Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Electrocardiography wikipedia , lookup
Heart failure wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Congenital heart defect wikipedia , lookup
Ventricular fibrillation wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
Atrial septal defect wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
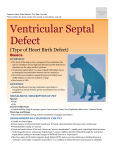
Review For reprint orders, please contact [email protected] Perventricular device closure of congenital muscular ventricular septal defects Expert Rev. Cardiovasc. Ther. 8(5), 663–674 (2010) Carlos AC Pedra†1,2, Simone RF Pedra1,2, Paulo Chaccur1,2, Marcelo Jatene1, Rodrigo N Costa1,2, Ziyad M Hijazi3 and Zahid Amin3 Instituto Dante Pazzanese de Cardiologia, Av. Dr Dante Pazzanese 500, 14 andar, CEP 04012-180, São Paulo, Brazil 2 Hospital do Coração da Associação Sanatório Sírio, R Desembargador Eliseu Guilherme, 147, CEP 04004-030, São Paulo, Brazil 3 Rush Center for Congenital and Structural Heart Disease, Rush University Medical Center, 1653, West Congress Parkway, 770 Jones, Chicago, IL 60612, USA † Author for correspondence: Tel.: +55 11 5085 6114 1 Fax: +55 11 5085 6196 [email protected] www.expert-reviews.com Muscular ventricular septal defects (MVSDs) account for approximately 20% of all congenital ventricular septal defects. Large defects in infants result in early heart failure, failure to thrive and pulmonary hypertension. Although percutaneous closure of MVSDs has been employed safely and effectively in children, adolescents and adults, its application in the small infant (weight <6 kg) carries a higher risk for complications including arrhythmias, hemodynamic compromise, cardiac perforation, tamponade and death. Perventricular closure of such defects, introduced by Amin and coworkers in the late 1990s, has become an attractive treatment modality for these small and high-risk patients. Experience worldwide has shown that the procedure is feasible, reproducible, safe and effective. In this article, the authors review the indications, the step-by-step technique and the results of perventricular closure of MVSDs using the AMPLATZER® mVSD device (AGA Medical, MN, USA). Keywords : AMPLATZER • hybrid • interventional catheterization • muscular ventricular septal defects • perventricular Muscular ventricular septal defects (MVSDs) account for approximately 20% of all congenital ventricular septal defects (VSDs) [1,2] . By definition, all rims of a MVSD are surrounded by muscular tissue within the interventricular septum (IVS) [1,2] . They can be located in the trabecular, apical or anterior region of the IVS [1,2] , and are usually distant from the atrioventricular node. When the defect is restrictive, the natural history usually shows spontaneous closure in most patients within the first 4–5 years of life [1,2] . Treatment is indicated when the defect results in heart failure in infancy or when there is volume overload of the left ventricle (LV) on echocardiography [1,2] . Worldwide experience has shown that percutaneous treatment of such defects is feasible, resulting in excellent outcomes in most patients from infancy to adulthood [3–12] . Complications are uncommon beyond infancy but may include embolization in an occasional adult patient in whom the septum might be too thick to accommodate the AMPLATZER® congenital mVSD device (AGA Medical, MN, USA) [13] . In addition, the application of this technique in the small infant (weight <5–6 kg) is associated with a higher risk for complications including hemodynamic compromise, arrhythmias, cardiac perforation, tamponade and death [5,10] . The concept 10.1586/ERC.10.31 of intraoperative closure of VSDs via a perventricular approach was introduced by Amin and coworkers in the late 1990s [14] . In this procedure, after a standard median sternotomy is performed by the surgical team, a delivery sheath is advanced through the anterior wall of the right ventricle (RV) across the defect into the LV. Under transesophageal echocardiographic (TEE) guidance, an intracardiac device is implanted through the delivery sheath by the interventionalist. Further publications documented its feasibility, reproducibility, safety and efficacy in this high-risk age group [15–21] . In this report, the authors will discuss the indications, the step-by-step technique and the results of perventricular closure of MVSDs. Anatomical classification of MVSDs for the interventionalist For the sake of ease and simplicity, the authors will describe a classification that is thought to be useful for the interventionalist. The IVS is a complex structure assuming an S-shape, separating the atrioventricular and semilunar valves. The muscular septum comprises most of the IVS and can be divided into three regions according to its right ventricular aspect (Figure 1) : trabecular, apical and anterior outlet septum. A trabecular © 2010 Expert Reviews Ltd ISSN 1477-9072 663 Review Pedra, Pedra, Chaccur et al. MVSD can extend into the inlet portion of the muscular IVS. This form is also called by some an inlet MVSD and should be differentiated from the true atrioventricular septal defect [22] . Apical defects are those located near the apex. The anterior outlet defects are the most uncommon and owing to their location, they can be challenging to cross with a guide wire using a perventricular approach. Most of the MVSDs are single and isolated lesions located in the mid portion of the trabecular IVS, the so-called mid-MVSDs. Sometimes the IVS looks like a sieve and has multiple muscular openings both in the left and right sides of the IVS. These defects are termed ‘Swiss cheese’ defects and may require multiple devices and repeat procedures for closure. Nevertheless, residual leaks are commonly seen after these multiple attempts. Indications of perventricular closure of MVSDs Perventricular closure is an alternative way of closing MVSDs using cardiac catheterization, echocardiographic and surgical techniques [22] . As such, this kind of hybrid procedure should SVC A P R 1 5 C NC M2 V 3 4 6 only be applied in special clinical scenarios. It is mainly indicated for the small infant weighing less than 5–6 kg with large and unrestrictive MVSDs, suffering from significant heart failure, pulmonary hypertension and failure to thrive [15–22] . In short, these patients are too fragile and not stable enough to undergo a long cardiac catheterization procedure. Vascular issues may also be a limiting factor. In addition, it has been shown that infants weighing less than 5–6 kg are at risk for complications during percutaneous closure of the MVSD [5,10] . On the other hand, one may consider undertaking the perventricular approach in infants a little bit larger than the threshold suggested earlier given the simplicity of perventricular closure and variations in policies at different institutions [21] . The patient with a hemodynamically significant MVSD associated with a concomitant condition that requires surgical repair, such as coarctation of the aorta, double-outlet RV, transposition of the great arteries and status post-pulmonary artery banding, may also benefit from the perventricular procedure [15–22] . In these patients, the MVSD can be closed using a perventricular approach through a median sternotomy and the associated defect can be surgically repaired at the same session in the operating room (OR). Avoidance of cardiopulmonary bypass (CPB) or limiting its time is a major advantage of the hybrid approach resulting in less morbidity, both in the short and long term, and faster recovery [23–29] . The patient with a small and restrictive MVSD, thriving well and without heart failure, should not undergo a per ventricular procedure. Spontaneous closure of such defects has been reported in most cases, usually in the first 5 years of life [1,2] . Closure of these defects with catheter, surgical or hybrid techniques on the basis of endocarditis prevention is highly debatable and not widely accepted [1,2] . MVSD devices IVC Figure 1. The interventricular septum from the right ventricular perspective. Encircled are the main locations of the muscular ventricular defects: (4) represents the trabecular mid-muscular defect; (6) represents the apical defects and (5) represents the anterior outlet defects. (1) represents the doubly committed or juxta arterial ventricular septal defects; (2) represents the perimembranous defect and (3) the inlet or atrioventricular type of ventricular septal defect. A: Aorta; C: Conal septum; IVC: Inferior vena cava; NC: Non-coronary cusp; P: Pulmonary trunk; R: Origin of the right coronary artery; SVC: Superior vena cava; V: Region of the AV node. 664 There are three devices available for MVSD closure: the CardioSEAL® (Nitinol Medical Technology, MA, USA), the Nit-Occlud® (Products fur Medizine, Germany) and the AMPLATZER mVSD. Because most, if not all, of the experience on perventricular closure of MVSDs was built using the AMPLATZER mVSD device and the authors are not familiar with the first two devices used in a perventricular approach, we will focus on this occluder. The AMPLATZER mVSD device (Figure 2) was designed specifically for closure of MVSDs. Of note, this device is approved for clinical use by the US FDA and by the Brazilian Expert Rev. Cardiovasc. Ther. 8(5), (2010) Perventricular device closure of congenital muscular ventricular septal defects National Health Vigilance Agency. It is made of a self-expanding Nitinol wire mesh woven into two discs connected by a 7-mm long cylindrical waist. Reinforced layers of polyester patches are sewn into the internal part of the Nitinol wire mesh to increase its occlusion rates. The device is malleable and has a shape memory owing to the properties of Nitinol. The size of the device is based on the diameter of the waist, which ranges from 4 to 18 mm in 2-mm increments. The discs are 8 mm larger than the connecting waist, except for the 4-mm device, in which the discs are 5 mm larger than the waist. Owing to the 7-mm separation between the two discs, the device seats well within the muscular defect, adjusted to the thickness and the motion of the IVS. As it happens with other AMPLATZER devices, the connecting waist has a stent-like effect on the edges of the defect and provides a self-centering mechanism, which helps to avoid prolapses during implantation and enhances closure rates. The device connects to the delivery cable by a female microscrew, located in the central portion of the right ventricular disc. The size of the delivery sheath required for implantation depends on the size of the device, ranging from 6–9 F. Because most MVSDs are oval in shape, a device that is approximately 2 mm larger than the largest end-diastolic diameter of the MVSD measured in at least two orthogonal echocardiographic views is selected for implantation [22] . Patients with severe pulmonary hypertension and/or with a deficient posteroinferior rim at the crux cordis may need some more oversizing (>3 mm than the largest diameter) to avoid prolapse and/or embolization [21] . The perventricular procedure Perventricular closure of MVSDs can be performed either in the OR (more common) or in a hybrid catheterization suite, if available. Regardless of the location chosen, it is crucial to have an experienced echocardiographer to monitor all steps of the procedure. A deep knowledge of the IVS anatomy, wire and catheter Review Figure 2. The AMPLATZER® (AGA Medical, MN, USA) muscular ventricular septal defects device. The device is made of a nitinol wire mesh forming two discs of the same size connected by a waist. manipulations, device delivery and deployment, and postrelease interrogation are all critical for procedural success and can only be accomplished by an experienced interventional echocardiographer. One must remember that in the operating room, the only imaging tool available to guide the whole procedure is the TEE. In less than ideal circumstances, epicardial echocardiography has also been used with good results. The procedure is performed under endotracheal general anesthesia. The size, location, proximity of valvular structures and number of defects are evaluated by TEE. After a median mini Figure 3. Median sternotomy and identification of the proper site to place the purse string suture. After median sternotomy is performed and the heart is secured in position in a pericardial cradle, surgical instruments (A) or the index finger (B) are used to gently push the right ventricular anterior free wall in order to identify the best location for placement of the purse string suture. The bulging on the anterior right ventricular free wall and its relation to the interventricular septum and the muscular ventricular septal defect are defined by transesophageal echocardiogram. www.expert-reviews.com 665 Review Pedra, Pedra, Chaccur et al. Figure 4. Transeophageal echocardiographic monitoring during perventricular closure of the muscular ventricular septal defect. Four-chamber view. (A) Single muscular ventricular septal defect located in the mid-trabecular area of the septum measuring 9–10 mm. (B) The distance between the anterior right ventricular free wall and the posterior left ventricular wall is measured (35 mm). (C) Internal bulging of the anterior right ventricular free wall after it is gently pushed using the index finger. (D) A J-tip 0.038-inch echogenic guide wire is seen across the defect into the left ventricle. or standard sternotomy is performed, the heart is secured in a pericardial cradle. Heparin sulfate is given (100 IU/kg) and prophylactic antibiotics are used according to local protocols. Under TEE guidance, the best location for needle puncture and sheath entry through the free wall of the RV is identified (F igures 3 & 4) . This is accomplished by gently pushing the anterior free wall of the RV using the index finger just opposite to the MVSD location, keeping a straight line and a perpendicular angle to the IVS (Figures 3 & 4) . A purse string suture is placed on this site. A 17–20-gauge needle (angiocath or metal) is inserted through the purse string suture into the RV cavity (Figure 5) . A Terumo glide wire or, preferably, a regular 0.038-inch J-tip wire (available in the standard short sheath box set) is maneuvered across the MVSD into the LV (Figures 4 & 5) . The regular J-tip 666 wire is usually easier to track by TEE since it is more echogenic than the Terumo wire. In addition, it rarely passes across the trabeculation of the RV owing to its J-tip. Once the wire is identified in the LV cavity, the needle is removed leaving sufficient amounts of wire in the LV. Some advocate predilating the RV free wall using a dilator that is 1 F larger than the sheath that is being planned to be used for deployment, although this is not mandatory [22] . In order to avoid inadvertent trauma to the posterior LV wall, the selected standard short sheath is premarked using a cotton suture (Figure 6) . The distances between the anterior RV wall and the free LV cavity and the posterior LV wall are measured by TEE using the four-chamber view (F igure 4) . The distance between the free cavity of the LV (where the tip of the sheath should be positioned) and the anterior RV Expert Rev. Cardiovasc. Ther. 8(5), (2010) Perventricular device closure of congenital muscular ventricular septal defects Review Figure 5. Purse string suture and puncture of the right ventricular free wall. (A) A purse string suture is placed on the right ventricular free wall by the surgeon. (B) A metallic needle is inserted through the right ventricular wall and a J-tip guide wire is advanced through the needle across the ventricular septal defect. wall (where the suture should be secured on the sheath) is then used as a reference for marking the sheath. The appropriate sized and marked short sheath is then advanced over the wire into the LV. A useful tip is to slide the sheath over the dilator and the guide wire once the dilator is approximately 1–2 cm past the anterior wall of the RV. Even premarking the delivery sheath, it is crucial to recognize the tip of the dilator and the sheath on TEE to prevent injuries to the posterior wall of the LV (Figure 7) . Flushing the sheath with saline is also helpful to verify where it is. An appropriate sized device is loaded either in the standard plastic loader that is enclosed in the delivery system package or in another short sheath with the same profile as the one left across the MVSD. The loader or the loading sheath is advanced through the hemostatic valve of the short sheath positioned across the MVSD and the delivery cable is pushed gently (F igure 6) . In order to ensure a smooth transition of the device from the loader to the short sheath, it is helpful to have a second pair of hands securing the short sheath in place in the RV wall. Once the device is transferred to the short sheath, the loader is removed. Under TEE guidance and in the beating heart, the delivery cable is slowly advanced in order to deploy the LV disc in the middle of the LV free cavity. TEE pictures must leave no doubts with regards to the location of the LV disc. It should be clearly seen inside the free LV cavity (Figure 7) . Special attention must be taken to ensure that there is no entanglement within the mitral valve apparatus. A slow and gentle pull on the short sheath exposes the connecting waist (Figure 7) . After this is confirmed by TEE, the whole system is brought back as a unit until the waist is seen within the MVSD itself and the LV disc is seen abutting the IVS on the left side (Figure 7) . The right disc is then delivered by very slowly and gently pulling back the sheath and advancing the delivery cable (two-hand Figure 6. Sheath positioning across the right ventricular free wall. (A) An 8 F standard short sheath is positioned through the right ventricular free wall. Note the suture on the sheath abutting the right ventricular wall. (B) After the device is transferred from the loader to the short sheath, implantation is performed with gentle movements, pulling on the sheath and pushing on the delivery cable. www.expert-reviews.com 667 Review Pedra, Pedra, Chaccur et al. Figure 7. Transeophageal echocardiographic monitoring during implantation. Four-chamber view. (A) The short 8 F sheath is seen across the defect. The tip is located in the mid-left ventricular cavity, away from the posterior wall. (B) The left disc and the waist of a 12‑mm device are deployed in the mid-left ventricular cavity. (C) The left disc is approaching the interventricular septum. (D) Adequate device positioning within the septum. technique). This delicate maneuver is of paramount importance since there is not much room in the RV to deploy the RV disc. Device position, possible interference with the function of the atrioventricular and semilunar valves, and residual leaks are then assessed by TEE (Figure 7) . Once the operators are sure that the device seats properly within the IVS with no impingement on any important cardiac structure, the device is released by rotating the delivery cable in a counterclockwise fashion. After device release, the delivery cable is withdrawn followed by the short delivery sheath. The purse string suture is tied, heparin is partially neutralized using protamine sulfate based on the activated coagulation time results and the chest is closed in a standard fashion. Pericardial drains, chest tubes and epicardial leads are not commonly left in place after a straightforward procedure to close an isolated MVSD. 668 In the case of an associated coarctation ���������������������������������� of the aorta���������� or a previously placed pulmonary artery banding, the lesions are subsequently repaired without the need of CPB. In the case of a complex congenital heart disease with unusual orientation of the IVS such as double-outlet RV or transposition of great arteries with an additional MVSD, the underlying condition is repaired surgically after the MVSD is device closed with this technique, sparing some precious time of CPB. Troubleshooting: adjusting & customizing the technique For apical defects, it is easier to cross the defect from a purse string suture placed near the apex. However, using this approach it may be more difficult (or even impossible) to deploy the right disc inside the right ventricular cavity owing to lack of space. In this Expert Rev. Cardiovasc. Ther. 8(5), (2010) Perventricular device closure of congenital muscular ventricular septal defects Review case, the right disc must be deployed very slowly (over 30 s) so as to give it ample time to reconfigure its shape as close to the IVS as possible [22] . If this does not work and the female end of the microscrew and part of the right disc protrudes out of the apical RV free wall, this part of the device should be secured to the RV wall using standard stitches and sutures (Figure 8) . Although this may not seem cosmetically adequate, it has not caused any clinical problems thus far. An AMPLATZER Duct Occluder (AGA Medical), with no disc on the right side may also be used in this setting. Another option to deal with apical defects is to place the purse string suture not at the apex but towards the mid portion of the anterior free wall of the RV [22] . One can use a bent needle to cross the defect, and a curved braided short sheath and dilator to reach the LV. The sheath is advanced through the RV free wall at an angle as if the defect was being closed Figure 8. The female microscrew and part of the right disc is seen protruding out from the internal jugular vein. Maneuvers to of the apical right ventricular wall. The device was secured in place using standard avoid device prolapse towards the RV while stitches and suture material. The delivery cable is still attached to the microscrew. deploying the device should be taken using this approach. out from the short sheath positioned in the free RV wall. Over We have not encountered a case in which a mid-muscular this wire, the delivery sheath is advanced and the procedure or an apical defect could not be crossed with a guide wire [22] . completed [30] . Occasionally, it may be difficult to cross an anterior defect comFor extremely large defects (>14 mm), especially when there is ing from the RV free wall. In such cases, a ‘true’ hybrid approach a deficient posteroinferior rim towards the crux cordis (Figure 9) may be employed to deal with the problem [30] . With the aid of and associated pulmonary hypertension, it may be necessary to angiography and fluoroscopy in a hybrid suite or using a portable oversize the device a little more than 2 mm in order to avoid C-arm in the OR, a catheter is positioned percutaneously in the device prolapse or embolization. Another option is to secure the LV and the defect is crossed retrogradely with a guide wire. The device in place by placing a stitch through the RV wall catching wire is then snared in the pulmonary artery and exteriorized the edge of the deployed RV disc (Figure 10) [21] . Figure 9. Transesophageal echocardiography in a modified gastric view. (A) Large mid-muscular ventricular septal defect with apical extension and a deficient posteroinferior rim. (B) Large (15-mm) muscular ventricular septal defect located in the mid-to-apical portion of the interventricular septum in a 2-year-old female patient previously submitted to pulmonary artery banding. The postero‑inferior rim of the defect is deficient. www.expert-reviews.com 669 Review Pedra, Pedra, Chaccur et al. Figure 10. Transesophageal echocardiography in a modified gastric view (same patient as in Figure 9 ). (A) Prolapse of the inferior portion of the left disc of a 16 mm device through the deficient part of the septum. (B) After the sheath was slightly reoriented, the device was correctly deployed and subsequently secured in place with stitches placed across the right ventricular wall catching the edge of the right ventricular disc. Color Doppler interrogation shows complete occlusion and no interference with the atrioventricular valve function. In the case of multiple defects, each defect is approached in a standard fashion using the previously described techniques. It may be wiser to start closing the more apical defect first to leave more room to deploy a second or even a third device higher up in the middle of the RV cavity. Because the sheath usually crosses the VSD in a perpendicular fashion, it is uncommon to pull the device through the defect using the perventricular approach. If the device is undersized, it obviously needs to be replaced. Deploying the waist in the LV cavity helps to align the LV disc to the plane of the LV septum, preventing the edge of the disc from protruding into the defect [22] . If the defect is large and the posteroinferior rim at the crux cordis is somewhat deficient (Figures 9 & 10) , one may need to slightly change the orientation of the sheath in order to bring the device in a more parallel fashion towards the IVS. Securing the device in place with a suture as described previously may also be helpful in such cases. Entanglement of the left disc within the mitral valve apparatus may occur during the procedure. It should be avoided by deploying the LV disc closer to the IVS and performing meticulous TEE. If there is any difficulty bringing the left disc and the delivery sheath back towards the IVS and the LV disc does seem to be entangled within the mitral valve apparatus on TEE, one should carefully advance the sheath and the device deep in the LV and recapture the LV disc [22] . Sometimes, both discs have to be deployed in the LV to untangle the device from the mitral valve chordae [22] . If these maneuvers do not work, surgical removal should be undertaken to prevent damage to the mitral valve apparatus. Figure 11. Chest radiograph pre- and postprocedure. (A) Enlarged cardiac silhouette and increased pulmonary vascular markings are conspicuous. (B) On the first postoperative day there was a remarkable decrease in the size of the heart and improvement in the lung fields. The implanted device is seen in the left lower portion of the cardiac silhouette. 670 Expert Rev. Cardiovasc. Ther. 8(5), (2010) Embolization is a rare event using a perventricular approach. It is probably associated with inadequate device selection and/or unrecognized device malposition prior to release. The operators must identify where the embolized device is stuck. Because patients undergoing perventricular closure of MVSDs are small, device retrieval using percutaneous or perventricular techniques are usually not feasible and may carry a higher risk than expected. Surgical retrieval of the device followed by patch closure of the MVSD should generally be undertaken. In the rare event of failure to close the defect using a perventricular approach, the patient can still undergo standard surgical patch closure of the MVSD under CPB or have a band placed around the main pulmonary artery. Follow-up The patient is usually extubated in the first hours after the procedure and is routinely monitored in the intensive care unit for 24–48 h. Inotropic support is rarely required. A transthoracic echocardiogram is performed the following day to assess device position, residual leaks and pericardial effusion. Patients are typically discharged 3–7 days after an uneventful procedure with remarkable improvement in their clinical conditions (Figure 11) . Aspirin is usually given a couple of days prior to the procedure (3–5 mg/kg/day) and maintained for 6 months. Bacterial endocarditis prophylaxis is recommended for 6 months or indefinitely if there is residual shunting persisting for over 1–2 years. Clinical visits and serial transthoracic echocardiograms are scheduled for 1, 3, 6 and 12 months after the procedure and yearly after. Although debatable, repeat Holter monitoring is advocated by some in order to detect subclinical conduction abnormalities. Results Because large MVSDs in small infants are not commonly encountered in clinical practice, most of the experiences of perventricular closure of such defects reported in the literature are based on small cohorts of patients [15–21] . As such, it seems prudent for low-volume institutions to refer these cases to institutions that are better versed with this procedure [22] . Even being a relatively new and uncommon procedure, with information based on a limited number of patients in the literature, the perventricular closure of MVSDs seems to be feasible and reproducible in different hands, safe and highly effective. The technical success rate of the perventricular approach should approach 100% in the hands of interventional and surgical teams experienced in treating congenital heart diseases. Complication rates should decrease with accumulation of experience [22] . The risk of device embolization should be minimized by state-ofthe-art use of TEE techniques and optimal device selection and positioning. Cardiac perforation should be avoided by careful and meticulous technique. Blood loss requiring transfusion may be an issue in these small and already fragile patients. Pericardial effusion and tamponade may occur, usually due to catheter injury of the LV posterior free wall, which is minimized with judicious techniques. It is speculated that late LV aneurysm formation may www.expert-reviews.com Review Figure 12. Echocardiographic views of a large mid-muscular ventricular septal defect with apical extension and a deficient posteroinferior rim. (A) Modified fourchamber view on transesophageal echocardiography before device implantation showing a large (14–15‑mm) defect. (B) Same modified four-chamber view on transesophageal echocardiography immediately after device implantation. A 16‑mm device is in good position with no prolapse towards the right ventricle. (C) Subxiphoid view on a transthoracic echocardiogram performed 1 week after implantation showing prolapse of the left posteroinferior portion of the device towards the right ventricle (arrow). Perventricular device closure of congenital muscular ventricular septal defects 671 Review Pedra, Pedra, Chaccur et al. be due to injury in the posterior LV wall during the procedure [31] . Interference with the function of the atrioventricular valves is uncommon but may occur when the trabecular defect extends towards the inlet septum. Interference with the function of the semilunar valves has not been described. Device-related hemolysis is rare and only occurs when a high-velocity residual leak is encountered at the edge of the device. Conservative management over a couple of days may be sufficient to treat this complication. Some advocate soaking the device in the patient’s own blood to enhance the immediate occlusion rate and prevent hemolysis [22] . Conduction abnormalities are relatively uncommon. A right or a left bundle branch block pattern may occasionally be encountered but usually has a benign course [32] . Complete heart block is rare and should prompt device removal when it occurs within the first hours or days after implantation. It is possible that the inlet type of muscular defect is at a higher risk for this complication [21] . Late heart block has not been described. The risk of death should be related to the patient’s comorbid condition rather than to the procedure itself. Closure rates are high. For the isolated and single MVSD, occlusion rates should approach 100% [15–21] . Residual leaks may be seen in multiple defects in which multiple devices have been used. However, most of these leaks are small and do not require further interventions, especially when the indexed left ventricular end-diastolic dimension for body surface area returns to normal (or near normal) values. In a multicenter experience in South America, from July 2007 to May 2009, nine non-consecutive patients (median age and weight 6 months and 5.5 kg, respectively) underwent the procedure in the OR under TEE guidance using AMPLATZER devices [21] . All patients but one were in congestive heart failure and had pulmonary arterial hypertension. One patient was status post-pulmonary artery banding and three also had coarctation of the aorta, which were all repaired at the same session. Eight patients had single MVSDs (six mid-muscular, two apical) measuring 10.3 ± 3.7 mm and one patient had multiple apical defects that required two devices. Ten devices were implanted successfully (median size: 12 mm), with two having to be secured in the RV wall with a surgical suture. One patient each developed right and left bundle branch block. In one patient with a 14-mm defect, the inferior portion of a 16-mm device prolapsed through the posteroinferior rim of the defect towards the RV (Figure 12) , requiring surgical removal with patch closure of the mid-MVSD. In retrospect, a larger device or fixation in the right ventricular wall should have been employed to avoid prolapse in this case. After a median follow-up of 1 year, all eight remaining patients, including the one with two devices, had complete closure of the defects with normal LV. The authors went on to conclude that perventricular closure of MVSDs seemed to be reproducible, feasible, relatively safe and effective in their hands. However, large defects may need device oversizing or suture fixation for adequate stabilization. In the largest personal experience encountered, Amin has performed 54 cases with a technical success rate of initial device implantation of 100% [Pedra CAC, Pers. Comm.] . However, some failures and complications were observed. In one patient with two defects, the second defect could not be crossed after one device had already been placed. One patient developed complete heart block within a few hours of the procedure and required a pacemaker. This patient had a high inlet MVSD. One patient had device embolization to the LV requiring surgical removal. This patient had prolonged PA banding with severe RV hypertrophy and pulmonary hypertension. We believe that the defect measurement was inadequate and underestimated at the time of the procedure. The VSD size increased as the RV hypertrophy regressed. One patient had elective device removal owing to hemolysis 5 days after the procedure. The remainder of the patients have had a follow-up ranging from 4 months to 10 years with excellent results. Expert commentary Device closure of MVSDs has significantly evolved over the last years and perventricular closure of MVSDs has emerged as the modality of choice to manage the small infant with a large defect. It enables a direct route to close the defect, minimizing the chances of hemodynamic compromise that usually occurs with the percutaneous technique in the catheterization laboratory. Because it avoids CPB, the morbidity is limited and recovery time is optimized. In addition, it is associated with high occlusion rates and consistent outcomes that persist in the mid-term follow-up. Key issues • Large muscular ventricular septal defects (MVSDs) can result in heart failure, pulmonary hypertension and failure to thrive in small infants. • Surgical closure of such defects can be challenging owing to the heavily trabeculated right ventricle and may be associated with significant morbidity, including residual shunting and the adverse effects of cardiopulmonary bypass. • Percutaneous closure of MVSDs can be performed safely and effectively in children and adolescents. In adults, there might be a slightly higher risk of embolization owing to the thickness of the interventricular septum. However, small infants (weight <5–6 kg) are at a higher risk for severe complications including hemodynamic compromise, arrhythmias, cardiac perforation, tamponade and death, and remain a challenging subset of patients. • Perventricular device closure of the MVSD in the beating heart has emerged as an excellent alternative to manage such fragile and high-risk patients. Clinical experience, albeit still limited, has demonstrated that the procedure is feasible and reproducible in different hands, safe and highly effective. • Further refinements in the technique are likely to improve the overall results, further decreasing an already remarkably low morbidity rate. 672 Expert Rev. Cardiovasc. Ther. 8(5), (2010) Perventricular device closure of congenital muscular ventricular septal defects Five-year view Miniaturized probes to perform real-time 3D TEE will probably be available in the near future. This might contribute to a better understanding of the anatomy of the IVS, the multiple defects and those that are large with a deficient posteroinferior rim at the crux cordis. A shorter, curved and braided AMPLATZER TorqVue ® (AGA Medical) delivery sheath, and a shorter and more flexible delivery cable (with Nitinol extension at the distal extremity) will probably be used for perventricular device closure of large MVSDs in small infants in the near future. Limiting (or even eliminating?) surgical scar and the extension of the median sternotomy will also be part of the next challenges to References 7 Papers of special note have been highlighted as: • of interest •• of considerable interest 1 2 3 4 5 6 Tynan M, Anderson RH. Ventricular septal defect. In: Paediatric Cardiology. Anderson RH, Baker EJ, Macartney FJ, Rigby ML, Shinebourne EA, Tynan M (Eds). Churchill Livingstone, London, UK, 983–1014 (2002). Kouchoukos NT, Blackstone EH, Doty DB, Hanley FL, Karp RB. Ventricular septal defect. In: Kirklin/ Barratt-Boyes Cardiac Surgery. Kouchoukos NT, Blackstone EH, Doty DB, Hanley FL, Karp RB (Eds). Churchill Livingstone, PA, USA, 850–910 (2003). Thanopoulos BD, Tsaousis GS, Konstadopoulou GN, Zarayelyan AG. Transcatheter closure of muscular ventricular septal defects with the AMPLATZER ventricular septal defect occluder: initial clinical applications in children. J. Am. Coll. Cardiol. 33(5), 1395–1399 (1999). Hijazi ZM, Hakim F, Al-Fadley F, Abdelhamid J, Cao QL. Transcatheter closure of single muscular ventricular septal defects using the AMPLATZER muscular VSD occluder: initial results and technical considerations. Catheter. Cardiovasc. Interv. 49(2), 167–172 (2000). Holzer R, Balzer D, Cao QL, Lock K, Hijazi ZM. Device closure of muscular ventricular septal defects using the AMPLATZER muscular ventricular septal defect occluder: immediate and mid-term results of a U.S. registry. J. Am. Coll. Cardiol. 43(7), 1257–1263 (2004). Arora R, Trehan V, Thakur AK, Mehta V, Sengupta PP, Nigam M. Transcatheter closure of congenital muscular ventricular septal defect. J. Interv. Cardiol. 17(2), 109–115 (2004). www.expert-reviews.com 8 9 improve the overall results of the procedure in the upcoming years. Reabsorbable devices will not be part of clinical practice in the next 5 years but might be in the next decade. Financial & competing interests disclosure Carlos AC Pedra and Zahid Amin are consultants and on the speakers’ bureau for AGA Medical (MN, USA). The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed. No writing assistance was utilized in the production of this manuscript. Thanopoulos BD, Rigby ML. Outcome of transcatheter closure of muscular ventricular septal defects with the AMPLATZER ventricular septal defect occluder. Heart 91(4), 513–516 (2005). Carminati M, Butera G, Chessa M, Drago M, Negura D, Piazza L. Transcatheter closure of congenital ventricular septal defect with AMPLATZER septal occluders. Am. J. Cardiol. 96, 52L–58L (2005). Djer MM, Latiff HA, Alwi M, Samion H, Kandavello G. Transcatheter closure of muscular ventricular septal defect using the AMPLATZER devices. Heart Lung Circ. 15(1), 12–17 (2006). 10 Diab KA, Cao QL, Mora BN, Hijazi ZM. Device closure of muscular ventricular septal defects in infants less than one year of age using the AMPLATZER devices: feasibility and outcome. Catheter. Cardiovasc. Interv. 70(1), 90–97 (2007). 11 Queiroz FJ, Rossi Filho RI, Ramos S et al. Percutaneous occlusion of interventricular septal defects. Initial experiment. Arq. Bras. Cardiol. 85(3), 174–179 (2005). 12 Pedra CAC, Pedra SRF, Pessotti C et al. Percutaneous closure of congenital muscular ventricular septal defects. Rev. Bras. Cardiol. Inv. 16(2), 218–224 (2008). 13 Bialkowski J, Szkutnik M, Kusa J, Fiszer R. Few comments regarding transcatheter closure of congenital perimembranous and muscular ventricular septal defects. Int. J. Cardiol. DOI: 10.1016/j. ijcard.2009.04.029 (2009) (Epub ahead of print). 14 Review Amin Z, Berry JM, Foker JE, Rocchini AP, Bass JL. Intraoperative closure of muscular ventricular septal defect in a canine model and application of the technique in a baby. J. Thorac. Cardiovasc. Surg. 115, 1374–1376 (1998). •• First paper to report the concept of perventricular device implantation. 15 Bacha EA, Cao QL, Starr JP, Waight D, Ebeid MR, Hijazi ZM. Perventricular device closure of muscular ventricular septal defects on the beating heart: technique and results. J. Thorac. Cardiovasc. Surg. 126, 1718–1723 (2003). 16 Bacha EA, Cao QL, Galantowicz ME et al. Multicenter experience with perventricular device closure of muscular ventricular septal defects. Pediatr. Cardiol. 26(2), 169–175 (2005). •• First multicenter study reporting consistent results of perventricular closure of muscular ventricular septal defects. 17 Gan C, Lin K, An Q et al. Perventricular device closure of muscular ventricular septal defects on beating hearts: initial experience in eight children. J. Thorac. Cardiovasc. Surg. 137(4), 929–933 (2009). • Results of a center in China confirming the reproducibility of the method. 18 Crossland DS, Wilkinson JL, Cochrane AD, d’Udekem Y, Brizard CP, Lane GK. Initial results of primary device closure of large muscular ventricular septal defects in early infancy using perventricular access. Catheter. Cardiovasc. Interv. 72(3), 386–391 (2008). • Results of a center in Australia confirming the reproducibility of the method. 19 Celiker A, Ozkutlu S, Erdoğan I, Karagöz T, Doğan OF, Demircin M. Perventricular closure of muscular ventricular septal defect in an infant. Anadolu. Kardiyol. Derg. 8(4), 312–313 (2008). 20 Becker P, Frangini P, Heusser F, Urcelay G, Garay F. New surgical approach to device closure of multiple apical ventricular septal defects. Rev. Esp. Cardiol. 57(12), 1238–1240 (2004). 673 Review 21 • 22 Pedra, Pedra, Chaccur et al. Pedra CAC, Pedra SRF, Chaccur P et al. Perventricular closure of congenital muscular ventricular septal defect: multicenter experience in South America. Rev. Bras. Cardiol. Invs. 17(3), 386–397 (2009). Results of a multicenter study in South America confirming the reproducibility of the method. Interesting review on percutaneous and perventricular closure of muscular ventricular septal defects. 23 Serraf A, Lacour-Gayet F, Bruniaux J et al. Surgical management of isolated multiple ventricular septal defects. Logical approach in 130 patients. J. Thorac. Cardiovasc. Surg. 103, 437–442 (1992). Kitagawa T, Durham LA III, Mosca RS, Bove EL. Techniques and results in the management of multiple 674 29 Hovels-Gurish HH, Konrad K, Skorzenski D et al. Long-term behavior and quality of life after corrective cardiac surgery in infancy for tetralogy of fallot or ventricular septal defect. Pediatr. Cardiol. 28(5), 346–354 (2007). 25 Hanna B, Colan SD, Bridges ND, Mayer JE, Castaneda AR. Clinical and myocardial status after left ventriculotomy for ventricular septal defect closure. J. Am. Coll. Cardiol. 17(Suppl.), 110A (1991). 30 26 Wollenek G, Wyse R, Sullivan I, Elliot M, de Leval M, Stark J. Closure of muscular septal defects through a left ventriculotomy. Eur. J. Cardiothorac. Surg. 10, 595–598 (1996). Diab KA, Hijazi ZM, Cao QL, Bacha EA. A truly hybrid approach to perventricular closure of multiple muscular ventricular septal defects. J. Thorac. Cardiovasc. Surg. 130(3), 892–893 (2005). 31 27 Kaltman JR, Javik GP, Bernabaum J et al. Neurodevelopmental outcome after early repair of a ventricular septal defect with or without aortic arch obstruction. J. Thorac. Cardiovasc. Surg. 131(4), 792–798 (2006). Breinholt JP, Rodefeld MD, Hoyer MH. Successful embolization of a left ventricular pseudoaneurysm after perventricular ventricular septal defect device closure. Catheter. Cardiovasc. Interv. 74(4), 624–626 (2009). 32 28 Hovels-Gurish HH, Konrad K, Skorzenski D, Herpertz-Dahlmann B, Messmer BJ, Seghaye MC. Attentional dysfunction in children after corrective cardiac surgery in infancy. Ann. Thorac. Surg. 83(4), 1425–1430 (2007). Robinson JD, Zimmerman FJ, De Loera O, Heitschmidt M, Hijazi ZM. Cardiac conduction disturbances seen after transcatheter device closure of muscular ventricular septal defects with the AMPLATZER occluder. Am. J. Cardiol. 97(4), 558–560 (2006). Amin Z, Cao QL, Hijazi ZM. Closure of muscular ventricular septal defects: transcatheter and hybrid techniques. Catheter. Cardiovasc. Interv. 72, 102–111 (2008). • 24 ventricular septal defects. J. Thorac. Cardiovasc. Surg. 115, 848–856 (1998). Expert Rev. Cardiovasc. Ther. 8(5), (2010)