Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
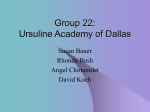
988 Flow through Collapsible Tubes at High Reynolds Numbers CAROL K. LYON, JERRY B SCOTT, DONALD K. ANDERSON, AND C.Y. W A N G Downloaded from http://circres.ahajournals.org/ by guest on June 16, 2017 SUMMARY The pressure-flow relationships of collapsible tubes were studied utilizing the Starling resistor model. Reynolds numbers much higher than previously reported were used to simulate high cardiac output states. Alterations which occur in vivo, including longitudinal tension, stretch, tubing diameter, length, and outflow resistance were also simulated and systematically investigated. The pressure-flow curves showed an initial rising phase, a plateau phase, as well as a late-rising phase which has not been reported previously. Self-induced oscillations occurred during the plateau phase and persisted throughout the late-rising phase. These perturbations were markedly increased by longitudinal tension and stretch, but were attenuated by increased diameter, length, and outflow pressure. These instabilities may prove to be an explanation for the "venoiia hum." Circ Res 49: 988996, 1981 VEINS are non-self-supporting structures that collapse when a critical transmural pressure is reached. Collapse of a vein greatly increases its resistance to flow, so that when collapse occurs, a non-linear pressure-flow relationship results. Forty years ago, Holt (1941) resorted to the use of a Starling resistor model to investigate and demonstrate the mechanics of the non-linear pressure-flow relationship of the inferior vena cava. His technique introduced into vascular research the use of a physical model which obviated many of the experimental difficulties encountered with in vivo venous research. The Starling resistor model has subsequently been adopted by many investigators to demonstrate the principles underlying the pressure-flow relationships which they have observed for various collapsible vessels: Brecher et al. (1952), the superior vena cava system; Swann et al. (1952), intra-renal venous pressures; Doppman et al. (1966), radiographic appearance of vena cava collapse; Rodbard et al. (1971), the vasculature of contracting muscle; Lopez-Muniz et al. (1968), the pulmonary circulation; and Fung and Sobin (1972), the pulmonary microcirculation. For all of these investigators, physical modeling has proven to be an important means of quantifying pressure-flow relationships and investigating the mechanisms of vascular collapse. In a previous paper (Lyon, Scott and Wang, 1980), we have shown that the flow properties of collapsible vessels depend heavily on the Reynolds number. This is a measure of the importance of the From the Department of Physiology, Michigan State University, East Laming, Michigan. This investigation was supported in part by a grant from the Michigan Heart Association, and by National Institutes of Health Grants HL10879 and HL243S3. Presented in part at the 62nd Annual Meeting of Fed. Am. Soc. Eip. Biol at Atlantic City, 197a Address foi reprints: Jerry B Scott, Department of Physiology, Michigan State University, East Lansing, Michigan 48824 Received December 17, 1980: accepted for publication June 5, 1981. inertial forces relative to the importance of viscous forces in determining flow properties. In the microvasculature, the Reynolds number is much less than one, and so viscous forces take predominance over the inertial forces. However, in vessels of larger diameter, such as arteries and veins, where the Reynolds number is large, inertial forces greatly influence the pressure-flow relationships. The experiments of Conrad (1969), Katz et al. (1969), Moreno et al. (1969), and our laboratory (Lyon et al., 1980) show that the properties and pressure-flow relationships of flow through collapsible vessels at high Reynolds numbers differ from those of the "waterfall model" of Permutt et al. (1962). The waterfall model predicts a total cessation of flow at low inflow pressures not observed by the above researchers. Flow at high Reynolds numbers also shows marked unsteady self-induced oscillations which have a significant effect on the pressure-flow relationships. The waterfall model as originally presented by Permutt et al. (1962) was an approximation of flow through the canine pulmonary micro vasculature. Such flow is described by low Reynolds numbers. Our data (Lyon et al., 1980) showed that when the Reynolds number is low enough to simulate the microcirculation, flow properties of the waterfall model are achieved. This result is indifferent to the mechanical properties of the collapsible tube, tube size, or the method of tube mounting. The purpose of the present research is to study flow through collapsible vessels with particular emphasis on the following areas which have not been investigated previously: 1. Pressure-flow relationships at high flow rates and Reynolds numbers. The maximum Reynolds number for previously published experiments is less than 1400. This may be adequate to model blood flow in the vena cava of resting man (Reynolds number = 900) and the dog (Reynolds number = FLOW THROUGH COLLAPSIBLE TUBES: HIGH REYNOLDS NUMBERS/Ljyon et al. Downloaded from http://circres.ahajournals.org/ by guest on June 16, 2017 1375) (Cooney, 1976). However, cardiac output and, consequently, the corresponding Reynolds number, may increase to five or six times the resting level during exercise (Wexler et al., 1968). 2, The effects on the pressure-flow relationships of tubing diameter, length, tension, and stretch of the conducting vessel. Both diameter and length of collapsible veins vary greatly within the human body. When the body is at rest, veins are subject to constant longitudinal tension due to their anatomical tethering to organs within the body (Moreno et al., 1970), but they must also stretch to accommodate body movement. Therefore, these parameters were also systematically investigated. 3. Significance and quantification of the selfinduced oscillations of the tubing. Rodbard (1953) proposed that such oscillations were the source of arterial sounds. In consideration of the phenomena of audible venous "hums" and palpable venous "thrills" (vibrations) during conditions of high cardiac output, these osculations may be clinically significant in the determination of venous blood flow patterns. Methods In accord with previous investigations, we used the "Starling resistor" to study the flow through collapsible vessels. The experimental apparatus was very similar to that used in a previous study (Lyon et al., 1980). The physical model (Fig. 1) consisted of flexible latex Penrose tubing (American Hospital Supply) enclosed in an 8,000-ml airtight transparent Plexiglas box. The Penrose tubing was 1.27 cm in diameter when expanded, 7.5 cm long, and had a wall thickness of 0.032 cm. Within the box, the tubing was mounted at both ends upon rigid cylindrical metal tubes with an inner diameter of 1.27 cm and a wall thickness of 0.05 cm. The tubing was mounted horizontally with no longitudinal stress applied unless otherwise noted. Pressure taps for the measurement of inflow pressure (P,) and outflow pressure (Po) were located outside the box on the metal tubing, 8.5 cm from either end of the collapsible tube. Pressure within the box external to the tubing (P.) was modified by the use of a pump connected by latex tubing to a port in the box. The cannula used to measure P e was inserted into the box through an airtight opening in the box. Pe, Pi, and Po pressure measuring cannulas were polyethylene tubing (PE 60), 80 cm long, filled with distilled water. Each was connected to a separate Statham low volume displacement transducer (P23Gb, Hato Rey) which was coupled to a Hewlett-Packard (7796 model 1065C) direct-writing oscillograph and Esterline Angus X-Y recorder (model 575). All pressure transducers were calibrated against a mercury manometer. The HewlettPackard electronic average was used for all pressure-flow measurements. Oscillations of the tubing were quantified for pressure amplitude and fre- RECORDER 989 X-Y PLOTTER PUMP DAMPER ho FLOW METER COLLAPSIBLE TUBE AIR-TIGHT BOX PUMP BASIN FIGURE 1 A schematic diagram of the experimental "Starling resistor" model which consisted of a collapsible latex Penrose tube mounted within an airtight Plexiglas box. Pressure ports for the measurements of inflow pressure (PJ and outflow pressure (PJ were located just outside the box on the mounting tubing. The pressure in the box (Pe) was modified by a hand pump connected to a port in the box. When water was pumped through the collapsible tube, pressure measurements and flow (Q) were charted by the recorder, and pressure differences (P,-Pa and P*-PJ were computed and graphed by the XY plotter. A l.S-ml latex bulb was used to dampen the pulse of the Po measurements. quency by use of the Hewlett-Packard electronic high filter setting and expansion of the time scale. The pressure catheter-transducer-recorder system was tested on high filter setting according to the method of Glantz and Tyberg (1969) and found to have an undampened natural frequency response of 33 Hz. Resistances upstream and downstream to the pressure ports (R, and Ro), were controlled by screw clamps on latex tubing, 1.2 cm i.d. This latex tubing opened above an outflow reservoir 8.5 cm distal to the P o port and, when completely open, produced minimal outflow resistance (approximately 1 mm Hg/80 ml per sec). Ro was elevated only when stated, by tightening the screw clamp on the outflow tubing so that it formed a near elliptical crosssection, the size of which was recorded as the diameter of its inner minor axis. Two of the components of the phenomenon of stretch, the effects of longitudinal tension and the effects of changes in vessel length, were investigated independently. The length of the collapsible tubing was taken as the measured separation of the mount- CIRCULATION RESEARCH 990 Downloaded from http://circres.ahajournals.org/ by guest on June 16, 2017 ing tubes within the airtight box. By definition, longitudinal tension was the force tending to cause longitudinal deformation (stretch) of the collapsible tubing. To study the effects of longitudinal tension, we applied tension to the tubing during the process of mounting, and shall refer to this initial tension as applied tension. The effects of longitudinal tension were isolated by keeping the separation of the mounting tubes (length) constant but mounting the collapsible tubing at varying levels of applied tension. On the other hand, the effects of vessel length were isolated by decreasing the distance between the mounting tubes in 1-cm decrements and shortening a section of Penrose tubing accordingly so that there was no applied tension on the collapsible tube. Finally, the simultaneous effects of applied tension and the resultant changes in length (stretch) were investigated by mounting a 4.5-cm length of tubing with no applied tension, then increasing the distance between the mounts by 0.5or 1.0-cm increments. This operation increased both tension and length. To determine the effect of changes in diameter, Penrose tubing 0.635 cm in diameter and 3.25 cm long, was mounted on rigid metal tubes that were 0.635 cm in diameter. This maintained the same length: diameter ratio that had been used for the larger (1.27 cm in diameter) Penrose tubing. A pressure-dependent centrifugal pump (Little Giant Pump Company) capable of delivering from less than 1 ml/sec up to 80 ml/sec of virtually nonpulsatile flow was employed to recirculate room temperature water through the system. The resistance R, served to modify the flow rate (Q). Q was measured upstream to the P, port by a flow-through flow probe connected to a Pulsed Logic Flowmeter (Biotronex Laboratory, Inc.), also coupled to the oscillograph and X-Y recorder. The zero flow set- '0 20 VOL. 49, No. 4, OCTOBER 1981 ting was obtained by stopping the pump and waiting for stabilization; calibration was obtained from 15second timed outflow collections that demonstrated a linear response. Zero drift was less than 0.1 ml/ sec during the time necessary to plot a curve, and the zero flow setting was checked immediately before initiating flow. Calibration checked at the end of the experiments was found to vary less than 1%. Because there were high amplitude fluctuations of P o when the Penrose tube oscillated, a "Windkessel" chamber was used to dampen the pulse in the P o measurements. It consisted of a 1.5-ml waterfilled latex bulb chamber connected in series by a T-tube to the pressure transducer tubing at its junction with the P o cannula. This compliance chamber was tested at low amplitude fluctuations (±10 mm Hg), and its use resulted in the same mean pressure as when the Hewlett-Packard electronic mean was used alone. Changes of volume of the Penrose tube resulted in minimal changes in P e (maximum of ±1 mm Hg). The method of experimentation used in this study was to initiate a low flow rate through the system. Pressure in the box was held at a predetermined level of P.-Po for each curve. All data points were graphed immediately via the X-Y recorder, which also served as an analog computer of P,-Po and Pe-Po. The pressure-flow relationships were obtained by plotting Q as a function of Pi-Po and Pe-Po, as explained in a previous paper (Lyon et al., 1980). Results A typical graph of the pressure-flow relationships of Penrose tubing (1.27 cm in diameter, 7.5 cm long) ia presented in Figure 2. For many of these curves, there are three distinct phases: an initial sharp- 40 60 Q cc/sec FIGURE 2 A typical graph of the pressure-flow relationships of the collapsible tube, 1.27 cm in diameter, 7.5 cm long. For these curves, P.-Po was held constant at 50, 30, 20, 10, and 5 mm Hg, respectively. Maximum Reynolds number achieved was 6,000. There are three distinct phases represented: an initial rising phase at low Q, a plateau phase at moderate Q, and a late rising phase for Q > 20 ml/sec. FLOW THROUGH COLLAPSIBLE TUBES: HIGH REYNOLDS NUMBERS/Z/yon et al. 991 1 The Effect of Pr-Po and Flow on Frequency and Pressure Amplitude of Oscillations TABLE 50 ml/sec 16 ml/sec P.'Po (mm Hg) Amplitude (mm Hg) Frequency (Hi) P,-Po (mmHg) Amplitude (mm Hg) Frequency (Hi) P.Pe (mm Hg) 0 10 30 50 0 1 1 1 0 5.5 10.5 14.5 1.4 110 31.5 50.7 31 16 1 1 5 25 7.0 10.25 13.0 11.0 16.8 33.6 52.9 Downloaded from http://circres.ahajournals.org/ by guest on June 16, 2017 affected both the initial and late-rising phases. During the initial rising phase, the shortest (2.5 cm) length of tubing was held partially open by the end constraints, resulting in a very low pressure gradient for flows less than 25 ml/sec. For this length, no oscillations, only a four-lobed constriction, was noted at all flow rate3. The effect of the end constraints was also apparent in the initial rising phase of the curve for the 3.5-cm segment of tubing. The pressure difference (P,-Po) of the late-rising phase reached a maximum at a length of 5.5 cm, and for lengths greater than 5.5 cm, the slope of the late rising phase was less. Representative data for the effect of vessel length on frequency and pressure amplitude of oscillations is presented in Table 2. Two sets of curves representing the effects of longitudinal tension are shown in Figure 5. Applied tension decreased the slope of the initial rising phase, but increased the oscillations and the slope of the late-rising phase. Representative data of the effect of longitudinal tension on frequency and pressure amplitude of oscillations is presented in Table 3. The effect of stretch was quantified by taking a 4.5 cm length of tubing, and stretching it to 5.5, 6.5, 7.5, 8.5, and 9 cm. Whereas, for the previous experiments, the pressure-flow relationships were extremely consistent, the results obtained for stretch were less so, and indicated that the effects of length rising phase, a plateau phase, and a late-rising phase of lesser slope than the initial rising phase. At flow rates of less than 6 ml/sec (the initial rising phase), the tube was collapsed flat except for two small round side channels. As flow approached 6-8 ml/sec, the flattened area gradually receded until only the outflow region of the tube appeared to be "pinched" closed, and the tube began to open and close intermittently (the plateau phase). During the plateau phase, P,-Po stabilized at approximately the level of Pe-Po. At flows greater than 20 ml/sec, the curves again began to rise. This late-rising phase occurred at higher flow rates for higher Pe-Po. The Reynolds number for this data, based on tubing diameter, maximum flow rate, and average velocity of flow, increased linearly with flow to a Reynolds number of 6,000 at a flow rate of 60 ml/sec. The amplitude of the pressure fluctuations caused by the self-excited oscillations increased during the late rising phase (Table 1). With Pe-Po held constant, increasing R^ had the effect of increasing the value of all pressure measurements. This outflow resistance reduced the frequency and the pressure amplitude of the oscillations, and decreased the slope of the late rising phase. A graph of a representative experiment at p e .p o = 10 mm Hg is shown in Figure 3. An experiment using different lengths of tubing resulted in the gTaph of Figure 4. Changes in length 40 X E E I 20 4O 20 Q 60 CC/sec 3 A graph of a representative experiment using high, moderate, and no applied outflow resistance (RJ at constant P.-Po = 16 mm Hg. Ro decreased the frequency and pressure amplitude of the self-induced oscillations, and decreased the slope and the resistance of the late rising phase. FIGURE CIRCULATION RESEARCH 992 VOL. 49, No. 4, OCTOBER 1981 20 0 20 40 Q 60 cc/sec 4 Representative results of an experiment using different lengths of tubing at constant Pr-P,, = 16 mm Hg. The shorter lengths of tubing were held partially open by the openings of the rigid mounting tubes, resulting in low pressure gradients for flows < 25 ml/sec. The slope and the resistance of the late rising phase were maximal at a length of 5xh cm. The slope of the late rising phase was decreased for lengths greater than 5V> cm. FIGURE Downloaded from http://circres.ahajournals.org/ by guest on June 16, 2017 and tension were not additive. Therefore, a statistical analysis was undertaken (Table 4). At high flow rates, the resistance increased as the tube was stretched from 4.5 to 7.5 cm. When stretched to 7.5 cm, the tube existed in either of two distinct states: a high resistance state of vigorous oscillations, or a lower resistance state of decreased oscillations. When stretched to 8.5 cm and 9 cm, the resistance of the tube increased incrementally from its lower resistance state at 7.5 cm. Analysis of variance was performed on the raw data of the stable stretched lengths. Tukey's multiple comparisons between all stable means proved significant (P < 0.05). Table 5 summarizes the data obtained from a representative experiment. It shows that stretch increased the pressure amplitude of the oscillations. The results for water perfusion of the smaller Penrose tubing, 0.635 cm in diameter, 3.25 cm long, demonstrated an interesting effect of tubing diameter (Fig. 6). Compared to the tubing that was 1.27 cm in diameter, the initial rising phase of the curves was steeper, and the plateau phase began at lower flow rates. Oscillations of the tubing were noted at the beginning of the plateau phase, and they continued as flow was increased. The steep curve of the late-rising phase also began at lower flow rates. The maximum Reynolds number for water perfusion of this smaller Penrose tubing for flow of 20 ml/sec was 4,000. TABLE 2 Discussion The use of the Starling resistor model to describe pressure-flow relationships avoids the biological inconsistencies that are encountered during in vivo research of collapsible blood vessels. Because flow rates and experimental pressures, especially tissue pressure, are extremely difficult to maintain and reproduce from one animal experiment to the next, only a statistical quantification of these puzzling relationships can be established in vivo. The Starling resistor model has proven to be a reliable tool that can be used to quantify these relationships so that the underlying mechanisms of blood flow through collapsible vessels can be better understood. For this research, we have used a segment of Penrose tubing as the collapsible tube. The reasons are as follows: (1) Penrose tubing has been used to study the properties of collapsible vessels during the past 40 years. Thus, its use facilitates the comparison of our data with previous results. (2) The elastic properties of the Penrose tube do not change with time, whereas in vitro vein segments perfused with artificial medium deteriorate progressively. (3) The experimental results using the Penrose tubing are highly reproducible. In recent careful experiments, Baird and Abbott (1977) compared the elastic properties of various The Effect of Vessel length on Frequency and Pressure Amplitude of Oscillations (P<-Pa = 16 mm Hg) 75 ml/sec 27ml/»ec Length (cm) Frequency (Hz) Amplitude (mm Hg) P.P. (mm Hg) Frequency iHx) Amplitude (mm Hg) 2.5 4.5 5.5 6.5 7.5 10.5 13.5 0 0 0 0 1 3 1.5 2 2 16 18 18.5 19 18 17.5 0 11 12 12 11.5 8 9 0 7 26 24 25 28 16 0 0 8 8 8 8 PrPo (mm Hg) 16 24 43 41 39 31.5 27 FLOW THROUGH COLLAPSIBLE TUBES: HIGH REYNOLDS NUMBERS/L>orc et al. 993 40r Downloaded from http://circres.ahajournals.org/ by guest on June 16, 2017 O 20 40 Q 60 cc/sec FIGURE 5 The effect of longitudinal tension at constant Pr-P0 = 16 mm Hg. Penrose tubing with a manufactured length of' 4h cm was placed on mounting tubes positioned 7M> cm apart. The curve generated by this tubing is labeled 4Vi + 3 cm, and should be compared to the curve labeled 7M>, the tubing of which had no applied tension. The curve labeled l&h + 3 also demonstrates the effect of longitudinal tension when compared to that labeled 13lh. Applied tension decreased the slope of the initial rising phase, but increased the elope of the late rising phase. creases so that it is less likely to collapse. The slope was increased by decreasing the transmural pressure or the length of the vessel. It is probable that for small veins, which are less compliant because their wall thickness-to-diameter ratio is greater, the initial rising phase would be present. During the plateau phase (P, > P e > Po), low amplitude oscillations of the tubing occurred. In this phase, resistance decreased remarkably as Q increased. The use of increased R, served to decrease these oscillations and prolong the plateau phase. Interestingly, the plateau phase always occurred at approximately Pi-Po = Pe-Po, even with the use of various types of Penrose tubing. The major effect of our experimental maneuvers upon the plateau phase was to modify the flow rates during which this phase occurred. At higher flow rates, the experimental graphs show a late rising phase not previously reported by other researchers. It is characterized by a distinct collapsible vessels. It was found that Penrose tubing possesses a linear stress-strain relationship, whereas that of veins is non-linear. However, the Young's modulus (slope of the stress-strain curve) of the Penrose tube closely approximates that of the polytetrafluoroethylene (PTFE) synthetic graft used clinically, and also those of the femoral vein and carotid artery at high strains. Thus the results of our experiments apply qualitatively to in vivo situations. The pressure-flow relationships of the Penrose tubing Starling resistor model show that at low flow rates, where P e > Pi > Po, the initial steep slope and high resistance of the curves increased as the parameter Pe-Po increased. These data confirm the findings of Conrad (1969), Katz et al. (1969), and Moreno et al. (1969). The slope of the initial rising phase was decreased by increasing longitudinal tension or stretch of the vessel. This occurred because, when the vessel is pulled taut, its compliance de- TABLE 3 The Effect of Applied Tension on Frequency and Pressure Amplitude of Oscillations P,-P. - 16 mm Hg Manufactured Experimental length length (cm) (cm) 13.5 10.5 10.5 7.5 7.5 4.5 13.5 13.5 10.5 10.5 7.5 7.5 Flow r»U - 75 ml/sec Frequency (Hi) Amplitude (mm Hgl 8.8 8.5 29 63 38 9.3 10.1 10.8 11.2 43-68 20-30 52-54 Pi-P. (mm Hg) 27.0 300 31.0 415 33.0 64.5 CIRCULATION RESEARCH 994 VOL. 49, No. 4, OCTOBER 1981 TABLE 4 The Effect of Stretch on Resistance (n - 25) P.-Pp - 16 mm Hg Flow rate m 74 ml/sec Manufactured length (cm) Experimental length (era) Mean Pi-P. (mmHg) P,-Po (mm Hg) Resistance (mm Hg/ml per set) 4.5 4.5 45 4.5 45 4.5 25.9* 38.5* 56.1* 42.0* 43.9* 2.4 2.5 3.2 1 6 0.9 0.35 0.52 0.76 0.57 0.59 5.5 6.5 8.5 9.0 SD • P < 0.05, Tukey's multiple comparison- Downloaded from http://circres.ahajournals.org/ by guest on June 16, 2017 stream influence cannot propagate upstream beyond the "pinched" segment of the collapsible tube. This theory has been challenged recently by the experiments of Conrad et al. (1978). Still another method of analysis assumed a slowly varying crosssection of the tube, such that the viscous Poiseuille's law can be applied to the "pinched" section of tubing. This assumption was used by Rubinow and Keller (1972) for the circular tube, Wild et al. (1977) for the elliptic tube, and Brower and Noordergraaf (1978) for the rectangular tube. However, only the time-independent first and second phase can be obtained by this method. Since these various theories axe based on conflicting principles and because none predicts the late-rising phase, it appears that the theory of flow in collapsible tubes at high Reynolds numbers remains controversial and incomplete. Finally, we would like to comment on the physiological implications of our study. In all of our experiments except one, low outflow resistance and low outflow pressure were used. This is similar to the hemodynamics of venous flow into the low pressure system of the thorax and atria. The one experiment in which outflow resistance was applied to increase P o represents less physiological states, such as heart failure, pericardial tamponade, or the Valsalva maneuver. The collapsible tubing was connected to rigid mounting tubes which may be considered to represent the anatomical tethering that tends to hold blood vessels open. Examples of anatomical tethering are the junctions of the venae cavae and the right atrium. The non-collapsible venous sinuses of the brain and the blood vessels within the bones also serve as anatomical tethering increase in oscillations as well as an increase in slope. The oscillations have been noted by previous investigators, but their systematic quantification has remained elusive until now. In general, our experiments show that the amplitude of the oscillations increases when there is an increase in flow, tension, and/or stretch. The amplitude of the oscillations is decreased by increasing P e -P o or increasing Ro and PQ. The effect of tension, length, and stretch on the frequency of the oscillations is variable. The late-rising phase is more prominent with experimental manipulations that increase the amplitude of the oscillations: low Pe-Po, low P o resulting from low Ro, increasing tension, and increasing stretch. The slope of the late-rising phase represents a relative constancy of resistance. Although we cannot rule out the development of turbulence as a mechanism for the late-rising phase, dye injections failed to demonstrate this. There have been several theoretical attempts to describe the flow in collapsible tubes at high Reynolds numbers. Approximation of the system by lumped parameters (resistors, capacitors, inductors, and nonlinear elements) was done by Conrad (1969), Kresch and Noordergraaf (1969), Katz et aL (1969), and Mahrenholtz (1974). Some success was obtained in the explanation of the early rising phase and the oscillations of the plateau phase. A completely different approach was taken by Lambert (1969), Griffiths (1975), Oates (1975), and Shapiro (1977), who assumed essentially one-dimensional inviscid flow. By using a compressible flow analogy, they theorized a critical speed (possibly related to the self-induced oscillations) above which down- TABLE 5 The Effect of Stretch on Frequency and Pressure Amplitude of Oscillations P,-P. - 16 mm Hg Flow rau =• 7S ml/sec Manufactured length (cm) Experimental length (cm) Frequency (cm) Amplitude (mm Hg) P.-P. (mm Hg) 4.5 4.5 4.5 4.5 4.S 4.5 4.5 4.5 5.5 6.5 7.5 7.5 8.5 9.0 11 10.25 12.25 11.25 9.7 11 4.1 6-S 24-30 68 47 9-26 12-47 7-50 26.8 33.5 63 51.8 33.3 40 44.3 FLOW THROUGH COLLAPSIBLE TUBES: HIGH REYNOLDS NUMBERS/Lyonetal. )40 7 E E a? ©30 ; ry Downloaded from http://circres.ahajournals.org/ by guest on June 16, 2017 \tz. 0 / y 20- i 5 995 P20 P _______O10 i 10 Q 15 20 25 cc/sec FIGURE 6 The effect of tubing diameter. The diameter of this tubing was 0.636 cm, tubing length was 3.25 cm, and the same length: diameter ratio was maintained as that of the larger collapsible tube shown in Figure 1. The pressureflow relationships were tested at Pr-Po of 40, 30, 20, and 10 mm Hg, respectively. The transitions between the three phases occurred at much lower Q and the slopes were much steeper than those of the larger diameter tubing. At Q = 20 ml /sec, the Reynolds number was 4,000. The initial rising phase, the plateau phase and the late rising phase were very distinct. tending to hold open the veins that lead away from them. An example of a venous system that is held open at either end is the jugular-subclavian-vena cava system. The flow rates of the third phase are representative of flow through the great veins when cardiac output is high. The self-induced oscillations may be representative of the "venous hum" that is often auscultated during high cardiac output states (Hardison, 1975). Probably the most commonly auscultated, although often unrecognized, venous hum is produced by the cervical veins (Cutforth et al., 1970). If we examine the dynamics of the production of this sound, it can be seen that the parameters of venous pressure and flow concur with those of the late-rising phase of our study: This "murmur" is best heard with the patient in the upright position (low Po), and usually disappears when the patient is recumbent, when light finger pressure is placed over the vein at its entrance into the thorax, and during a Valsalva maneuver (increased Po). Hardison (1975) reported that it ie loudest during diastole and inspiration (decreased Po), and when the head is extended and turned away from the examining side (stretching of the vein being auscultated). By analysis of the expected values of the various pressures and flow in each of these sound-producing situations, one finds that Pi > P e > Po, and P o is very low or possibly negative. Therefore, it is not unreasonable to expect that, in all of these instances, the walls of the veins may be oscillating or vibrating as in our model. Cutforth et al. (1970) devised a physical model to duplicate the production of the venous hum. Dye injections demonstrated turbulent flow when the hum was reproduced in the model, but his use of relatively noncompliant polyethylene tubing obviated the possibility of non-turbulent oscillations such as we observed with the collapsible Penrose tubing. However, the possibility that oscillatory movement of the venous walls may be a factor in the production of the cervical venous hum is given additional credence by the experimental observations of Brecher et al. (1952). In their study of the effects of respiration on venous collapse of the canine superior vena cava system, they observed "vibratory oscillations" of canine jugular veins, as well as of their physical model. In certain instances venous vibrations are also palpable. A continuous venous "thrill" (palpable vibratory phenomenon) accompanied by a "bruit" (auscultatory phenomenon) is helpful in establishing the diagnosis of an arteriovenous fistula (Young and deWolfe, 1978). A venous hum is indicative of systemic pathology when heard over the paraumbilical veins (Ramakriflhnaii, 1978). Interestingly, Cutforth et aL (1970) found that a hum could be auscultated over the femoral veins when individuals were tilted in a 45° head-down position. Further study of this phenomenon in human subjects is now possible with the use of newer, more sophisticated non-invasive clinical techniques. CIRCULATION RESEARCH 996 Downloaded from http://circres.ahajournals.org/ by guest on June 16, 2017 It is possible that a better understanding of the femoral venous hum may lead to a simple bedside method for monitoring femoral venous flow patterns, which have been shown to be disrupted in the presence of thrombophlebitis (Young and de Wolfe, 1978). In conclusion, our studies have shown that the pressure-flow relationships of collapsible tubes for Reynolds numbers comparable to those of high cardiac output states are markedly affected by instabilities of flow. These instabilities include oscillatory phenomena and higher pressure gradients than are predicted by the waterfall model. Longitudinal tension and stretch markedly increased these instabilities. Increased diameter, length, and outflow pressure had the opposite effect. The pressure gradients were always greater than would be required for flow through the same vessel in the non-collapsed state. These instabilities markedly increase the resistance to flow through collapsible tubes and may prove to be an explanation for the venous hum. References Baird RN, Abbott WM (1977) Elasticity and compliance of canine femoral and jugular vein segments. Am J Physiol 233: H15-H21 Brecher GA, Mister G, Share L (1952) Dynamics of venous collapse in superior vena cava system. Am J Phyaiol 171; 194203 Brower RW, Noordegraaf A (1978) Theory of steady flow in collapsible tubes and veins, chap 27 In Cardiovascular System Dynamics, edited by J Bonn, A Noordergraaf. MIT Press Conrad WA (1969) Pressure-flow relationships in collapsible tubes. DEEE Trans Biomed Eng 16: 284-295 Conrad WA, Cohen ML, McQueen DM (1978) Note on the 08cilldtions of collapsible tubes. Med Biol Eng Comput 16: 211-214 Cooney DO (1976) Biomedical Engineering Principles, New York, Dekker, pp 72-73 Cutforth R, Wiseman J, Sutherland RD (1970) The genesis of the cervical venous hum. Am Heart J 80: 488-492 Doppman J, Rubinson RM, Rockoff SD, Vasko JS, Shapiro R, Morrow AG (1966) Mechanism of obstruction of the infradiaphragmatic portion of the inferior vena cava in the presence of increased intra-abdominal pressure Invest Radiol I: 37-52 Fung YC, Sobin SS (1972) Pulmonary alveolar blood flow. Circ Res 30: 47O-49O Glantz SA, Tyberg JV (1969) Determination of frequency response from step response: Application to fluid-filled cathetera Am J Physiol 236: H376-H378 Griffiths DJ (1975) Negative-resistance effects in flow through VOL. 49, No. 4, OCTOBER 1981 collapsible tubes- Med Biol Eng 13: 797-801 Hardison JE (1975) The cervical venous hum: A help or a hindrance. N Engl J Med 292: 1239-1240 Holt JP (1941) The collapse factor in the measurement of venous pressure. Am J Physio! 134: 292-299 Katz A, Chen Y, Moreno A (1969) Flow through a collapsible tube: Experimental analysis and mathematical model. Biophys J 9: 1261-1279 Kresch E, Noordergraaf A (19O) A mathematical model for the pressure-flow relationship in a segment of vein. IEEE Trans Biomed Eng 16: 296-307 Lambert JW (1969) Closed form solutions for fluid flow in a thin walled tube buckled by a uniform external pressure. Int J Eng Sci 7: 963-971 Lopez-Muni2 R, Stephens N, Bromnerger-Bamea B, Permatt S, Riley R (1968) Critical closure of pulmonary vessels analyzed in terms of Starling resistor model. J Appl Physiol 24: 625635 Lyon CK, Scott JB, Wang CY (1980) Flow through collapsible tubes at low Reynolds numbers Circ Res 47: 68-73 Mahrenholtz O (1974) Zur pumpwirkung kollabier fahiger ventdasser Schlauche. Ing Arch 43: 173-182 Moreno A, Katz A, Gold L (1969) An integrated approach to the study of the venous system with steps toward a detailed model of the dynamics of venous return to the right heart. IEEE Trans Biomed Eng 16: 308-324 Moreno A, Katz A, Gold L, Reddy RV (1970) Mechanics of distention of dog veins and other very thin-walled tubular structures. Circ Res 27: 1069-1060 OateB GC (1975) Fluid flow in soft-walled tubes. Med Biol Eng 13: 773-780 Permutt S, Bromberger-Barnea B, Bane H <1962) Alveolar pressure, pulmonary venous pressure, and the vascular waterfall. Med Thorac 19: 239-260 Ramakrishnan T (1978) Venous hum of the Cruveilhier-Baumgarten syndrome. Letter to the Editor. Arch Intern Med 138: 826 Rodbard S, Saiki H (1953) Flow through collapsible tubes. Am Heart J 46: 715-725 Rodbard S, Handel N, Sadja L (19711 Flow patterns in a model of a contracting muscle. Cardiovasc Res 5: 396-404 Rubinow SI, Keller JB (1972) Flow of a viscous fluid through an elastic tube with applications to blood flow. J Theoret Biol 35: 299-313 Shapiro AH (1977) Steady flow in collapsible tubes. J Biomech Eng Trans ASME 99: 126-147 Swann HG, Hink BW, Koester H, Moore V, Prine JM (1952) The intrarenal venous pressure. Science 115: 64-65 Weiler L, Bergel DH, Gabe IT, Makin GS, Mills CG (1968) Velocity of blood flow in normal venae cavae. Circ Res 23: 349-359 Wild R, Pedley TJ, Riley DS (1977) Viscous flow in collapsible tubes of slowly varying elliptical cross-section J Fluid Mech 81: 273-294 Young JR, de Wolfe VG (1978) Diseases of the peripheral arteries and veins, chap 104. In The Heart, edited by JW Hurst. New York, McGraw-Hill Flow through collapsible tubes at high Reynolds numbers. C K Lyon, J B Scott, D K Anderson and C Y Wang Downloaded from http://circres.ahajournals.org/ by guest on June 16, 2017 Circ Res. 1981;49:988-996 doi: 10.1161/01.RES.49.4.988 Circulation Research is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1981 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7330. Online ISSN: 1524-4571 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circres.ahajournals.org/content/49/4/988 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation Research can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation Research is online at: http://circres.ahajournals.org//subscriptions/