Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
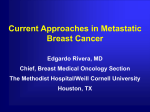
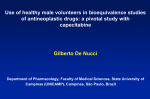
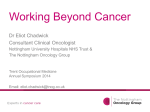
P h a se I a n d P h a rm a c o ki n e t i c S t u dy o f t h e O r a l F l uo ro p y rimid in e Cape c i t a bi n e i n C o m bi n a t i o n W i t h P a c l i ta x e l in P a tie n ts W i t h Adv a n c e d S o l i d Ma l i g n a n c ies By Miguel A. Villalona-Calero, Geoffrey R. Weiss, Howard A. Burris, Maura Kraynak, Gladys Rodrigues, Ronald L. Drengler, S. Gail Eckhardt, Bruno Reigner, Judy Moczygemba, Hans Ulrich Burger, Tom Griffin, Daniel D. Von Hoff, and Eric K. Rowinsky Purpose: To evaluate the feasibility of administering the oral fluoropyrimidine capecitabine in combination with paclitaxel, to characterize the principal toxicities of the combination, to recommend doses for subsequent disease-directed studies, and to determine whether significant pharmacokinetic interactions occur between these agents when combined. Patients and Methods: Sixty-six courses of capecitabine and paclitaxel were administered to 17 patients in a two-stage dose-escalation study. Paclitaxel was administered as a 3-hour intravenous (IV) infusion every 3 weeks, and capecitabine was administered continuously as two divided daily doses. During stage I, capecitabine was escalated to a target dose of 1,657 mg/m2/d, whereas the paclitaxel dose was fixed at 135 mg/m2. In stage II, paclitaxel was increased to a target dose of 175 mg/m2, and the capecitabine dose was the maximum established in stage I. Pharmacokinetics were characterized for each drug when given alone and concurrently. Results: Myelosuppression, predominately neutropenia, was the principal dose-limiting toxicity (DLT). Other toxicities included hand-foot syndrome, diarrhea, hyperbilirubinemia, skin rash, myalgia, and arthralgia. Two patients treated with capecitabine 1,657 mg/m2/d and paclitaxel 175 mg/m2 developed DLTs, whereas none of six patients treated with capecitabine 1,331 mg/m2/d and paclitaxel 175 mg/m2 developed DLTs during course 1. Pharmacokinetic studies indicated that capecitabine and paclitaxel did not affect the pharmacokinetic behavior of each other. No major antitumor responses were noted. Conclusion: Recommended combination doses of continuous capecitabine and paclitaxel are capecitabine 1,331 mg/m2/d and paclitaxel 175 mg/m2/d IV every 3 weeks. Favorable preclinical mechanistic interactions between capecitabine and paclitaxel, as well as an acceptable toxicity profile without clinically relevant pharmacokinetic interactions, support the performance of disease-directed evaluations of this combination. J Clin Oncol 17:1915-1925. r 1999 by American Society of Clinical Oncology. T 58-DFUR was shown to be much more than that of 5-FU, and 58-DFUR was shown to possess potent anticachectic and antimetastatic activity that was not noted with 5-FU.3,4,8,9 In clinical studies, high and predictable oral bioavailability was noted, and 58-DFUR showed prominent antitumor activity in patients with breast, colorectal, and gastric cancers.10-12 However, diarrhea caused by the generation of 5-FU in gastrointestinal tissues that also highly express pyrimidine nucleoside phosphorylases limited the development of 58- HE ORAL FLUOROPYRIMIDINE capecitabine (Xeloda; Hoffmann-LaRoche, Inc, Nutley, NJ; N4pentyloxycarbonyl-58-deoxy-5-fluorocytidine) was rationally synthesized to be efficiently absorbed from the gastrointestinal tract as a prodrug and converted to fluorouracil (5-FU), preferentially in neoplastic tissues (Fig 1).1,2 After gastrointestinal absorption, capecitabine is metabolized to 58-deoxy-5-fluorocytidine (58-DFCR; Furtulon; Roche, Basel, Switzerland) by hepatic carboxyl esterase, and this intermediate is further metabolized to doxifluridine (58-DFUR) by cytidine deaminase in both hepatic and extrahepatic tissues, including malignant tumors.3,4 58DFUR is subsequently metabolized to 5-FU by the enzyme thymidine phosphorylase (dThdPase), which is one of two types of pyrimidine nucleoside phosphorylases.5 dThdPase has recently been shown to be a potent tumor-associated angiogenesis factor with higher expression in tumor cells than normal cells, which may account for the intriguing results reported by some investigators that malignant cells preferentially convert 58-DFUR to 5-FU.6,7 The immediate precursor to capecitabine, 58-DFUR, underwent development as an oral fluoropyrimidine in the 1980s.3,4 In preclinical evaluations, the therapeutic index of From the Institute for Drug Development, Cancer Therapy and Research Center, and The University of Texas Health Science Center at San Antonio, San Antonio; Brooke Army Medical Center, Fort Sam Houston, TX; and Hoffmann-LaRoche, Inc, Nutley, NJ. Submitted September 24, 1998; accepted February 11, 1999. Supported in part by a grant from Hoffmann-LaRoche, Inc, and grant no. MO1 RR01346 from the National Institutes of Health to the Frederic C. Bartter Clinical Research Unit of The Audie Murphy Veterans Administration Hospital. Address reprint requests to Miguel A. Villalona-Calero, MD, Division of Hematology Oncology, Ohio State University, B406 Starling-Louing Hall, Columbus, OH 43210; email [email protected]. r 1999 by American Society of Clinical Oncology. 0732-183X/99/1706-1915 Journal of Clinical Oncology, Vol 17, No 6 (June), 1999: pp 1915-1925 1915 1916 VILLALONA-CALERO ET AL Fig 1. The metabolism of capecitabine. After oral administration, capecitabine is metabolized to 5ⴕ-DFCR by acylamidase in the liver. Cytidine deaminase, which is found in both hepatic and extrahepatic tissues, further metabolizes 5ⴕ-DFCR to 5ⴕ-DFUR. dThdPase, which may be preferentially expressed in neoplastic tissue and upregulated by prior treatment with paclitaxel, metabolizes 5ⴕ-DFUR to 5-FU. DFUR, although it is licensed in Japan.10 In contrast, the carbamate structure of capecitabine precludes its conversion to 5-FU in the intestines; therefore, capecitabine is much less likely to induce diarrhea than 58-DFUR. Indeed, capecitabine administered daily for 3 weeks produced less gastrointestinal toxicity in animals and was more efficacious against the human colon cancer xenografts HCT116 and CXF280 across a broader dosing range than 5-FU administered either intravenously (IV) (three times weekly for 2 weeks) or orally (daily for 3 weeks), or 58-DFUR given orally daily for 3 weeks.1,2 At equitoxic doses, treatment with capecitabine also resulted in substantially greater intratumoral exposure to 5-FU compared with 5-FU itself administered intraperitoneally.13 In early phase I and pharmacologic studies, capecitabine showed efficient and predictable gastrointestinal absorption, with 61% of the administered dose recovered in urine as drug-related material, and the agent was rapidly converted to 58-DFCR and 58-DFUR (time to peak plasma concentration [tmax], 30 minutes).14 In addition, 5-FU concentrations were 2.9-fold higher, on average, in malignant tissues compared with nonmalignant tissues.14 Diarrhea and hand-foot syndrome have been the principal toxicities of capecitabine, and severe myelosuppression has been uncommon on protracted dosing schedules.2,15,16 Recommended phase II dose sched- ules for capecitabine have included 1,331 mg/m2/d in two divided doses daily for 12 weeks and 2,510 mg/m2/d in two divided doses daily for 2 weeks every 3 weeks. Capecitabine on the latter schedule has recently received regulatory approval in the United States for treating patients with paclitaxel-refractory metastatic breast cancer. Because a principal determinant of the therapeutic index of capecitabine-based treatment is the differential rate of conversion of 58-DFUR to 5-FU in malignant and nonmalignant tissues, therapeutic strategies have focused on maximizing the ratio of dThdPase activity in malignant versus nonmalignant tissues. Transfection of the dThdPase gene into the DLD-1 human colon cancer cell line, which is dThdPase-deficient and highly resistant to 58-DFUR, increases dThdPase activity by 1,068-fold and sensitivity to 58-DFUR by 1,070-fold.17 In addition, treatment of malignant tumors with various cytokines, such as tumor necrosis factor-alpha, interleukin-1-alpha, and interferon-gamma (IFN-␥), increases intratumoral dThdPase activity and enhances tumor sensitivity to 58-DFUR in vitro and in vivo.17-19 For example, treatment of nude mice bearing the human colon cancer xenograft COLO205 with human IFN-␥ resulted in an 8.7-fold increase in dThdPase activity in the tumors.19 Although IFN-␥ alone was ineffective against this tumor, it substantially increased the activity of 1917 PHASE I STUDY OF PACLITAXEL AND CAPECITABINE capecitabine, but did so only slightly for 5-FU. Furthermore, treatment of the nude mice bearing a capecitabine-resistant human colon cancer xenograft with paclitaxel, which has been shown to upregulate both interleukin-1-alpha and tumor necrosis factor-alpha, resulted in a 7.9-fold increase in intratumoral dThdPase activity.19,20 In this model, dThdPase activity increased 4 days after treatment with paclitaxel and remained elevated for up to 10 days (Ishitsuka et al, unpublished results). Paclitaxel, capecitabine, or 5-FU alone did not appreciably inhibit tumor growth, whereas the combination of 5-FU and paclitaxel was additive, and the combination of capecitabine and paclitaxel produced synergy. To date, these results with capecitabine provide both mechanistic and clinical rationale to evaluate the feasibility of administering it in combination with paclitaxel. In addition, the overlapping antitumor activities of both singleagent capecitabine and paclitaxel in several tumor types, particularly breast cancer, as well as the nonoverlapping principal toxicities of these agents, support a rationale for the evaluation of this combination regimen. The principal objectives of this phase I and pharmacokinetic study were as follows: (1) to determine the maximum-tolerated doses (MTDs) of capecitabine administered twice daily in combination with paclitaxel as a 3-hour IV infusion every 3 weeks to patients with advanced solid malignancies; (2) to describe and quantitate the toxicities of the capecitabine-paclitaxel regimen; (3) to characterize the individual pharmacokinetic behavior of both paclitaxel and capecitabine and determine whether significant pharmacokinetic interactions occur when the agents are administered in combination; and (4) to seek preliminary evidence of antitumor activity for this combination. PATIENTS AND METHODS Eligibility Patients with histologically confirmed solid malignancies refractory to conventional therapy or for whom no effective therapy existed were candidates for this study. Eligibility criteria also included the following: age ⱖ 18 years; Karnofsky performance status ⱖ 70% (ambulatory and capable of self-care); a life expectancy ⱖ 3 months; no major surgery, radiotherapy, or chemotherapy within 28 days (42 days for mitomycin or nitrosourea); no history of major disorders or surgery involving the stomach, small intestines, liver, or kidney that might affect the gastrointestinal absorption or clearance of capecitabine; adequate hematopoietic (WBC count ⱖ 3,000/µL, absolute neutrophil count [ANC] ⱖ 1,500/µL, platelet count ⱖ 100,000/µL, and hemoglobin level ⱖ 9.0 g/dL), hepatic (total bilirubin level ⬍ 1.5 times the upper normal limits; AST, ALT, and alkaline phosphatase ⬍ 2.5 times the upper normal limits), and renal (serum creatinine ⬍ 1.5 times the upper normal limits) functions; no clinically significant cardiac disease (New York Heart Association class III or IV); no history of seizures, CNS disorders, or psychiatric disease that might affect study compliance; no evidence of brain metastases; no history of hypersensitivity to paclitaxel or other drugs formulated in Cremophor EL (polyoxyethylated castor oil); no requirement for chronic corticosteroids except for inhalation therapy; and no prior documentation of hepatitis B surface antigen, hepatitis C antibodies, or human immunodeficiency virus type 1 antibodies, although such viral evaluations were not required for eligibility. All patients gave informed written consent before treatment. Dosage and Dose Escalation The starting doses were paclitaxel 135 mg/m2 as a 3-hour IV infusion and capecitabine 1,004 mg/m2/d orally in two divided doses every 12 hours. These dose schedules resulted in antitumor activity and minimal toxicity when either drug was administered as a single agent in similar patient populations.2,21 Paclitaxel was administered on day 1 and repeated every 3 weeks. Capecitabine was begun on day 3 after the first paclitaxel treatment and continued for the duration of the study. The capecitabine dose levels evaluated were identical to those evaluated in phase I single-agent studies to facilitate comparisons of results of combination and single-agent studies. Doses of either capecitabine or paclitaxel were escalated in each successive cohort of new patients in two stages. In stage I, the goal was to progressively increase the dose of capecitabine from 1,004 mg/m2/d to 1,331 mg/m2/d and then to the target dose of 1,657 mg/m2/d, which was the MTD established on a continuous daily dosing schedule,2 whereas the dose of paclitaxel was fixed at 135 mg/m2. No dose escalation greater than 1,657 mg/m2 in the capecitabine dose was to be undertaken. In stage II, the goal was to increase the dose of paclitaxel from 135 mg/m2 to a clinically relevant target dose of 175 mg/m2, with the initial dose of capecitabine being the highest safest dose level established in stage I. A minimum of three new patients were to be treated at all tolerable dose levels. Intrapatient dose escalation was not permitted. Toxicities were graded according to the National Cancer Institute Common Toxicity Criteria.22 Dose-limiting toxicity (DLT) was defined as ANC less than 500/µL for longer than 5 days or less than 1,000/µL with fever; platelet count less than 25,000/µL; hemoglobin level less than 6.5 mg/dL; and nonhematologic toxicity of at least grade 3 (including diarrhea, nausea, and vomiting) that did not improve to at least grade 1 within 2 days after the institution of appropriate therapy, or that led to the interruption of capecitabine treatment or delayed paclitaxel treatment for more than 2 weeks. If DLTs occurred, a maximum of six new patients was treated at that dose level. The MTD level was defined as the highest capecitabine dose up to 1,657 mg/m2/d, which when combined with paclitaxel 175 mg/m2, induced DLTs in less than two of six new patients during their first cycle of therapy. Drug Administration Capecitabine was supplied by Hoffmann-LaRoche, Inc (Nutley, NJ) as 100-, 150-, 500-, or 750-mg film-coated tablets. After the total dose was calculated according to body surface area, it was then rounded off to the nearest 50 mg. The precise dose of capecitabine, which was packed individually in a mediplanner dispensing cassette (Health Care Logistics, Circleville, OH), was administered with 200 mL of water within 30 minutes of ingesting solid food. Capecitabine was to be taken every 12 ⫾ 2 hours. Paclitaxel (Taxol; Bristol-Myers Squibb, Princeton, NJ) was supplied in 30-mg (5-mL) vials, with each milliliter containing 6 mg of paclitaxel, 527 mg of polyoxyethylated castor oil (Cremophor EL; BASF, Aktiengesellschaft, Germany), and 49.5% dehydrated alcohol (United States Pharmacopeia). Paclitaxel was diluted with either 0.9% sodium chloride solution or 5% dextrose solution to a final concentration of 0.3 to 1.2 mg/mL administered as an IV infusion over 3 hours using a Harvard pump (Harvard Apparatus Inc, South Natick, MA). The following medication was administered before paclitaxel: 1918 dexamethasone 20 mg orally 6 and 12 hours before treatment; diphenhydramine 50 mg IV 30 to 60 minutes before treatment; and either cimetidine 300 mg IV or ranitidine 50 mg IV 30 to 60 minutes before treatment. Dosage Modifications Treatment with capecitabine was discontinued if patients developed at least grade 2 nonhematologic (except isolated hyperbilirubinemia) or grade 3 hematologic toxicity. Treatment was resumed when toxicity resolved to grade 0 to 1 at either the original dose level (for grade 2 nonhematologic toxicity; grades 2 to 4 hematologic toxicity; grade 3 nausea and vomiting; and grade 3 palmar-plantar erythrodysesthesia) or at the next lower dose level for all other grade 3 nonhematologic toxicities. Patients were to be withdrawn from study if they developed any grade 4 nonhematologic toxicity, unless an objective response was documented, in which case treatment with capecitabine at the next lower dose level was continued. If patients had persistent toxicity of at least grade 2 in severity on the scheduled day of paclitaxel administration, treatment was delayed for 1 week. If the toxicity did not resolve to ⱕ grade 1 after a 1-week treatment delay, the patient was withdrawn from study unless clinical benefit was documented, in which case a treatment delay of up to 2 additional weeks was permitted. For patients who experienced DLTs during the previous course, the paclitaxel dose was reduced to the next lower dose level or by 25% if DLTs occurred at the 135-mg/m2 dose level. Pretreatment Assessment and Follow-Up Studies Histories, physical examinations, and routine laboratory studies were performed before treatment and weekly after treatment. Routine laboratory studies included serum electrolytes, chemistries, complete blood cell count with differential WBC count, clotting times, and urinalysis. If patients developed toxicity manifested by grade 3 or 4 abnormalities in hematologic or biochemical laboratory parameters, the tests were repeated immediately and then daily until the toxicity resolved. Tumors were measured after every two courses, and treatment was continued in the absence of progressive disease or intolerable toxicity. A complete response was defined as the disappearance of all disease on two measurements separated by a minimum of 4 weeks. A partial response required more than 50% reduction in the sum of the products of the bidimensional measurements of all measurable lesions documented by two measurements separated by at least 4 weeks. Plasma Sampling and Assay To assess the effects of capecitabine on the pharmacokinetics of paclitaxel, blood was sampled for analysis of paclitaxel concentrations after treatment on day 1 (before treatment with capecitabine) and day 22 (during treatment with capecitabine). Samples were collected from indwelling venous catheters in the arm contralateral to the paclitaxel infusion. For the analysis of paclitaxel, sampling times included pretreatment, 2 hours into the infusion and immediately before the end of the 3-hour infusion, and 3.5, 4, 5, 8, 11, 23, 30, and 48 hours after the start of infusion. Paclitaxel plasma concentrations were measured by liquid chromatography/mass spectroscopy as described previously.23 For analysis of capecitabine and capecitabine metabolites, blood samples were collected before capecitabine treatment and at 0.5, 1, 2, 3, 4, 5, 6, 8, and 12 (immediately before the evening dose) hours after treatment. Five-milliliter samples were collected into Vacutainer tubes (Becton Dickinson, Rutherford, NJ) containing EDTA, except when sampling times for paclitaxel and capecitabine coincided, in which case 10-mL samples were obtained. Blood samples were immediately VILLALONA-CALERO ET AL centrifuged to separate plasma, and at least 2 mL of plasma was transferred into polypropylene tubes and frozen at ⫺20°C. Concentrations of capecitabine and its metabolites 58-DFCR, 58-DFUR, 5-FU, 58-68-dihydrofluorouracil (5-FUH2), and fluoro-beta-alanine (FBAL) were measured by means of a validated liquid chromatography/mass spectrometry technique, as previously described.24 Pharmacokinetic Analysis Estimates of pharmacokinetic parameters for paclitaxel and capecitabine and its metabolites were derived from individual concentration-time data sets using noncompartmental methods and the program SAS, version 6.11 for Windows (SAS Institute, Inc, Cary, NC).25 The values for area under the concentration-time curve (AUC) were calculated using the linear trapezoidal method with extrapolation of the curve to infinity (AUC0-⬁), and from time 0 to the last sampling time at which the concentration could be measured (AUC0-t). The following pharmacokinetic parameters were also determined: maximum plasma concentration (Cmax), tmax, and apparent half-life of elimination (t1/2). For paclitaxel, total clearance (CLs) was estimated by dividing the dose (in milligrams) by AUC0-⬁, and the volume of distribution (Vd) was calculated from CLs/k, where k was the terminal rate constant of elimination. Descriptive statistics were used to summarize all pharmacokinetic parameters. Mean, SD, coefficient of variation, minimum, maximum, and median values were determined for all parameters. In addition, geometric mean and geometric coefficient of variation were determined for Cmax, AUC0-t, and AUC0-⬁. Clinically relevant pharmacokinetic interactions between capecitabine and paclitaxel were sought. Plasma samples obtained on day 1 were used to evaluate the pharmacokinetics of paclitaxel alone, whereas day-15 samples were used to evaluate the pharmacokinetics of capecitabine alone, and day-22 values were used to evaluate the pharmacokinetics of both drugs given in combination. For 58-DFUR, 58-DFCR, and 5-FU, the AUC0-⬁ values estimated on days 15 and 22 were used for statistical comparisons. For both capecitabine and 5-FUH2, the AUC0-t was assessed because AUC0-⬁ could not be estimated reliably in all patients. For FBAL, the AUC0-12 was evaluated. Paired t tests were performed for statistical comparisons of AUC between treatment days. Because several dosing groups of paclitaxel and capecitabine were used in the analysis, a three-way analysis of variance, with dose and day as fixed factors and subject nested in the dose group as the random factor, was performed for the logarithmically transformed AUC estimates of paclitaxel on day 1, of capecitabine and metabolites on day 15, and of paclitaxel, capecitabine, and capecitabine metabolites on day 22. Statistical analysis was performed using both StatView version 5.0 statistical software program and the general linear models program in PROC GLM of SAS version 6.11 (both from SAS Institute). RESULTS General The number of new and total patients, courses, and rates of DLTs as a function of dose level are listed in Table 1. Seventeen patients received 66 assessable courses of paclitaxel and capecitabine. Two other patients were not assessable for toxicity because treatment was discontinued early during their first course as a result of rapidly progressive disease. Patient characteristics are listed in Table 2. Sixteen patients received prior chemotherapy and 10 subjects were previously treated with both chemotherapy and radiation therapy. During study stage I, the daily dose of capecitabine 1919 PHASE I STUDY OF PACLITAXEL AND CAPECITABINE Table 1. Dose Escalation Scheme Hematologic Toxicity No. of Patients Dose (mg/m2/d) Paclitaxel Capecitabine New 135 135 135 175 175 Total 1,004 1,331 1,657 1,657 1,331 3 3 3 2 6 17 Reduced to This Dose Total 0 1 0 0 1 3 4 3 2 7 Total Courses 12 18 10 2 24 66 New Patients With DLT/ Total New Patients* 0/3 0/3 0/3 2/2 0/6 *During course 1. was increased from 1,004 to 1,657 mg/m2/d, and the dose of paclitaxel was fixed at 135 mg/m2. Because there were no dose-limiting events in patients treated with capecitabine doses as high as 1,657 mg/m2/d, which was the dose recommended for phase II studies of capecitabine as a single agent on a continuous treatment schedule,2 the study was amended, and further dose escalation of capecitabine was not pursued. Instead, the dose of paclitaxel was increased to 175 mg/m2, and because no DLTs were observed with capecitabine 1,657 mg/m2/d in study stage I, this dose was administered to the first cohort of patients in stage II. However, DLT, characterized by fever associated with neutropenia, occurred during course 1 in the first two patients treated at this dose level. Therefore, the daily dose of capecitabine was decreased to 1,331 mg/m2/d in combination with paclitaxel 175 mg/m2 in the next cohort of patients. None of the six new patients treated at this dose level developed DLTs during course 1, and only two of 24 total courses were associated with DLT, which consisted of grade 3 diarrhea that lasted longer than 2 days (course 2) and severe neutropenia associated with fever (course 3). No objective antitumor responses were observed. Table 2. Characteristics of Patients No. of Patients Characteristic Male/female Age, years Median Range Karnofsky performance status, % Median Range Previous treatment Chemotherapy Chemotherapy ⫹ radiation therapy Disease site Colorectal Esophagus Breast Osteosarcoma Unknown primary tumor 13/4 63 48-72 Myelosuppression, predominately neutropenia, was the principal DLT in this study. Table 3 lists the number of courses associated with grade 3 (ANC ⱖ 500/µL and ⬍ 1,000/µL) and grade 4 (ANC ⬍ 500/µL) neutropenia, severe (grade 3 to 4) neutropenia associated with fever, prolonged (⬎ 5 days) grade 4 neutropenia, and severe thrombocytopenia (platelet count ⬍ 50,000/µL). Overall, 10 of 17 patients (58%) developed either grades 3 or 4 neutropenia during 18 of 66 courses (27%). However, the duration of grade 4 neutropenia never exceeded 5 days, and the duration of grade 4 neutropenia was short (median, 2 days). Fever associated with grade 3 or 4 neutropenia was experienced by three subjects (17%) during three courses (4.5%). Onset of neutropenia occurred on days 7 to 15; the mean time to ANC nadir was 15 days (range, 8 to 15 days); and the median time to complete recovery was 7 days. Recovery of blood cell counts to pretreatment levels was usually complete by day 22, and paclitaxel treatment delay because of incomplete recovery of ANCs was required in only one of 66 courses. Anemia and thrombocytopenia were typically mild and infrequent, with only one patient experiencing grade 3 anemia and no patients experiencing grades 3 or 4 thrombocytopenia. DLT, consisting of grades 3 to 4 neutropenia associated with fever, was initially noted in two patients treated with capecitabine 1,657 mg/m2/d and paclitaxel 175 mg/m2. Another individual developed grade 3 neutropenia associated with fever during his third course of capecitabine/ paclitaxel at the next lower dose level (1,331 mg/m2/d and 175 mg/m2, respectively). Gram-negative bacteremia without sepsis was documented in two of these three patients. Complete recovery of the ANC to pretreatment levels occurred 5 days after the onset of neutropenia in all of these patients. In one of the patients who was initially treated with capecitabine 1,657 mg/m2/d and paclitaxel 175 mg/m2, grades 2 and 3 neutropenia were noted on two occasions soon after resumption of treatment with capecitabine 1,657 mg/m2/d. Nonhematologic Toxicity 90 80-100 16 10 12 2 1 1 1 The principal nonhematologic toxicities of this regimen of capecitabine and paclitaxel are listed in Table 4. Eleven patients experienced diarrhea, which was typically mild to moderate (grade ⱕ 2 in nine patients) and brief (median duration, 2 days [range, 2 to 12 days]). Neither the incidence nor severity of diarrhea seemed to be related to dose level. However, diarrhea seemed to be cumulative, generally occurring after a median of two courses. Except for the diarrhea that occurred in one individual, all other episodes were successfully managed with brief courses of either 1920 VILLALONA-CALERO ET AL Table 3. Hematologic Toxicity of Capecitabine Plus Paclitaxel No. of Courses With: Dose Level Neutropenia Grade 4 Grade 4 ⬎ 5 days Grades 3-4 With Fever Thrombocytopenia Grades 3 and 4 0 1 0 1 6 0 0 0 0 0 0 0 0 2 1 0 0 0 0 0 ANC (/L) Nadir Paclitaxel (mg/m2) Capecitabine (mg/m2/d) Total No. of Patients/Courses Median Range Grade 3 135 135 135 175 175 1,004 1,331 1,657 1,657 1,331 3/12 4/18* 3/10 2/2 7/24* 2150 1260 688 357 540 1,110-3,290 541-5,430 629-1,860 36-714 277-3,854 0 2 3 1 4 *Includes courses administered to two patients whose capecitabine/paclitaxel dose level was reduced after initial assignment to the 1,657/175-mg/m2 dose level. loperamide or diphenoxylate hydrochloride. A 59-year-old man with rectal cancer who was previously treated with radiation to his pelvis and rectum developed grade 3 diarrhea 4 days after his second treatment with paclitaxel during course 2 at the capecitabine/paclitaxel dose level of 1,331 mg/m2/d and 175 mg/m2, respectively, but these complaints were temporally related to the initiation of treatment with laxatives for constipation. His diarrhea was still present, albeit grade 1 in severity, at the time of his death from progressive disease 12 days after onset. A second patient developed grade 3 diarrhea that lasted 1 day during his third course of capecitabine/paclitaxel at 1,331 mg/m2/d and 135 mg/m2, respectively. Elevations in serum bilirubin concentrations occurred in eight patients during 12 courses. The onset of bilirubin elevations occurred between days 8 and 22 (median, day 15). Concomitant elevations in serum transaminases and alkaline phosphatase were noted in one patient only. Fractionation of total bilirubin in two of the eight individuals showed that unconjugated bilirubin accounted for most of the elevation. The absolute elevations were generally modest (median peak serum bilirubin concentration, 1.4 mg/dL [range, 1.1 to 2.4 mg/dL]), and cumulative toxicity was not observed. In addition, treatment with capecitabine was never interrupted for hyperbilirubinemia, and hyperbilirubinemia resolved after a median of 8 days in all individuals. For these reasons, despite the fact that several of these elevations met the criteria for grade 3 toxicity using the National Cancer Institute Common Toxicity Criteria (1.5 to three times the upper normal limit), these adverse effects were not considered dose-limiting. One patient developed hand-foot syndrome. The patient, a 61-year-old man with metastatic colon cancer who was treated with capecitabine 1,657 mg/m2/d and paclitaxel 135 mg/m2, developed a symmetrical erythematous macular rash on both of his forearms and hands 15 days after beginning treatment. Because of the concomitant development of grade 3 neutropenia, treatment with capecitabine was delayed for 5 days and then begun again at the same dose after complete hematologic recovery and improvement of his rash. However, 7 days after treatment with his second dose of paclitaxel on day 22, he developed abdominal cramping (grade 2), nausea and vomiting (grade 2), diarrhea (grade 2), and neutropenia (grade 3). His hands were tender, edematous, and erythematous, and a rash involving his arms, shoulders, face, and trunk was also noted. These toxic manifestations resolved after capecitabine and paclitaxel were discontinued, and no further treatment was administered because of the development of progressive disease. Two additional patients treated with capecitabine 1,657 or 1,004 mg/m2/d and paclitaxel 135 mg/m2 developed ery- Table 4. Nonhematologic Toxicities of Capecitabine Plus Paclitaxel* No. of Courses With: Dose Level Diarrhea Hyperbilirubinemia Skin Rash Myalgia-Arthralgia Paclitaxel (mg/m2) Capecitabine (mg/m2/d) No. of Courses 1 2 3 4 1 2 3 4 1 2 3 4 1 2 3 135 135 135 175 175 1,004 1,331 1,657 1,657 1,331 12 18 10 2 24 1 0 0 0 1 1 1 2 2 3 0 0 1 0 1 0 0 0 0 0 0 0 0 0 0 0 2 1 1 3 0 1 2 1 1 0 0 0 0 0 1 0 1 1 2 1 0 1 0 1 0 0 1 0 0 0 0 0 0 0 0 0 0 0 0 0 2 1 0 2 1 0 1 0 0 *Toxicity grading: Diarrhea: 1) increase by two to three stools/day over pretreatment; 2) increase by four to six stools/day or nocturnal stools; 3) increase by seven to nine stools/day or incontinence; 4) increase by ⱖ 10 stools/day, grossly bloody diarrhea, or need for parenteral support. Hyperbilirubinemia: 1) not graded as; 2) one to 1.5 upper normal limit; 3) 1.5 to three times upper normal limit; 4) ⬎ three times upper normal limit. Skin rash: 1) scattered macular or papular eruption, or erythema that is asymptomatic; 2) scattered macular or papular eruption, or erythema with pruritus or other symptoms; 3) generalized symptomatic macular, papular, or vesicular eruption; 4) exfoliative dermatitis or ulceration dermatitis. Myalgias–arthralgias: 1) mild; 2) moderate; 3) severe. 1921 PHASE I STUDY OF PACLITAXEL AND CAPECITABINE thematous pruritic eruptions on their hands, which was not typical of hand-foot syndrome, and therapy was not interrupted. Seven patients experienced myalgia and/or arthralgia. The onset of symptoms was typically 2 to 4 days after treatment with paclitaxel 135 and 175 mg/m2. Myalgia and arthralgia generally lasted 2 to 7 days and were managed successfully with either nonsteroidal anti-inflammatory medications or acetaminophen. Other mild to moderate drug-related toxicities, which seemed unrelated to dose level, included mucositis, nausea, vomiting, alopecia, conjunctivitis, facial flushing, lower extremity edema, paresthesia, and malaise. In addition, a 72-year-old man with rectal carcinoma and lung metastasis who was previously treated with radiation to his primary rectal lesion, as well as interstitial irradiation for a stage B prostate cancer, developed hemorrhagic cystitis 21 days after beginning his first course of capecitabine 1,331 mg/m2/d and paclitaxel 135 mg/m2. Cystoscopy showed a large, friable necrotic mass involving the left trigone of his bladder that was associated with extensive mucosal inflammation. Biopsy specimens of the mass and adjacent bladder showed cystitis, which was believed to be caused by a radiation recall phenomenon. Pharmacokinetic Studies Plasma samples for pharmacokinetic studies were obtained in all 17 patients on day 1 (treatment with paclitaxel alone), 11 patients on day 15 (treatment with capecitabine alone), and 14 patients on day 22 (concurrent treatment with paclitaxel and capecitabine). Therefore, 11 paired samples were available to assess the effects of paclitaxel on capecitabine pharmacokinetics, and 14 paired samples were available to assess the effects of capecitabine on paclitaxel pharmacokinetics. At paclitaxel doses of 135 and 175 mg/m2, AUC0-⬁ values on day 1 averaged 10,829 and 16,045 ng-h/mL, respectively. Mean (⫾SD) paclitaxel pharmacokinetic parameters on day 1 included a Vd of 565.46 ⫾ 224.8 L, a t1/2 of 16.7 ⫾ 4.9 hours, and a CLs of 24.01 ⫾ 7.1 L/h. Paclitaxel pharmacokinetic parameters are listed in Table 5, and cumulative plasma concentration-versus-time profiles for paclitaxel administered alone (day 1) and concurrent with capecitabine (day 22) are shown in Fig 2. Scatterplots depicting AUC and Cmax values of capecitabine and capecitabine metabolites as a function of capecitabine dose are shown in Fig 3. Although the sample size was small, the relationship between capecitabine dose and AUC appeared linear in the capecitabine dosing range evaluated. Figure 4 shows plasma concentration-versus-time curves for capecitabine and capecitabine metabolites from a representative patient, and pharmacokinetic parameter values for Table 5. Paclitaxel Pharmacokinetic Parameters Before Treatment With Capecitabine (Day 1) and During Capecitabine (Day 22)* Pharmacokinetic Parameter Paclitaxel 135 (n ⫽ 6) Cmax, ng/mL AUC0-⬁, ng-h/mL t1/2, h CLs, L/h Vd, L Paclitaxel 175 mg/m2 (n ⫽ 8) Cmax, ng/mL AUC0-⬁, ng-h/mL t1/2, h CLs, L/h Vd, L Before Capecitabine Treatment (Day 1) During Capecitabine Treatment (Day 22) Mean % Mean % 2,614 10,829 15.5 25.8 550.3 20 27 35 34 61 2,390 10,191 15.0 26.7 540.9 26 28 32 33 57 3,980 16,045 16.9 21.2 503.3 35 21 26 19 30 4,434 18,664 14.0 18.2 343.2 21 19 38 24 30 mg/m2 *Values represent geometric mean and coefficient of variation (percent) for Cmax, AUC0-t, AUC0-⬁, CLs, and Vd, and arithmetic means and coefficient of variation (percent) for t1/2. prodrug and metabolites in patients treated with two daily doses of capecitabine 666.5 mg/m2 (1,331 mg/m2/d) on day 15 are listed in Table 6. Peak capecitabine plasma concentrations occurred at a median of 1.05 hours (range, 0.5 to 4.05 hours) after capecitabine administration, whereas maximum plasma concentrations of 58-DFCR, 58-DFUR, and 5-FU were noted at median of 2.02 hours (range, 0.50 to 4.05 hours) after treatment. Median tmax values for 5-FUH2 and FBAL were 3 hours (range, 1.03 to 4.05 hours) and 3.03 hours (range, 1.98 to 5.13 hours), respectively. Despite nearly identical tmax values for 58-DFUR and 5-FU, AUC values for 5-FU were 26.5-fold lower, on average, than those for 58-DFUR at the recommended dose of capecitabine (1,331 mg/m2/d) in this study. The potential influence of capecitabine on paclitaxel pharmacokinetics was assessed. Paclitaxel AUC0-⬁ values that resulted from the administration of paclitaxel alone (day 1) were compared with AUC0-⬁ values obtained when paclitaxel and capecitabine were administered concurrently (day 22) using paired data sets. Paclitaxel exposure was not affected by capecitabine, as shown by paired comparisons of AUC0-⬁ values obtained on days 1 and 22 (paired t test, P ⫽ .80). Similarly, the potential influence of paclitaxel on the pharmacokinetics of capecitabine and capecitabine metabolites was assessed by comparing AUC and Cmax values obtained when capecitabine was administered before treatment with paclitaxel (day 15), with parameter values obtained when capecitabine and paclitaxel were administered concurrently (day 22). Paired analyses showed that paclitaxel did not significantly affect the AUC of capecitabine or any of its metabolites (paired t test, P ⬎ .1 for all comparisons). In addition, Cmax values for capecitabine, 1922 VILLALONA-CALERO ET AL 58-DFCR, 58-DFUR, 5-FU, 5-FUH2, and FBAL before and during treatment with paclitaxel were similar (paired t test, P ⬎ .10 for all comparisons). Similar analyses using three-way analysis of variance for logarithmically transformed AUC estimates of paclitaxel on day 1, capecitabine and capecitabine metabolites on day 15, and all moieties on day 22 showed no significant effects of paclitaxel on the AUC of capecitabine and capecitabine metabolites and visa versa, except for the AUC of FBAL, which was significantly lower when capecitabine and paclitaxel were administered concurrently (P ⫽ .02). DISCUSSION The high and predictable oral bioavailability of capecitabine, as well as the preferential conversion of this prodrug to 5-FU in neoplastic tissues, as shown by several investigators,1,13,14 render capecitabine one of the most interesting fluoropyrimidines undergoing development. dThdPase, which Fig 3. Scatterplots depicting AUC and Cmax values of capecitabine (䊊), 5-DFCR (䉭), 5-DFUR (䊉) and 5-FU (ⴛ) as a function of capecitabine dose. Fig 2. Mean plasma concentration-versus-time curves for paclitaxel administered before treatment with capecitabine on day 1 and during treatment with capecitabine on day 22. is highly expressed in neoplastic tissue and may account for the preferential metabolism of 58-DFUR to 5-FU in malignant neoplasms, has been shown to be upregulated in human colon cancer xenografts after treatment with paclitaxel, and synergy between paclitaxel and capecitabine has also been noted.19 On the basis of this preclinical rationale and the overlapping clinical antitumor spectra of these agents, this phase I pharmacologic study was performed to evaluate the feasibility of administering capecitabine and paclitaxel in combination and to study the pharmacologic profiles and potential for pharmacokinetic interactions between these agents. Myelosuppression, predominately neutropenia, was the principal DLT. However, clinically relevant single-agent doses of both paclitaxel and capecitabine were able to be administered in combination. Because the incidence of severe neutropenia associated with fever at the paclitaxel 175-mg/m2 and capecitabine 1,657-mg/m2/d dose level was unacceptably high, the dose level of paclitaxel 175 mg/m2 and capecitabine 1,331 mg/m2/d, consisting of paclitaxel 1923 PHASE I STUDY OF PACLITAXEL AND CAPECITABINE hyperbilirubinemia was not clinically significant.2,15,16 In contrast to the results of early studies, four of the eight individuals who developed hyperbilirubinemia in the present study did not have liver metastases, including two of the three patients with grade 3 toxicity, and only one subject had concomitant elevations of other liver function tests. In addition, the elevation was largely caused by unconjugated bilirubin. The relative early tmax values for all metabolites, particularly 58-DFUR, and higher Cmax and AUC values for 58-DFUR relative to both capecitabine and 58-DFCR, indicate that capecitabine is rapidly and extensively metabolized to 58-DFUR. Interestingly, systemic exposure to 58-DFUR, as estimated from AUC values in plasma, was nearly 30-fold greater, on average, than that of 5-FU. However, because conversion of 58-DFUR to 5-FU is largely an intracellular process that primarily occurs in peripheral tissues,5 the relative exposures of capecitabine and its metabolites based on AUC value estimates from plasma concentrations in this study may not accurately reflect the relative exposure of peripheral tissues and malignant tumors to capecitabine and capecitabine metabolites. Nevertheless, significant pharmacokinetic interactions between paclitaxel, capecitabine, and capecitabine metabolites were not evident. Although hepatic metabolism and/or biliary excretion play a principal role in the metabolism and clearance of both capecitabine and paclitaxel, significant pharmacokinetic interactions would not have been anticipated because the principal mechanisms of hepatic involvement in the metabolism and disposition of capecitabine and paclitaxel are different. Paclitaxel is primarily metabolized by hepatic cytochrome P450 isoform CYP2C to 6-alpha-hydroxypaclitaxel, with hepatic cytochrome P450 isoform CYP3A accounting for a minor degree of drug disposition,27 whereas capecitabine is not metabolized by hepatic cytochrome P450–dependent processes (Hirose et al, unpublished results). In fact, capecitabine neither inhibits nor induces hepatic cytochrome P450 mixed function oxidases. Fig 4. Plasma concentration-versus-time curves for capecitabine and metabolites on day 15 in a patient treated with capecitabine 1,331 mg/m2/d. 175 mg/m2 every 3 weeks and capecitabine in two divided daily doses of 666 mg/m2, was the MTD and recommended dose level for subsequent evaluations. Overall, both the qualitative and quantitative aspects of the hematologic effects at the paclitaxel 175-mg/m2 and capecitabine 1,331mg/m2/d dose level were similar to those observed with paclitaxel 175 mg/m2 administered as a single agent over 3 hours.21,26 However, several observations, such as the recurrence of neutropenia when capecitabine was restarted after a treatment delay in a patient who had recovered from severe neutropenia, presumably caused by paclitaxel, indicates that capecitabine may also contribute to the neutropenia that occurs with the paclitaxel/capecitabine regimen. Qualitatively, the nonhematologic effects of the capecitabine/paclitaxel combination were similar to the toxicities of either capecitabine (diarrhea, rash, flushing, hand-foot syndrome, nausea, vomiting, and mucositis) or paclitaxel (myalgia, arthralgia, asthenia, peripheral neurotoxicity, malaise, and alopecia) administered as single agents.2,15,16,22 The development of hyperbilirubinemia in eight patients during 12 courses is of interest, but increases in serum bilirubin levels were also noted in early studies of capecitabine administered as a single agent, and, as in the present study, Table 6. Pharmacokinetic Parameters for Capecitabine and Metabolites Before Treatment With Paclitaxel (Day 15) at the Capecitabine/Paclitaxel Dose Level of 175/1,331 mg/m2* Pharmacokinetic Parameter Cmax, g/mL tmax, hours Median Range AUC0-t, g-h/mL AUC0-⬁, g-h/mL t1/2, hours Capecitabine 58-DFCR 58-DFUR 5-FU 5-FUH2 FBAL Mean % Mean % Mean % Mean % Mean % 2.93 74 1.78 105 5.10 18 0.196 42 0.736 25 1.01 0.50-3.00 3.59 44 3.83 56 0.51 18 1.99 0.52-4.02 3.32 87 3.44 84 0.79 22 1.99 0.52-4.02 8.92 13 9.04 14 0.69 16 1.99 0.52-4.02 0.334 31 0.341 30 0.87 49 *Patients treated with capecitabine 1,331 mg/m2/d in two divided daily doses of 665.5 mg/m2. 2.01 1.03-4.02 2.09 8 2.22 9 1.23 40 Mean 3.60 % 30 2.99 1.98-5.13 20.2 33 20.9 35 3.57 24 1924 VILLALONA-CALERO ET AL The fact that there were no major antitumor responses noted in the present study must be tempered by the knowledge that 15 of the 17 subjects were previously shown to be clearly refractory to 5-FU, with progressive tumor growth occurring during prior treatment with 5-FU–based regimens, and that at least 13 of the 17 patients had malignant neoplasms that are considered innately resistant to the taxanes. Still, the experimental evidence that paclitaxel upregulates dThdPase in malignant cells in vitro is intriguing and provides a rationale for further evaluations of combination regimens consisting of paclitaxel and capecitabine.19 In addition to this specific molecular interaction, perhaps the most impressive cytotoxic interactions between the taxanes and other cytotoxic agents have been between the taxanes and 5-FU, which further supports the development of this drug combination.28,29 Although the specific capecitabine/paclitaxel regimen that was evaluated in the present trial was selected, in part, to achieve protracted exposure to 5-FU and maximal convenience for patients, other capecitabine/paclitaxel treatment schedules may increase the likelihood that favorable pharmacologic and molecular drug interactions between these agents will occur. For example, administering paclitaxel on a more frequent schedule, such as on a weekly low-dose schedule, may result in more protracted periods of dThdPase upregulation, as well as coexposure of tumors to both capecitabine and paclitaxel. Alternatively, the administration of higher doses of capecitabine has been shown to be more feasible on less protracted capecitabine daily dosing (eg, 14-day) schedules compared with continuous daily treatment schedules.15 Also, the use of shorter, albeit more intensive, capecitabine regimens may hypothetically provide maximal concentrations of the 5-DFUR substrate to dThdPase during periods when the enzyme is maximally upregulated after treatment with paclitaxel. The overall results of this study indicate that the administration of clinically relevant single-agent doses of both capecitabine and paclitaxel is feasible in patients with solid malignancies, and that there are no relevant pharmacologic interactions between capecitabine and paclitaxel that might complicate the further development and broad usage of the regimen. On the basis of the toxicologic profile of the capecitabine/paclitaxel regimen shown in the present study, paclitaxel 175 mg/m2 as a 3-hour IV infusion every 3 weeks administered in combination with capecitabine 1,331 mg/ m2/d in two divided doses is recommended for diseasedirected evaluations. From a mechanistic standpoint, further evaluations of capecitabine/paclitaxel regimens that are rationally designed to optimize favorable subcellular interactions are warranted. ACKNOWLEDGMENT This article is dedicated to the memory of Maura Kraynak. REFERENCES 1. Ishitsuka H, Miwa M, Ishikawa T, et al: Capecitabine: An orally available fluoropyrimidine with tumor selective activity. Proc Am Assoc Cancer Res 36:407, 1995 (abstr 2426) 2. Budman D, Meropol N, Reigner B, et al: Preliminary studies of a novel oral fluoropyrimidinecarbamate: Capecitabine. J Clin Oncol 16:1795-1802, 1998 3. Bollag W, Hartmann H: Tumor inhibitory effects of a new fluorouracil derivative: 5-Deoxy-5-fluorouridine. Eur J Cancer 16:427-432, 1980 4. Hartmann H, Bollag W: 58-Deoxy-5-fluorouridine: A new antineoplastic pyrimidine antimetabolite. J Suisse Med 110:1078-1080, 1980 5. Kono A, Hara Y, Sugata S, et al: Activation of 58-deoxy-5fluorouridine by thymidine phosphorylase in human tumors. Chem Pharm Bull 31:175-178, 1983 6. Takebayashi Y, Yamada K, Miyadera K, et al: The activity and expression of thymidine phosphorylase in human solid tumors. Eur J Cancer 32A:1227-1232, 1996 7. Takebayashi Y, Akiyama S, Akiba S, et al: Clinicopathologic and prognostic significance of an angiogenic factor, thymidine phosphorylase, in human colorectal carcinoma. J Natl Cancer Inst 88:1110-1117, 1996 8. Tanaka Y, Eda H, Fujimoto K, et al: Anticachectic activity of 58-DFUR in a murine tumour cachexia model, colon 26 adenocarcinoma. Cancer Res 50:4528-4532, 1990 9. Ishikawa T, Ura M, Yamamoto T, et al: Selective inhibition of spontaneous pulmonary metastasis of Lewis lung carcinoma by 58DFUR. Int J Cancer 61:516-521, 1995 10. Bajetta E, Colleoni M, Di Bartolomeo M, et al: Doxifluridine and leucovorin: An oral treatment combination in advanced colorectal cancer. J Clin Oncol 13:2613-2619, 1995 11. Di Bartolomeo M, Bajetta E, Somma L, et al: Doxifluridine as palliative treatment in advanced gastric and pancreatic cancer patients. Oncology 53:54-57, 1996 12. Alberto P: Phase II study of an oral combination of doxifluridine, prednimustine and idarubicin (FUPRIDA) for first line treatment of advanced breast cancer. Ann Oncol 4:423-425, 1993 13. Ishikawa T, Utoh M, Sawada N, et al: Xeloda (capecitabine): An orally available tumor-selective fluoropyrimidine carbamate. Proc Am Soc Clin Oncol 16:208a, 1997 (abstr 727) 14. Schuller J, Cassidy J, Reigner B, et al: Tumor selectivity of Xeloda in colorectal cancer patients. Proc Am Soc Clin Oncol 16:227a, 1997 (abstr 797) 15. Mackean M, Planting A, Twelves C, et al: A phase I and pharmacologic study of intermittent twice-daily oral therapy with capecitabine in patients with advanced and/or metastatic cancer. J Clin Oncol 16:2977-2985, 1998 16. Taguchi T, Ishitani, K, Saitoh K, et al: A Japanese phase I study of continuous twice daily treatment with capecitabine in patients with advanced and/or metastatic solid tumors. Ann Oncol 7:87, 1996 (suppl 1) (abstr 299) 17. Eda H, Fujimoto K, Watanabe S, et al: Cytokines induce thymidine phosphorylase expression in tumor cells and make them PHASE I STUDY OF PACLITAXEL AND CAPECITABINE more susceptible to 5’-deoxy-5-fluorouridine. Cancer Chemother Pharmacol 32:333-338, 1993 18. Eda H, Fujimoto K, Watanabe S, et al: Cytokines induce uridine phosphorylase in mouse colon 26 carcinoma cells and make the cells more susceptible to 58-deoxy-5-fluorouridine. Jpn J Cancer Res 84:341347, 1993 19. Sawada N, Ishikawa T, Fukase Y, et al: Induction of thymidine phosphorylase activity and enhancement of capecitabine efficacy by Taxol/Taxotere in human cancer xenografts. Clin Cancer Res 4:10131019, 1998 20. Bogdan C, Ding A: Taxol, a microtubule stabilizing antineoplastic agent, induces expression of tumor necrosis factor alpha and interleukin-1 in macrophages. J Leuk Biol 52:119-121, 1992 21. Rowinsky E, Donehower R: Paclitaxel (Taxol). N Engl J Med 332:1004-1114, 1995 22. National Cancer Institute: Guidelines for Reporting of Adverse Drug Reactions. Bethesda, MD, Division of Cancer Treatment, National Cancer Institute, 1988 23. Royer I, Alvinerie P, Armand J, et al: Paclitaxel metabolites in human plasma and urine: Identification of 6 alpha-hydroxytaxol, 7-epitaxol and taxol hydrolysis products using liquid chromatography/ atmospheric-pressure chemical ionization mass spectrometry. Rapid Commun Mass Spectrom 9:495-502, 1995 1925 24. Reigner B, Verweij J, Dirix L, et al: Effect of food on the pharmacokinetics of capecitabine and its metabolites following oral administration in cancer patients. Clin Cancer Res 4:941-948, 1998 25. Gibaldi M, Perrier D: Noncompartmental analysis based on statistical moment theory, in Gibaldi M, Perrier D (eds): Pharmacokinetics (ed 2). New York, Marcel Dekker, 1992, pp 409-417 26. Eisenhauer E, ten Bokkel Huinink W, Swenerton K, et al: European-Canadian randomized trial of paclitaxel in relapsed ovarian cancer: High-dose versus low-dose and long versus short infusion. J Clin Oncol 12:2654-2666, 1994 27. Cresteil T, Monsarrat B, Alvinerie P, et al: Taxol metabolism by human liver microsomes: Identification of cytochrome P450 isoenzymes involved in its biotransformation. Cancer Res 54:386-392, 1994 28. Klaassen U, Wilke H, Harstrick A, et al: Paclitaxel in combination with weekly 24-hour infusional 5-fluorouracil plus leucovorin in the second-line treatment of metastatic breast cancer: Results of a phase II study. Ann Oncol 9:45-50, 1998 29. Bokemeyer C, Lampe CS, Clemens M, et al: A phase II trial of paclitaxel and weekly 24 h infusion of 5-fluorouracil/folinic acid in patients with advanced gastric cancer. Anticancer Drugs 8:396-399, 1997