Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
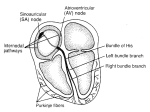
Nursing 202 – Notes on Dysrhythmia Medications 1. Some dysrhythmias produce no patient symptoms, while others may be life threatening. Some dysrhythmias are asymptomatic, while others require immediate treatment. The frequency of dysrhythmias is common, particularly in the geriatric population. HF and MI are associated with an increased risk of dysrhythmias. 2. The phases of the cardiac action potential include rapid depolarization, a long plateau, and repolarization. The cardiac action potential involves an electrical impulse generated and transmitted due to depolarization and repolarization of the cell membrane. During these phases sodium, potassium, or calcium channels open and close in the cell membrane. 3. The electrocardiogram (ECG) is used to measure electrical conduction across the myocardium. The ECG contains three waves of importance to the diagnosis of heart disease: the P wave, the QRS complex, and the T wave. Changes to the waves or in their timing suggest certain pathologies. Antidysrhythmic drugs affect the ECG. 4. Dysrhythmias are classified by the impulse origin and type of rhythm abnormality produced. Dysrhythmias are classified by their site of origin, either atrial or ventricular, and by the type of rhythm abnormality produced such as tachycardia, bradycardia, flutter, or fibrillation. 5. Antidysrhythmic drugs inhibit abnormal pathways of electrical conduction and are only used when there is a clear benefit to the patient. Antidysrhythmic agents have the ability to create new rhythm abnormalities or worsen existing ones. Because of this, there must be a clear benefit to the patient before initiating pharmacotherapy. Nonpharmacological treatment such as cardioversion or catheter ablation is often preferred over drug therapy. 6. Antidysrhythmic drugs are classified by their mechanism of action. Most antidysrhythmic drugs are placed into one of five classes, based on their mechanism of action. Class I agents are further subdivided into IA (Procainamide), IB (Lidocaine), and IC (Flecainide). Agents within the same class have similar actions and adverse effects. 7. Class I antidysrhythmics act by blocking sodium ion channels in myocardial cells. Sodium channel blockers stabilize dysrhythmias by slowing the spread of impulse conduction across the myocardium. They are used to treat both atrial and ventricular dysrhythmias. Drugs in this class are subdivided into class IA, IB, and IC. All the class I drugs can worsen or create new dysrhythmias. 8. Class II Beta-adrenergic antagonists reduce automaticity as well as slow conduction velocity in the heart. Beta-blockers stabilize dysrhythmias by slowing the heart rate and decreasing the conduction velocity through the AV node. As antidysrhythmic agents the main indication for of beta blockers is to treat atrial dysrhythmias associated with heart failure. Tachydysrhythmias respond well to beta blockers. 9. Class III Potassium channel blockers prolong the refractory period of the heart. Potassium channel blockers stabilize dysrhythmias by prolonging the duration of the action potential and extending the refractory period. Potassium channel blockers are used to treat resistant ventricular tachycardia and recurrent fibrillation. Drugs in this class have limited uses due to potentially serious toxicity. 10. Class III Potassium Channel Blockers are medications that delay repolarization may cause hypotension, bradycardia, N/V, prolonged QTI (Amiodarone, Cordarone, Pacerone Tikosyn, Corvert, Sotalol/Betapace, Bretylium) 11. Class IV Calcium channel blockers are used to treat atrial dysrhythmias. Calcium channel blockers (CCBs) have antidysrhythmic effects similar to those of beta-adrenergic blockers. This includes reduced automaticity in the SA node, slowed impulse conduction through the AV node, and a prolonged refractory period. CCBs are only effective against atrial dysrhythmias and are indicated for atrial flutter or fibrillation, and the prophylaxis of PSVT. 12. Other Antidysrhythmics: Adenosine and digoxin are used for specific dysrhythmias but do not act by blocking ion channels. Adenosine (Class V) and digoxin (Cardiac Glycoside) are are used for specific dysrhythmias, but do not act by the mechanisms of Class I, II, III, or IV drugs. Adenosine is a drug of choice for serious PSVT. Atrial flutter or fibrillation and PSVT are indications for digoxin.