Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
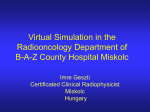
The Radiographer- vol. 49:141-146: Validating the use of Digitally Reconstructed Radiographs as Verification Tools in Radiation Therapy Simulation of Prostate Treatment J. Parker, 1 M. Vigar, 1 S. Dempsey, 1 H. Warren-Foiward, 1 & K. Jovanovich, 1•2 ABSTRACT Purpose: The aim of this study was to validate the clinical usefulness of Digitally Reconstructed Radiographs (DRRs) as a replacement tool for simulator verification films in prostate treatment. Method: The study was performed on a convenience sample of 13 patients who had all undergone or were currently undergoing prone treatment to the prostate and/or seminal vesicles. All patients received 60 or 66Gy in 30 or 33 fractions via a fourfield PA/AP, Lt. & Rt. lateral field technique using 6 or 18 MV photons. The previously acquired PA and lateral simulation films were collected for each patient and a set of DRRs produced from stored data. In total 26 DRRs were produced and these were compared to the 26 simulation films. In order_ to compare and identify variation between the image sets distance measurements were taken from a single bony landmark to the isocentre in the superior-inferior (sup-inf), left-right (lt-rt), and anterior/posterior (ant-post) directions. Results: In the sup-inf displacement a maximum difference of 0.4cm was ol)served (correlation coefficient of r = 0.96, p<0.001). In the lt-rt displacement a maximum difference of 0.3cm was observed (rr'= 0.89, p<0.001). In the ant/post direction an outlying difference of 0.8cm was recorded although 10 of 13 measurements were less than 0.3cm (r=0.94, p<O.OOl). Conclusion: A statistically significant correlation was found between the image sets. In terms of isocentre placement, DRRs within this study accurately represented the simulation verification film and may be considered as a clinically acceptable replacement for the current simulation verification film in prostate treatment. This outcome suggests that current clinical protocols could change to incorporate the increased use of DRRs as either aids in placing planned fi¢ld position within a verification simulator session or as a primary planning output replacing the current simulation verification session. This has implication for both the patient and the department. GT INTRODUCTION Images from modalities such as computed tomography (CT), magnetic resonance imaging (MRI) and positron emission tomography (PET), downloaded onto a radiation therapy planning system, can provide a 3D model of the patient's anatomy that allows more accurate identification of planning target volumes (PTV) and their relationship with organs at risk (OAR). Modern radiation therapy planning systems also facilitate the use of these images to create divergently correct digitally reconstructed radiographs, which can look similar to simulation images, and which can display volumes, field shape and isodose distributions.' Purdy (1997, p358)2 at the time defined digitally reconstructed radiographs (DRRs) as " ... computer generated projection images produced by mathematically passing divergent rays through a CT data set and acquiring X-ray attenuation information along the rays during 3D planning." Once I. Faculty of Medicine & Health Sciences, The University of Newcastle, Australia 2. Radiation Oncology, Mater Hospital, Newcastle, Australia Address for Correspondence: Mr Shane Dempsey, Box 16, ' Hunter Building, University of Newcastle NSW Australia Tel: +61 2 4921 6667 Fax: +61 2 4921 7053 E-mail: [email protected] econstructed, the DRR can serve as a reference image for transferring the 3D-treatment plan to the treatment machine. The DRR can replace the conventional simulator radiograph with a digital version obtained by arrangement of the CT voxels into a geometrically equi'\_l!lent planar view. It should be noted that the data set can include imaging modalities other than CT.,_. For clinical usefulness DRR images must give reasonable approximation- of true simulation images in terms of both spatial resolution and subject contrast so that multiple bony landmarks can be used to compare the DRR to a simulator or treatment verification image. 7 The increa&ing potential for clinical use of DRRs as a referenc'e image for treatment field and set-up verification can be explained through understanding the inherent advantages these images possess over current hard copy plain film images. ADVANTAGE 1: Because DRRs are directly derived from CT data their geometric accuracy, with respect the treatment plan, is not compromised by inaccuracies in the treatment simulation. An example of this is the reduction of manual judgement, or parallax error, in visually adjusting the treatment fields, via manual fluoroscopic movement as performed currently from the plan in the simulator verification session. ADVANTAGE 2: The DRR computation can be manipulated to change the appearance of the image to facilitate comparison with portal images. An application of this is where the DRR can be digitally manipulated to improve contrast or resolve anatomy by selectively removing overlying anatomical structures. ADVANTAGE 3: DRRs can be computed for arbitrary angles of projection through CT slices. This allows for quantification of patient rotation along axes parallel to the plane of the imag- The Radiographer- vo/.49, no. 3, December 2002 141 VALIDATING THE USE OF DIGITALLY RECONSTRUCTED RADIOGRAPHS ~. AS VERIFICATION TOOLS IN RADIATION THERAPY SIMULATION OF PROSTATE TREATMENT ing device, and out of plane rotations can then be verified. ADVANTAGE 4: With constant advancements in computing technologies, such as improvements in hardware processing and therefore faster computational ray tracing algorithms, DRRs are now produced within, clinically acceptable times. This study attempts to validate the clinical usefulness of DRRs as a replacement tool for simulator verification films. Prior to implementing into clinical practice emerging technologies, like DRRs, there is a need to validate the new technology or protocol against existing protocols to assess the outcomes, benefits and disadvantages of the technology or protocol. Validation studies are an important element of acceptance testing. Validation studies also allow the ethical considerations of the technology or protocol, ie. the real or perceived risks and benefits, to be considered in isolation of the rush to implement the new procedure into clinical practice. In this study comparisons were made between DRRs produced on the planning system and the films currently taken at the simulator verification session by compari!,lg the var.iation between the image sets. Variation was assessed as the distance measured from a single bony landmark to the intended treatment isocentre in the sup-inf, lt-rt, and ant-post directions.' If there is significant correlation between the image sets this may suggest that: 1. DRRs can be produced on the current planning system with comparable image quality to simulatpr radiographs making · _, comparison possible. 2. DRRs are valid and accurate tools for verifying isocentre location with respect to pelvic bony anatomy and may replace simulation verification images with respect to establishing the treatment isocentre location. 3. DRRs can be used as the reference image for treatment verification!;10 \ METHOD AND MATERIALS A convenience sample of 20 patients who were being treated, or had completed a radical course of radiation therapy to the prostate, or prostate and seminal vesicles, at the Mater Hospital Newcastle, were selected for this validation study on thf1 use of DRRs as a verification tool within a radiotherapy depj~rtment. To be considered eligible for the study all patients haq to positioned prone and have undergone a traditional4 field- PNAP & Rt/Lt lateral "box" technique. All patients received between 60Gy to 66Gy to the isocentre, (ICRU50 reference point) in 30 or 33 fractions, using 6 or 18 MV photons. ;. All patients had planning CT's performed u~ing a Seimens Somatron Plus 4 CT scanner. Each CT study consisted of 5mm thick contiguous slices through the intended treatment area from which volumes and plans where produced. All patients were planned using the ADAC Pinnicle' 3D planning system Version 5.0e, and all plans Right: Figure 1: · were produced prior to the · Three Dimensional Co-ordinate verific1,1tion simulation sesSystem. The x-axis represents sions. These plans, along with left-right displacements as the CT scout image, were used determined from the PA film. by radiation therapists to visuThe y-axis represents superiorally place the treatment fields inferior displacements as during simulation verification determined from the PA film. and these simulator verification The z-axis represents anteriorfilms were used for posterior displacements as subsequent comparison with determined from the lateral treatment verification images film. 142 The Radiographer- vol. 49, no. 3, December 2002 (port films). In assessing DRRs within this study prostate treatment was chosen for the following reasons: The prostate is generally a mid-sagittal plane structure, and isocentre localisation during simulation may vary from the planned isocentre position in sup-inf, lt-rt, and ant-post directions. This scope of possible movement in three dimensions will allow adequate quantification of the differences between the image sets. The surrounding bony anatomy in relation to the prostate is stable, with multiple bony landmarks from where measurements can be taken to compare the accuracy of the planned isocentre on the two images. Upon analysing the cases currently stored on the hospitals planning system, there were a sufficient number of prostate treatments to collect a pilot or validation study sample, and those selected should reasonably represent patients typically being referred for treatment to this centre. In assessing the completed plans for the most recent twenty prostate patients treated, seven patients were removed from the study. Three patients were ruled out because they were positioned supine, therefore comparisons of variability of anatomy position could not be made. Data from three patients were unable to be retrieved from the computer for technical reasons, and the data for one patient was incomplete at the time of the research. In all 13 patients were included in this study and 26 DRRs were produced, comprising one P;A and one lateral DRR per patient. DRRs were produced using the following parameters. For the PA DRR an energy of 0.0006 MeV and a brightness level of 0.6 to 0.8 was selected, and for the lateral DRR an energy of 0.0002 MV and brightness level of 0.5 to 0.8 was selected. These are average exposures and were yaried slightly depending on the size of the patient. (Note: Optimal DRRs are now produced using the default values on Pinnacle 6.2G). For visual comparison to the simulation films the DRRs were printed on plain paper using a Hewlett Packard Laser printer. The crosshairs and field outlines were left on for the purposes of the research. The anatomical reference points used for comparison y ----------~~~~~--------X z J PARKER, M. VIGAR, S. DEMPSEY, H. WARREN-FORWARD, K. JOVANOVICH tion therapy a value of (0.5cms has historically been used as the point at which image sets are thought to agree. With the shift to more conformal beam shapes and better patient immobilisation methods this value could realistically be reduced to s0.3cms or less. between the image sets were the right anterior aspect of symphysis pubis (RAASP) for the anterior films and the anterior aspect of the symphysis pubis (AASP) for the lateral views. Once the DRRs were produced the simulation verification films were located a~d distances from the isocentre to the anatomical landmarks on both image types were recorded on a worksheet and the difference between the image sets determined. The measurements on both images sets were considered in three dimensions as displayed in the Figure 1. This research was carried out over approximately a five month period as part of a supervised final year student research project. The researchers reviewed the planning records to identify a large enough pool of similar cases that could be used for the study, learnt to generate and optimise DRRs on the Pinnacle planning~ system, identified bony landmarks suitable for comparison, and learnt to use and interpret a statistical data base. The actual production of DRRs for all cases and measurement of differences between all image sets took 2-3 weeks and was dependent on the access to the planning system. It would be possible to perform the DRR production and measurements in a much shorter time frame if they formed part of the routine planning protocol. Basic data analysis was performed using Microsoft Excel. Assessment of how well the DRRs correlated with the simulation images was made on two levels. I. Statistical analysis: Scattergrams of the measured differences between images sets were generated and correlation coefficients and the associated p-values were determined for agreement in 1,1ll three directions separately. A correlation coefficient greater than 0.8 indicates a high level of correlation between the image sets. 2. Descriptive analysis: Bar Charts were generated that showed the actual agreement and differences between image sets. When comparing verification images in radia- RESULTS The comparison of the measured differences between the images sets in the sup-inf, lt-rt, and ant-post directions, demonstrated a statistically significant correlation between DRRs and simulation verification films for the purposes of isocentre localisation for prostate treatments. Given that the results displayed a similarly high level of correlation between the image sets in all three directions, individual results have been displayed only for the assessment of one set of images, the left to right displacements (Figures 2 & 3). Figure 4 displays the actual differences between images sets when all data is pooled or combined. Table 1 provides an overview of the levels of agreement and statisticaVpnalysis of the entire data set. Figure 2 cl1splays the differences between the DRRs and the simulator verification films in terms of lateral isocentre displacement from the anatomical bony landmark, measured from the AP/PAview. For five image sets (5 out of 13) the isocentre displac'iment between the DRR and the simulator verification film d~inonstrated 100% agreement. Twelve image sets (12 out of 13) had an overall difference (0.2cm with the maximum difference recorded being 0.3 em for one patient. These r.esults fall within the historic 0.5cm tolerance, which is generally accepted at the centre as being within clinical tolerances. Figure 3 is a scattergram plotting the left to right isocentre displacements for both imaging modalities. Correlation analysis demonstrates a high level of statistically significant agreement between the DRRs and the simulator radiograph (r = 0.89, p = <0.001). Figure 4 is a scattergram plotting the pooled isocentre ,. " 0.8 0.7- e ~ ~ - D Radiograph [i] ORR 0.6- s::: - Q) u u 0 -';; ,--c- 0.5- - . .!!!. E -- 2 0.4s::: Q) ,- ,-~ ,- 1'\ 0.3E Q) u (/) ~ ;:'] 11:1 c. ~ l:t£ 0.20.10 J~~ ~~~ 2 - - ~ Ci 3 ·t~~ ~ I 4 5 6 7 I 8 9 11 12 13 Patient Number Figure 2: Bar Chart comparing the Left to Right lateral displacements for the AP/PA image sets. The Radiographer- val. 49, no. 3, December 2002 143 VALIDATING THE USE OF DIGITALLY RECONSTRUCTED RADIOGRAPHS ~. AS VERIFICATION TOOLS IN RADIATION THERAPY SIMULATION OF PROSTATE TREATMENT ~ r = 0.89, p = <0.001 ~ ~ ~ ~ u; 0.6 E - .. ~ sCl)::: E Cl) (.) ..!!:! c.. .!a 0.4 ,'_,,,----'_,,,' "C a: a: 0 • /,_ ... 0.2 0 , 0.2 0 ') 0.6 0.4 0.8 Radiograph displacement (ems) Figure 3: Scattergram comparing lt-rt lateral isocentre displacement~ for the AP/PA image sets. The thin dotted line represents the y=x line between both image sets and the thick line represents the line of best fit for the measurements obtained. 10 8 I r = 0.99, p = <0.001 I u; E ~6 s::: Cl) E Cl) -a (.) tn :c 4 a: a: 0 2 0 2 3 4 5 6 7 8 9 Radiographs displacement (ems) Figure 4: Scattergram comparing isocentre displacements for the pooled data. The thin dotted line represents the y=x line between bo_th image sets and the thick line represents the line of best fit for the measurements obtained. \ displacements in sup/inf, lt/rt, and ant/post directions for both imaging modalities. Correlation analysis demonstrates a high level of statistically significant agreement between the DRRs and the simulator radiograph (r = 0.99, p = <0.001). Table 1 provides an overview of the level of agreement and 144 The Radiographer- vol. 49, no. 3, December 2002 the differences between individual and pooled image sets, as well as the correlation co-efficients for. the data sets. Perhaps the most important observation to be mad.e from the table is that for the pooled data there were 34 of 39 measured displacements between the image sets that were s0.3cm.· J.PARKER, M. VIGAR, S. DEMPSEY, H. WARREN-FORWARD, K. JOVANOVICH Table 1: Descriptive and statistical comparison of all individual image sets and the p9oled data. Left to Right Lateral Displacements from AP/PA image sets 100% isocentre agreement 5 out of 13 image sets Differences s0.3cm 12 out of 13 image sets Maximum difference 0.3cm Correlation Coefficient, p-value r = 0.89, p=<0.001 Superior/Inferior Displacements from AP/PA image sets 100% isocentre agreement 2 out of 13 image sets Differences s0.3cm 11 out of 13 image sets Maximum difference 0.4cm Correlati6n-coefficient, p-value r = 0.96, p=<0.001 Anterior/Posterior Displacements from lateral image sets 100% isocentre agreement 0 out of 13 image sets Differences s0.3cm 11 out of 13 image sets Maximum difference 0.8cm Correlation Coefficient, p-value r = 0.94, p = <0.001 Pooled Displacements from all images 100% isocentre agreement 7 out of 39 image sets Differences s0.3cm 34 out of 39 image sets Maximum difference 0.8cm Correlation Coefficien!, p-value r = 0.99, P=<0.001 DISCUSSION This study demonstrated, within the framework of how prostate planning and simulation is performed at the Mater Hospital, Newcastle, that DRRs \ire valid and accurate tools for verifying isocentre location with respect to pelvic bony anatomy, and therefore may replace simulation verification images with respect to establishing the treatment isocentre location in prostate treatments. With this result comes the idea that for those treatment regions where validation of the DRR to the simulator film has been demonstrated, the DRR can be used to establish the treatment isocentre position from the developed plan without the need for a post planning simulation session. This validation also means that the DRR could serve as the reference image for comparison with subsequent treatment verification images, but this suggested outcome would need to be validated in a study comparing treatment verification images to simulation reference images and the DRR reference image. Within this study it might have been possible to achieve a higher level of correlation if the quality of DRRs produced were improved. In this study the CT slice thickness used was 5mm, and this did not provide good bone edge definition, making it difficult to accurately measure isocentre displacements from bony landmarks. This problem could have been the reason why we obtained many differences that were between 0.1 and 0.3cm. By simply reducing the slice thickness to 3mm, the quality of the DRRs should improve allowing more accurate measurements to be obtained however there may be patient dose implications that need to be considered before doing this. This research uncovered a need for independent cross checking by another person, or the multiple measuring of data by the research group, to reduce measurement errors and increase measurement validity. It was found for one patient that the initial measurements taken from the isocentre for one DRR image were not de-magnified and therefore a large difference was noted between this and the simulation image. When this was discovered all measurements within the study were rechecked and the results changed for that patient increasing the resulting couelation analysis. Having introduced the discussion point of human error in measuring the DRRs and simulator radiographs, it should also be noted that the correlation might have been influenced by the error involved with the simulating therapist visually placing the fields in the simulation verification session. This is a source of potential error that needs to be ascertained. Care needs to be taken when generalising the results of this study to other departments or sites of treatment other than the prostate. There may be differences between clinical centres as to how patient~ are planned, simulated and treated. These differences may' be enough to require clinical sites to undertake their own replication studies to ensure internal validity of the outcomes. It wcpf mentioned in the introduction that there are ethical considerations to implementing new technology or new protocols. It;is not necessarily ethical to only think that a new technology may offer benefits and therefore should be rushed into clinical service. It is our responsibility to ensure through research that this is in fact the case, and that there is no possibility for the implementation of the technology or protocol to in fact do harm. This study validated the technology and protocol development of the use of DRRs priot to actual clinical use, and demonstrated equivalence with the current clinical methods used within the department. Benefits to the patient would include a reduction in the need for a simulation verification session leading to a reduction of patient time spent in preparation for treatment and decreasing patient radiation dose from simulation exposures. Possible harm could arise if the plan or DRR is developed incorrectly and . therefore treatment isocentre " localisation was inco~ct. This issue could be checked by visual inspection of the DRR against the marked CTs or by pretreatment verification images, ie port film or EPI. CONCLUSION This validation study has concluded on the basis of the highly statistically significant correlation analysis, that the DRRs produced as part of this prostate study do visually and quantitatively represent the isocentre position. The image sets demonstrated agreement of the isocentre position in x, y and z directions when compared to the current verification techniques employed at the clinical centre used within the study. The implication for the clinical centre may be a refinement of their current protocol to include the use of DRRs as both the initial source of isocentre position and also as the reference image for treatment verification. This notion has positive efficiency gains; for the department in terms of reducing simulation verification sessions; and for the patient in removing the need for an additional simulation session and resulting radiation dose. The results of this should now be further validated by a larger prospective randomised study which would take into account differences between patient physical characteristics, and monitored for the entire length of the patient's treatment using the DRR as the source of portal image verification. Also DRRs should be validated in each individual centre to allow for The Radiographer- val. 49, no. 3, December 2002 145 VALIDATING THE USE OF DIGITALLY RECONSTRUCTED RADIOGRAPHS ~ AS VERIFICATION TOOLS IN RADIATION THERAPY SIMULATION OF PROSTATE TFfEATMENT the differences with each centre to be included in the evaluation ofDRRs. Another conclusion drawn from the study is that a reduction in CT slice thickness would increase the quality of the DRRs produced and hence improve the quality of the images for use as a verification tool for prostate treatments which should make the measurement of differences more precise. The method we employed in this study is quite easy to perform and is reproducible for other treatment sites. The method could be replicated as part of a constant quality improvement procedure for other anatomical sites. Author's note Due to the outcomes of this study a larger randomised prospective study, as mentioned in the conclusion, is to be undertaken on prostate patients at the ~ater Hospital, NSW, Australia. With thanks to Mr Steve Howlett, Senior Medical Physicist, The Mater Hospital, NSW, Australia. The staff and patients of the Newcastle Mater Misercordae Hospital for their time and co-operation The work expressed in this paper owes much to the intellectual and supportive environment of The Discipline of Medical Radiation Science, Fac'~lty of Health, The University of Newcastle, Australia. REFERENCES 1. Bahner, M.L., Debus, J., Zabel, A., Levergrun, S., and Van Kaick, G. Digitally Reconstructed Radiographs From Abdominal CT Scans as a New Tool for Radiotherapy Planning, 1999, 34: 643-647. 2. Purdy, J.A. Ch 10, Three-Dimensional Physics and Treatment Planning, 1997, Principles and Practices of Radiation Oncology 3rd Ed. Perez, C.A., and Brady, L.W. Editors, Lippencott-Raven Publishers, Philadelphia. 3. Das, I.J., McGee, K.P., Desobry, G.E. The Digitally Reconstructed Image, 1995. A Practical Guide to CT Simulation. Cioa, L.R., Schultheiss, T.E. and Hanks, G.E. Editors, Advanced Medical Publishing Madison 1995. 4. Sherhouse, G.W., Novins, K. and Chaney, E.L. Cdinparison of Digitally Reconstructed Radiographs for use in Radiotherapy Treatment Design. International Journal of Radiation Oncology, Biology and Physics, ]990, 18: 651'. 658. \ I 146 The Radiographer- vol. 49, no. 3, December 2002 5. Ramsey, C.R. And Oliver, A.L. Magnetic Resonance Imaging Based Digitally Reconstructed Radiographs, Virtual Simulation, and Three-Dimensional Treatment Planning for Brain Neoplasms, Medical Physics, 1998', 25: 1923-1934. 6. Ramsey, C.R., Arwood, D., Scaperoth, D., and Oliver, A.L. Clinical Application of Digitally Reconstructed Radiographs Generated from Magnetic Resonance Imaging for Intracranial Lesions, International Journal Of Radiation Oncology, Biology and Physics, 1999, 45: 797802. 7. Galvin, J.M., Sims, C., Dominiak, G., and Cooper, J.S. The Use of Digitally Reconstructed Radiographs for ThreeDimensional Trea:tment Planning and CT-Simulation International Journal of Radiation Oncology, Biology and Physics, 1995, 31: 935-942. 8. Dawson, L.A., Mah, K., Franssen, E., and Morton, G. Target position Variability Throughout Prostate Radiotherapy, International Journal of Radiation Oncology, Biology and Physics, 1998, 42:1155-1161. 9. Valicenti, R.K., Waterman, F.M., Corn, B.W., and Curran Jr, W.J. A Prospective Randomized Study Addressing the Need for Physical Simulation Following Virtual Simulation, International Journal of Radiation Oncology, Biology and Physics, 1997. 39: 1131-1135. 10. Fritsch, D.S. Raghavan, S., Boxwala, A., Earnhart, J., Tracton, G., Cullip, T., and Chaney, E.L. Benchmark Test Cases for Evaluation of Computer-based Methods for Detection of Setup Errors: Realistic Digitally Reconstructed Electronic Portal Images with Known Setup Errors, International Journal of Radiation Oncology, Biology and Physics, 1997, 37: 199-204. Peer reviewed Submitted: June 2002 Accepted: October 2002