Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Cardiac contractility modulation wikipedia , lookup
History of invasive and interventional cardiology wikipedia , lookup
Cardiac surgery wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Electrocardiography wikipedia , lookup
Coronary artery disease wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Jatene procedure wikipedia , lookup
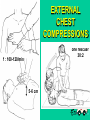
Quantium Medical Cardiac Output wikipedia , lookup
Heart arrhythmia wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
CARDIO PULMO (CEREBRAL) RESUSCITATION Jozef Firment Judita Capková Department of Anaesthesiology & Intensive Medicine Šafárik University Faculty of Medicine, Košice 1 Most frequent causes of out-of-hospital cardiac arrest CA 2 Most common causes of cardiac arrest CA • 1. place IHD...Myocardial infarction (80%) • Hypertension • Valvular disease,.. • • Trauma • Poisoning • Drowning Ventricular fibrilation • Hypotermia... 3 Most common causes of cardiac arrest CA • 1. place IHD...Myocardial infarction • Hypertension Electrical defibrillation – Valvular disease,.. only• effective treatment for VF • • Trauma • Poisoning • Drowning Ventricular fibrilation • Hypotermia... 4 Cause of CA in • Trauma • Drowning • Drug overdose • Children Asphyxia Rescue breaths are critical for resuscitation 5 • In- hospital arrests are due tu PEA or asystole (60-70%) - early recognition of pp at risk may prevent arrest – „Medical Emergency Teams“ • Overall survival to hospital discharge is 10% 6 THE CHAIN OF SURVIVAL Early access to emergency services up to 4 min up to 8 min Early BLS to buy time Early defibrillation to reverse VF Early advanced care to stabilise 7 8 Cervical spine injury • Jaw thrust (no for lay rescuer) or chin lift with manual inline stabilisation of head and neck by an assistant 9 AGONAL BREATHING • Occurs shortly after the heart stops in up to 40% of cardiac arrests • Described as barely, heavy, noisy or gasping breathing • Recognise as a sign of cardiac arrest 10 EXTERNAL CHEST COMPRESSIONS one rescuer 30:2 f : 100-120/min. 5-6 cm 11 Effective chest compressions 12 Effective chest compressions 13 Continous chest compression - only 14 Only 1 in 4 patients in CA recieves bystander CPR • transmission of infection: - tuberculosis, SARS, H1N1 – small number, - HIV – never reported 15 Protective devices: 16 Continous chest compression - only • If layman is not able or is unwilling to perform mouth to mouth breathing • f: 100/min without stopping 17 Basic life support C,A,B Advanced life support C, A, B, Drugs, ECG, Fibrilation treatment - defibrilation... 18 In hospital CPRAdvanced life support One person starts 30:2 others call resuscitation team + defibrillator, r. equipments (airway, ambu bag, adrenalin,..) only one person: leaves the patient, calls resuscitation team starts 30:2 19 VENTILATION MANAGEMENT ALS –In-hospital CPR A: • Oral/nasal airway • Tracheal intubation : f: 10/min , Fi02 = 1,0 (reservoir bag), VT(tidal volume) 6-7 ml/kg, (chest compressions and ventilations continue uninterupted) 20 Laryngeal mask, laryngeal tube Oe-Trach Combitube Oe 90% Trach 21 Campbell B: adults: 15 - “ children 20 - “ - O2 l/min 13 FiO2 % 85-100 4 5 >40 85-100 2 >40 BAG WITH OXYGEN SUPPLY VT x f 1000 x dtto 300 x dtto Inlet O2 10 - 13 l/min 22 Advanced life support Self-inflating bag-mask + oropharyngeal airway : C:V= 30:2 Hyperventilation reduces cerebral blood flow The quality of chest compressions is frequently suboptimal, team leader should change CPR providers 23 Hearth rhytms associated with CA: Ventricular fibrillation Asystole Ventricular tachycardia Electro-mechanical disociation (EMD) Pulseless ventricular activity (PVA) 24 25 DEFIBRILLATION • Paddle positions (sternum, apex), no over the breast tissue • Self- adhesive pads (sparks!!) -the best • Biphasic defibrilators: 1. 150-200J 2. 150-360J,.... • CPR for 2 min (5 x 30:2) after shock 26 DEFIBRILLATION • Check the rhythm (organised QRS complexes: regular + narrow- feeling for a pulse) • After the third shock give: adrenalin 1mg every 3-5 min. iv amiodaron 300mg iv • Time between CC and shock delivery < 5s • Signs of life return :normal breathing, movement, coughing, puls 27 A precordial thump • Generates a small electrical shock • In witnessed and monitored VF/VT arrests if a defibrillator is not immediately available •The ulnar edge of fist the lower half of sternum from a height of 20 cm •Converting VT to sinus rhytm 28 29 LIFE-THREATENING CARDIAC RHYTHM DISTURBANCES Cardiac arrest (asystole) Fine VF will not be shocked successfully Pulseless electrical activity (PEA, EMD)myocardial contractions are too weak to produce pulse or blood pressure 30 POTENTIALLY REVERSIBLE CAUSES (5 H’s & 5 T’s): • • • • Hypoxia Hypovolemia Hypothermia Hyper/hypoK+and metabolic disorders • H+ ions (acidosis) • Tension pneumothorax • Tamponade • Toxic/therap. disturbances • Thrombosis coronary • Thrombosis pulmonary 31 POTENTIALLY REVERSIBLE CAUSES (5 H’s & 5 T’s): • Hypoxia – ventilation with 100% oxygen • Hypovolemia (haemorrhage-trauma, GIT bleeding,rupture of an aortic aneurysm- fluid ( saline or Hartman´s solution + urgent surgery) • Hypothermia (in drowning incident) • Hyper/hypoK+and metabolic disorders • H+ ions (acidosis) 32 POTENTIALLY REVERSIBLE CAUSES • • • • • (5 H’s & 5 T’s): Tension pneumothorax- needle thoracocentesis and chest drain Tamponade – needle pericardiocentesis Toxic substances – appropriate antidotes Thrombosis coronary - thrombolysis Thrombosis pulmonary – trombolytic drug 33 Thoracocentesis 34 Needle pericardiocentesis 35 Thrombosis pulmonary 36 DRUGS USED CPR 1. Adrenaline (EPINEPHRINE) 1 mg á 3’- 5 ’ (EVERY SECOND LOOP(5x CV 30:2) OF THE ALGORYTHM) alpha adrenergic actions cause vasoconstriction, increases myocardial and cerebral perfusion pressure 2. Bicarbonate 50ml 8,4% -pH < 7.1, BE < -10 -hyperkalaemia -tricyclic antidepressant overdose & equipment • (defibrilator) • oxygen • Ambu bag • face mask • F1/1 • infusion set • plastic IV cannula 3. Amiodarone 300 mg after a third unsuccessful defibrillation in VF/VT...150 mg (inf. 900mg/24h) lidocaine 1 mg/kg- alternative 37 DRUG DELIVERY ROUTES • Intravenous (central, peripheral + 20 ml sol. F 1/1 + elevate 10-20 s) • Intraosseal – effective concentrations of drugs is achieved very quickly • Tracheal (2-3x more dose + 10 ml water) (adrenaline, lidocaine, atropine) • NEVER IM nor SC !!! 38 EZ-IO AD Proximal Tibial Access Intraosseous Infusion System 39 Automatický intraoseálny injektor 40 Post – resuscitation care • Stable cardiac rhythm, normal haemodynamic function (thrombolysis, percutaneous coronary intervention) • Intubation, ventilation, sedation • Therapeutical hypothermia • Comatose adults after out-of-hospital VF cardiac arrest were cooled to 32-34 oC for 12-24 h. • Improved neurological outcome 41 • www.erc.edu • www.resus.org. uk • Resuscitation (in october 2010) • http://www.lf.upjs.sk/kaim/pregradualne _vzdelavanie.html 42 Thank you! [email protected] 43 Open chest CPR • better coronary perfusion • Trauma, after cardiothoracic surgery, when chest or abdomen is already open Ectopic rhythm Normal SR 1 2 5 Rhythm disorders at AMI 3 Thrombus development Acute MI 4 45 LIFE-THREATENING CARDIAC RHYTHM DISTURBANCES 1. Ventricular fibrillation, pulseless ventricular tachycardia 2. Cardiac arrest (asystole) 3. Pulseless electrical activity (PEA, EMD) = circulatoty arrest 46 Basic life support - to buy time for Advanced life support – to restore circulation 1961: Peter Safar 47 Effective chest compressions 48