Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
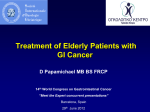
Working Beyond Cancer Dr Eliot Chadwick Consultant Clinical Oncologist Nottingham University Hospitals NHS Trust & The Nottingham Oncology Group Trent Occupational Medicine Annual Symposium 2014 Email: [email protected] Macmillan – the scene • In the UK, over 100,000 people of working age are diagnosed with cancer each year. • More than 700,000 people of working age are living with a cancer diagnosis. • The HR department of a large employer will see more new cancer diagnoses in a year than a GP. Cancer Incidence (CRUK) Cancer Incidence (CRUK) The Big 4 Cancer survival (CRUK) Cancer survival (CRUK) …and then there were 3 Why Toxicity? • Normal tissue reaction to chemotherapy and radiotherapy. • Relates to cell turnover. • Early vs late broadly correlates with α/β ratio Timelines - toxicity Long term Short term 4/52 8/52 6/12 20yrs The Return to Work Fear of relapse Pragmatism Denial Time DECISION Guilt Independence Empowerment Finance Self Employment Identity Self worth Breast Cancer • • • • • Surgery Chemotherapy Hormones Radiotherapy Biological agents (Herceptin®) Fatigue “...5 years after....I've been off sick from work since then...and, being completely honest, I have no desire of returning. I don't feel I can't work full time and, I can't survive on a part time wages. I have chronic fatigue, chemo brain and PSD. So far, nobody seems to care about the devastating effects of the aftermaths of cancer. The unrealistic expectations of employers, colleague and friends and, maybe my own, really puzzled me.” Longitudinal patient case rates for persistent fatigue over 12 months (n = 218). Goldstein D et al. JCO 2012;30:1805-1812 ©2012 by American Society of Clinical Oncology Lymphœdema Stiffness Pain BrCa Side effects ACUTE Peri-operative complications, seroma, infection Poor wound healing, infection, nausea, mucositis, alopecia Neuralgia, shoulder stiffness, fatigue Lymphœdema, cardiac, depression 6/52 3/12 2yr 10yrs 20yrs Prostate Cancer Risk of treating a non-lethal disease Success & morbidity of treatment Hormones LHRHa EBRT 3/12 6/12 18/12 2yrs 3yrs Hormones • Insulin resistance* / cardiovascular morbidity • ↓muscle mass • Cognitive impairment • Hot flushes *LGI diet advised (but see Pelvic RT) Hormones - summary • Effects as long as administered, and months to years beyond. • Probably underplayed. • Impact on occupation not necessarily direct. Pelvic Radiotherapy ACUTE Fatigue, *proctitis, cystitis, prostatitis nausea, skin reaction Pelvic RT effects EBRT CHRONIC / LATE *Proctitis, cystitis, arthritis, hip fracture 6/52 3/12 * ”Beige” diet advised 2yr 10yrs 20yrs Case 1 – 38yrs female, anal Ca Mitomycin C D1 EBRT 50.4Gy /28# 5-fluorouracil D1-4 Coronary artery spasm from 5-FU. D22-25 not given. 5.4Gy boost given in lieu. } At 18m, ongoing discomfort in perineum, frequency of stool 5-10/day, with urgency and occ. incontinence. Works at check-out in supermarket. Case 2 – 56yrs male, peri-anal Ca, vegetarian. Mitomycin C D1 5-fluorouracil D1-4, D22-25 Electron boost of 20Gy/10# } EBRT 50.4Gy /28# At 12m, ongoing discomfort in perineum, frequency of stool 5/day, with urgency. Struggles to maintain wt. Pre treatment, worked for council – refuse, gardens. Now medically retired. Radiotherapy - summary • Can cause significant long term effects. • Functional deficit. • Not easily treated. Chemotherapy Chemotherapy effects ACUTE Multiple, disparate effects. Not all intuitive. Fatigue, myalgia, arthralgia dysgeusia Wt gain, Neuropathy, cardiac 6/52 3/12 2yr 10yrs 20yrs Case 3 – 48yrs male, rectal Ca, node positive on MRI. Capecitabine 825mg/m2/bd + EBRT 50.4Gy / 28# Works in abattoir. Develops palmar-plantar erythema (PPE). Capecitabine stopped during RT. Post-op (stoma). Pathologically node positive. For further capecitabine + oxaliplatin adjuvantly. Pt declines oxaliplatin. Starts capecitabine, but stops early due to PPE. Case 4 – 65yrs male, colon Ca, Duke’s C Referred for adjuvant chemotherapy 5-fluorouracil / oxaliplatin q2/52 for 12 cycles. Loses sense of taste and smell. Develops PPE. Continues to work as Michelin star chef but finds it increasingly difficult. Chemo - Summary • • • • Most chemo effects acute. Fatigue most common long term. Subjective. Pts occupational circumstance may dictate chemo given. Surgery Surgery effects ACUTE Peri-operative complications Fatigue, poor wound healing, TED Anterior resection syndrome Hernia, stoma, incontinence 6/52 3/12 2yr 10yrs 20yrs Case 5 – 28yrs female, sigmoid Ca, emergency Hartmann’s. pT4b tumour Referred for adjuvant chemotherapy. Receives 8 cycles of capecitabine / oxaliplatin within SCOT study Regular FU post-chemo for SCOT data collection. Regular discussion regarding stoma. Pt works in clothes shop. Gaining weight, as finds it difficult to exercise. Stoma reversal on hold until 1 year CT performed. 1 year CT ?Ovarian mass Surgery - summary • Surgery usually irreversible. • Implications for lifestyle should be explored, particularly if options available. • Can have significant body image as well as functional effects. Are we doing enough? Challenges • Patients not informed about impact of cancer on their working lives. • Many patients do not have access to vocational rehabilitation services. • Employers don’t know how to support staff with cancer. • (Cancer specialists don’t know how to support employers.) Questions?