Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Nicotinic agonist wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Drug design wikipedia , lookup
Drug discovery wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Pharmacognosy wikipedia , lookup
Pharmacokinetics wikipedia , lookup
Prescription drug prices in the United States wikipedia , lookup
Prescription costs wikipedia , lookup
Urban legends about drugs wikipedia , lookup
Drug interaction wikipedia , lookup
Polysubstance dependence wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
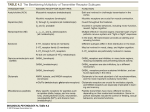
Modificazioni cerebrali associate all’utilizzo di droghe Silvia Mandillo ELLS LearningLAB “Conoscere il sistema nervoso” EMBL Monterotondo 22-24 Ottobre 2008 Parte I Definizioni Concetti generali Basi biologiche Parte II Nicotina Alcohol Cannabis Opioidi (Morfina, Eroina) Allucinogeni e club drugs (LSD, Ecstasy...) Psicostimolanti (Anfetamine, Cocaina...) What is drug addiction? Drug addiction is a chronic, relapsing BRAIN disease that is characterized by COMPULSIVE drug seeking and use, despite harmful consequences Use>Abuse>Addiction Why do people take drugs: -to feel good -to feel better -to do better Why do people CONTINUE to take drugs: -curiosity -not to feel sick -imitation -to feel ‘normal’ -love of risk -loss of control -habit Why do people become ADDICTED: -physical changes in the brain -loss of judgment -compulsive behavior Risk factors Does everybody become addicted to drugs? VULNERABILTY Biology/Genes Genetics Gender Mental disorder Age Environment Stress Repeated DRUG USE Early use Availability Cost Method of administration BRAIN changes Addiction Home and family School/Work Peer influence Increased risk with early use: The brain is still developing during adolescence ‘Physical vs. psychological dependence?’ Drug Drug Body Brain > Behaviour PET images of diseased organs Cerebral hemisphere lobes Brain regions, cortical areas and the limbic system Parietal lobe Sensory information Frontal lobe Decision-making Problem solving Planning Occipital lobe Vision Temporal lobe Memory Emotion Hearing Language Hippocampus Amygdala Motor coordination Limbic system Heart rate Breathing Sleeping Reward circuit Reward system Pfcx N.Acc Dopamine VTA Natural rewards Food Water Sex Nurturing Music Art …and Drugs! Neurons, synapses and neurotransmitters Drugs act at the synapse Dopamine Opioids Serotonin ACh GABA Glutamate Interfering with major neurotransmitter systems Drugs disrupt the reward circuit Methods of administration How much and for how long a drug acts in the brain depends on the dose and on the method of administration The way a drug is administered determines the amount and permanence in the brain and therefore its effect on behavior Effects on behavior Acute single use Hyperactivity, alertness, intense pleasure, relaxation Relieves of anxiety, stress and fatigue, perception changes Chronic repeated use Tolerance and dependence >>> ADDICTION Tolerance and dependence …are the main components of addiction. Tolerance decrease of a behavioral response after repeated administration of the same dose of a drug. The development of tolerance to the rewarding effect of a drug (e.g. morphine) leads to administration of the drug at increasing doses in order to experience the initial effect. Dependence is the altered physiological state induced by long-term drug exposure that leads to a withdrawal syndrome on cessation of drug administration. Neural mechanisms of addiction Long term administration of a drug elicits changes in the neurons of the central nervous system (CNS) that alter the functioning of neural circuits. 1. Receptor and transporters level: Increased or decreased number of binding sites 2. Structural level: Rearranging of synapses and connections Neuroplasticity Learning Brain changes in addiction Dopamine D2 receptors Serotonin neuron axons Brain regions and functions affected by drugs Parte II Most common drugs of abuse Nicotine Alcohol Cannabis Opioids (Morphine, Heroin) Hallucinogens and club drugs (LSD, Ecstasy...) Psychostimulants (Amphetamines, Cocaine...) Nicotine Nicotine is a natural alkaloid found in tobacco leaves. Nicotiana tabacum named after Jean Nicot (1530-1600) who introduced tobacco to Europe. Nicotine was first isolated in 1828. Reinforcing component of tobacco. When smoked, nicotine reaches the brain in about 10 seconds. It mimics the action of the neurotransmitter acetylcholine activating cholinergic nicotinic receptors. Nicotinic receptor are present in muscles, adrenal glands, heart and brain Actions in the brain Nicotine increases dopamine and endorphins levels in the reward pathways. Another component of tobacco decreases MAO levels (monoamine oxidase), enzyme for dopamine breakdown Nicotine’s effects Changes in respiration, blood pressure and vasoconstriction. Facilitation of task performance, improvement of memory, reward, reduction of anxiety, appetite suppression, analgesia Tolerance and dependence. Withdrawal syndrome is a major cause of relapse among people attempting to quit smoking, it produces: craving, irritability, anxiety, anger, difficulty concentrating, hunger, and fatigue Nicotine is highly addictive Smoking Tobacco use is the leading preventable cause of death in US Cancer, respiratory and cardiovascular diseases (stroke, heart attack..) Women are less successful to quit smoking Smoking helps to control body weight (appetite suppressant) Adolescents are more sensitive to reinforcing effects of nicotine More vulnerable to tobacco addiction High incidence of smoking in mental illness (e.g. schizophrenia) Alcohol Ethyl alcohol (Ethanol) derived in nature from fermentation of glucose and water Legal drug widely used as beverages for social and medical benefits Sedative, hypnotic, euphoric, ‘social lubricant’, anxiolytic Disinhibitory effects, stimulant At high doses it impairs: Motor coordination, reaction time, cognition, sensory processing, judgment Chronic use: Addiction (alcoholism), cirrhosis of the liver, heart disease, pancreatitis Action in the brain Frontal lobes, limbic system, cerebellum, reticular formation Initial action of ethanol at GABA and glutamate receptors It acts on the reward system increasing dopamine levels It also disrupt opioid peptides and serotonin systems It dysregulates brain stress system (CRF, NPY) It interacts into the cell with second-messenger and CREB systems Brain activity during memory task Cannabis Natural product of Cannabis sativa L. It is smoked as herbal (marijuana), resin (hashish) Psychoactive constituent is tetrahydrocannabinol (Δ9-THC) THC content and potency is variable It binds to cannabinoid receptors (anandamide, endogenous ligand) Analgesic and treatment of nausea from chemotherapy Fibre production (hemp) Cannabis Effects euphoria, relief of anxiety, sedation and drowsiness, changes in perception, mood swings Most commonly used illicit drug in US It is usually smoked, often mixed with tobacco or in a smoking device When smoked can be detected in plasma within seconds Plasma half-life: about 2 hours Metabolites can be detected in the urine for up to 2 weeks Typical dose of average ‘joint’ cigarette 200mg. Street names: pot, dope, weed, grass, hemp, Mary Jane… 2004 EU price: 5-10 eu per gram Opioids (Morphine, Heroin) Morphine a natural product of opium: the dried latex of certain poppy species (e.g. Papaver somniferum L.). Named after Morpheus the God of Dreams Heroin A semi-synthetic product of morphine. Diacetylmorphine is the psychoactive constituent of heroin Act as agonists at OPIOID receptors (the μ, κ and δ subtypes) that normally respond to endogenous peptides known as endorphins. Limbic system, brain stem, spinal cord. Narcotic analgesic Treatment of pain, diarrhea, cough Heroin Effects: Euphoria and a sense of detachment. Subjective effects following injection are known as ‘the rush’ and are associated with feelings of warmth and pleasure, followed by well-being and a longer period of sedation. Respiratory depression, nausea and vomiting, decreased motility in the gastrointestinal tract, suppression of the cough reflex and hypothermia. Withdrawal symptoms: Yawning, lacrimation, rhinorrea, perspiration, gooseflesh, tremors, dilated pupils, anorexia, nausea, vomiting, diarrhea, restlessness, insomnia, weight loss, dehydration, hyperglycemia, high blood pressure and pulse rate. Dysphoric state, depression, anxiety, craving Heroin Methods of administration ‘Smoked’ by heating the solid on a metal foil above a small flame and inhaling the vapour. Injected after solubilisation with citric acid. When injected it crosses BBB in 20 sec. 1-5 min when smoked. Plasma half-life: about 3 min Typical Dose 100mg. Street names: horse, smack, shit, brown Accidental overdoses Infectious diseases (hepatitis, HIV..) Heroin South-East Asia (China) more common in the ‘70s White powder, water soluble Injected 2004 price range: 31-202 eu per gram South-West Asia (Afghanistan, Pakistan) Brown powder, insoluble ‘Smoked’ 2004 price range: 12-141 eu per gram http://www.emcdda.europa.eu/ Hallucinogens and club drugs LSD, PCP, Ecstasy LSD: hallucinations (‘trips’), reality distortion, blend of five senses, perception alteration, fear, euphoria, psychosis, ‘flashbacks’ acid Phencyclidine (PCP): hallucinations angel dust Ecstasy (MDMA): euphoria, increased sensory awareness, socialization Adam, XTC 2004 price: 2-16 eu per tablet Serotonin system (5HT2 receptor, SERT) Glutamate receptor (NMDA receptor) Dopamine system (DAT) Neurotoxicity Ecstasy acute effects at serotonin synapse Normal state Serotonin overflow…. …and depletion http://www.dancesafe.org/slideshow/index.html Long term effects Reduced DAT binding Neurotoxicity Psychostimulants Amphetamine: Synthetic, ingested, Methamphetamine: Synthetic, ingested, smoked. More potent Cocaine: Natural, snorted or smoked Psychomotor stimulant, euphoria, tachycardia, hypertension and appetite suppression, increased confidence, sociability and energy Cocaine and methamphetamine are strong reinforcers and highly addictive (tolerance and dependence) Following oral use, the effects of usually start within 30 minutes and last for many hours. Later, users may feel irritable, restless, anxious, depressed and lethargic. Upon chronic use: deficits in memory and in decision-making and verbal reasoning. Some of the symptoms resemble those of paranoid schizophrenia. Cocaine Cocaine is a natural product extracted from the leaves of Erythroxylon coca Lam (South America) Snorted. Free base form is smoked (Crack) Typical dose: 100-200mg Street names: coke, snow, charlie, C 2004 price: 41-100 eu per gram Medical use as local anesthetic Psychostimulants increase dopamine levels by blocking the dopamine transporter or facilitating dopamine release in the reward pathway (VTA-N.Acc) VTA N.Acc Long term effects • Irritability and mood disturbances, restlessness, paranoia, auditory hallucinations • In animals minimal exposure to cocaine can alter the dopamine responsiveness for at least a week •After chronic cocaine abuse, dopamine activate the reward system even if the abuser encounters a cue associated with the drug • Craving and relapse Lifetime prevalence % of Population having tried COCAINE at least once Treatment of addiction Medications nicotine, bupropion, methadone, naltrexone, acamprosate, disulfiram Behavioral intervention enhance the saliency value of natural reinforcers (social support) strengthen inhibitory control and executive functions decrease conditioned responses improve mood if disrupted Prevention act on the environmental factors (reduce stress, limit exposure) more information prohibition Effects of Methamphetamine D2 receptors DAT binding Websites on drug addiction United States http://www.drugabuse.gov/ Website of the National Institute on Drug Abuse (NIDA) part of the NIH - National Institutes of Health The most complete. A lot of downloadable educational material. For example: http://www.nida.nih.gov/MOM/MOMIndex.html http://www.nida.nih.gov/pubs/Teaching/ Europe http://www.emcdda.europa.eu/ Site of the European Monitoring Centre for Drugs and Drug Addiction (EMCDDA). In multiple languages. EMCDDA was founded in 1993, it is based in Lisbon and it is the hub of drug-related information in the European Union. Very good drug profiles http://www.emcdda.europa.eu/index.cfm?nnodeid=25328 Grazie! [email protected]