Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Heart failure wikipedia , lookup
Coronary artery disease wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Myocardial infarction wikipedia , lookup
Electrocardiography wikipedia , lookup
Atrial fibrillation wikipedia , lookup
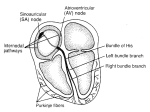
Drugs for Dysrhythmias Expanded Key Concepts 23.1 The frequency of dysrhythmias in the population is difficult to predict because many patients experience no symptoms. Persistent or severe dysrhythmias may be lethal. Some dysrhythmias produce no symptoms and are harmless, while others are life threatening. The frequency of dysrhythmias is difficult to predict, although it is thought to be quite common, particularly in the geriatric population. 23.2 Dysrhythmias are classified by the location (atrial or ventricular) or type (flutter, fibrillation and block) of rhythm abnormality produced. There are many types of dysrhythmias and the simplest method of classification is to name them according to the type of rhythm abnormality produced and its location. Dysrhythmias are associated with other diseases such as hypertension, CAD and heart failure. 23.3 The electrical conduction pathway from the SA node to the AV node to the bundle branches and Purkinje fibers keeps the heart beating in a synchronized manner. Some myocardial cells in these regions have the property of automaticity. The normal rhythm of the heart is established by the SA node, which ensures the chambers beat in a synchronized manner. The central problem of dysrhythmia is the potential to affect the function of the heart. It can manifest itself as a reduction in cardiac output and can cause certain consequences such as stroke or congestive heart failure. 23.4 The electrophysiologic events in the heart can be measured with an electrocardiograph. The ECG depicts electrical events occurring in the heart. It can assess timing or changes to the wave patterns. It is also used to diagnose dysrhythmias and other cardiac pathologies. 23.5 Changes in sodium and potassium levels generate the action potential in myocardial cells. Depolarization occurs when sodium and calcium rush in; repolarization occurs when potassium is removed. An action potential begins when sodium ion channels located in the plasma membrane open and Na+ rushes into the cell producing a rapid depolarization. During this period, Ca++ also enters the cell through calcium ion channels, although the influx is slower than that of sodium. The cell returns to its polarized state by the removal of K+ through potassium ion channels. 23.6 Non-pharmacologic therapy of dysrhythmias including cardioversion, ablation, and implantable cardioverter defibrillators are often the treatments of choice. Because of their potential to cause serious side effects, antidysrhythmic drugs are normally reserved for those patients experiencing overt symptoms or for those whose condition cannot be controlled by other means. Non-pharmacologic treatment is often preferred over drug therapy. 23.7 Antidysrhythmic drugs are classified by their mechanism of action, Class I -- IV. Antidysrhythmic drugs affect the action potential in myocardial cells and act by blocking sodium, potassium or calcium channels in the cell membrane. Most antidysrhythmic drugs are placed into one of five classes based on their mechanism of action. Class I agents are further subdivided into IA, IB, and IC. Agents within the same class have similar actions and adverse effects. 23.8 Sodium channel blockers are the largest group of antidysrhythmics and act by slowing the rate of impulse conduction across the heart. Sodium channel blockers stabilize dysrhythmias by slowing the spread of impulse conduction across the myocardium. Quinidine, a class IA agent, is the oldest antidysrhythmic drug. 23.9 Beta-adrenergic blockers act by reducing automaticity as well as slowing conduction velocity across the myocardium. Beta-adrenergic blockers are widely used for cardiovascular disorders. Their ability to slow the heart rate and conduction velocity can suppress several types of dysrhythmias. The main value of beta-blockers as antidysrhythmic agents is to treat atrial dysrhythmias associated with heart failure. 23.10 Potassium channel blockers prolong the refractory period of the heart. A potassium channel blocker, such as amiodarone, can stabilize dysrhythmia by prolonging the duration of the action potential and extending the refractory period. Drugs in this class generally have restricted uses due to potentially serious side effects. 23.11 The calcium channel blockers act by reducing automaticity and by slowing myocardial conduction velocity. Their actions and effects are similar to the beta-blockers. The calcium channel blocker, verapamil, reduces automaticity in the SA node, slows impulse conduction through the AV node, and prolongs the refractory period. Only a few drugs in this class are approved for dysrhythmias. 23.12 Digoxin, adenosine, and ibutilide are used for specific dysrhythmias but do not act by blocking ion channels. Several other medications are occasionally used to treat specific dysrhythmias, but do not act by the mechanisms of Class I, II, III or IV drugs. Digoxin is prescribed for certain types of atrial dysrhythmias because of its ability to decrease automaticity of the SA node and slow conduction through the AV node. Adenosine and ibutilide are used for the short-term, rapid termination of dysrhythmias.