 19. Tsunoda K, Abe K, Hagino T, Omata K, Misawa S, Imai Y, el al.: Hypotensive effect of losartan, a nonpeptide angioiensin II receptor antagonist, in essential hypertension. Am J Hypenens 1993, 6:28-32. 20. 21. 22. 23. DahlÖf B, Keller SE, Makris L, Goldberg Al, Sweet CS, Lim NY: Efficacy and tolerability of losartan potassium and atenolol in patients with mild to moderate hypertension. Am J Hypertens 1995, 8:576-583. Schoenberger JA for the Losartan Research Group: Losartan with hydrochlorothiazide in the treatment of hypertension. J Hypertens 1995, 13 (suppl 1};S43-S47. Goldberg Al, Dunlay MC, Sweet CS: Safety and tolerability of losartan potassium, an angiotensin II receptor antagonist, compared with hydrochlorothiazide, atenolol, felodipine ER, and angiotensin-converting enzyme inhibitors for the treatment of systemic hypertension. Am J Cardiol 1995, 75:793-795. Ilson B, Boike S, Larouche J, Freed M, Jorkasky D: The angiotensin II receptor antagonist SB 203220 does not increase uric acid (UA) excretion in healthy men [abstract]. J Am Soc Nephrol 1994, 5:562. Appendix The Scandinavian Study Group investigators are: Finland: T. Forslund, F. Fyhrquist, A. Halonen, J. Hämäläinen, P. Kivi, R. Lampen, A. Lehtniemi, I. Nikkari, H. Noronen, P. Saarinen, H. Säynäjoki, T. Silvennoinen, J. Silvo, T, Tikkanen, H. Ty Ö lahti, P. Vuojolahti. Denmark: P. Aarslev, J. Andersen, H.G. Bertelsen, M. Brahm, N. Borrild, R. Christensen, P. Duedal, T. Fredcriksen, O. Hansen, P.E. Heldgaard, T.E. Kristensen, T. Lassen, H.A. Lenler-Eriksen, O. Lindegaard, K. Moeller-Soerensen, S. Oegaard, J.E. Oestergaard, O. Oestergaard, J. Praest, O. Runesten, T. Sandager, H, Schmdt, P. Schultz-Larsen, F. Sorensen, P. Toft-Christensen, P. Vittrup, C. Voetmann, E. WendelEriksen. Iceland: A. Knstinsson. Norway: P.M. Chritensen, N. Espeland, R. Gundersen, G. Haugeberg, B.Helland, G. Hjorth, H Holmboc, H. Istad, K.L. Jacobsen, C. Lundbo, B. Ravlo, T Risanger, K. Sveen, T. Smedsrud, T. Thomassen, S. Vabo, P. Walvik.