Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
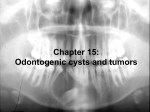
Nidhi Gupta et al International Journal of Clinical Pediatric Dentistry, January-April 2009;2(1):56-58 CASE REPORT What Lies Within? 1 Nidhi Gupta, 2Manohar Bhat, 3Rajesh Sharma 1 PG Student, Department of Pedodontics and Preventive Dentistry, Jaipur Dental College, Jaipur, Rajasthan, India 2 Professor and Head, Department of Pedodontics and Preventive Dentistry, Jaipur Dental College, Jaipur, Rajasthan, India 3 Reader, Department of Pedodontics and Preventive Dentistry, Jaipur Dental College, Jaipur, Rajasthan, India Correspondence: Nidhi Gupta Postgraduate Student, Department of Pedodontics and Preventive Dentistry, Jaipur Dental College, Jaipur, Rajasthan, India Ph: 09352782342, 09810358916, e-mail: [email protected] Abstract What follows is a case report of a 12 years old child who complained of gaps between teeth in the lower front region. OPG showed tooth 43 impacted and malformed with enlarged pulp chamber and a unilocular radiolucency surrounding the crown. Surgical enucleation was done under LA. Biopsy was sent for histopathological examination revealing the miracle diagnosis of “Central Odontogenic Fibroma” being a rare tumor of odontogenic tumor family and also a rare finding regard to age, site and clinical behavior of tumor is reported. Keywords: Odontogenic fibroma, odontogenic tumor. INTRODUCTION CASE REPORT A 12 years old male child presented to Jaipur Dental College, Department of Pedodontics and Preventive Dentistry. The chief complaint of patient was gaps between teeth in lower front region. Patient gave history of crown fracture of 42 which he had got endodontically treated. The patient used Neem datun to maintain his oral hygiene and behaviorally the patient was cooperative. Extraoral examination revealed that patient was of normal built with facial symmetry bilaterally symmetrical, oval facial form and a straight facial profile. On Intraoral examination soft tissue appeared normal. On hard tissue examination all permanent teeth were present except 41, 43 and 45 (Fig. 1). Central odontogenic fibroma is a rare and benign neoplasm of jaw. It is derived from mesenchymal component of odontogenic apparatus that is dental papillae, dental follicle and periodontal ligament. Clinically it is more frequently seen in children and young adult. Commonly found in mandible but in posterior regions. Radiographically, majority of COF are radiolucent with multilocular radiolucency and rarely unilocular. Lesion often contains small radiopaque flecks of varying density. Histologically WHO type COF consists of mature cellular fibrous connective tissue with many islands of odontogenic epithelium. Osteoids, dysplastic dentin and cementum can be seen. Case of central odontogenic fibroma 1 and central odontogenic fibroma—granular cell variant type2 have been reported in the literature. Fig. 1: Intraoral lower arch 56 What Lies Within? Fig. 2: Preoperative OPG 42 showed unsatisfactory restoration and was drifting distally. Molar relation on left side was class I and on right side class III. The patient was advised for OPG to see the missing teeth (Fig. 2). Radiographic examination revealed: 41: congenitally missing 42: endodontically treated 45: impacted, and an unusual finding was seen in relation to 43 which was impacted and malformed with enlarged pulp chamber and radiolucency completely surrounding the crown. At this juncture, the patient was referred to orthodontic department for further opinion regarding definitive orthodontic treatment plan and it was decided to first undergo surgical extraction of malformed 43 followed by fixed orthodontic therapy. Therefore, the treatment plan was, first the oral prophylaxis was done, then surgical extraction of malformed 43 followed by restoration of 42 followed by fixed orthodontic therapy. SURGICAL PROCEDURE The surgery was planned and consent of parents was taken. The inferior alveolar nerve block was given on right side. The incision extending from mesial of 42 to 44 was made and the envelop flap was raised and the lesion was exposed. Then, we surgically extracted 43 along with the soft tissue lesion (Fig. 3). The flap was repositioned and interrupted sutures were given. Then, the specimen (Fig. 4) was sent to oral pathology department for histopathological examination. 57 Fig. 3: Extracted socket Fig. 4: Extracted 43 MICROSCOPICALLY Soft tissue section consisted of soft connective tissue stroma with collagen fibers arranged in whorl pattern. The fibrous component varied from fibrous to myxoid. Island of odontogenic epithelium (Fig. 5) were visible all over the connective tissue stroma. Some islands appeared ameloblast like cells and stellate reticulum and some solid lacking features of odontogenic epithelium. Few islands were surrounded by eosinophilic material (Fig. 6). Numerous calcification in form of dentids and cementum visible. Fibrous capsule with strands and islands of odontogenic epithelium was seen. Dentin hypocalcified at places and showed interglobular dentin. Regular enamel space was Nidhi Gupta et al Fig. 7: Postoperative OPG Fig. 5: Histopathological slide 1 Fig. 6: Histopathological slide 2 seen. Cementum appeared normal. Pulp showed collagen fiber, blood vessels and pulp stones. Pulp stones did not resemble dentin. Seeing the histological findings the diagnosis came as “Central odontogenic fibroma—WHO type”. It is asymptomatic and displacement of teeth can be seen. It is more commonly seen in children and young adults and is more prediculent in females.5 But in this case it was seen in a young boy. Radiographically, majority of COF are radiolucent with multilocular radiolucency and rarely unilocular.3 In this case unilocular radiolucency was seen. Lesion often contain small radiopaque flecks of varying density. Postoperative OPG is shown in Figure 7. Histologically, the WHO type consist of mature cellular fibrous connective tissue with many islands of odontogenic epithelium. Osteoids, dysplastic dentin and cementum can be seen.6 The histopathological finding of this case were very much similar to central odontogenic fibroma (WHO type) therefore, this diagnosis was given. REFERENCES 1. Covani U, Crespi R, Perrini N, Barone A. Central Odontogenic Fibroma—A case report; Med oral Patol Oral cir buccal 2005; 10(suppl 5):154-7. 2. Calvo N, Alonso D, Prieto M, Junquera L. Central Odontogenic Fibroma—Granular cell varient. Journal of Oral Maxillofacial Surgery 2002;6:1192-4. 3. Shaffer’s Textbook of Oral Pathology. Odontogenic cyst and Tumour; 4th edition. 4. Daniels JS. Central odontogenic fibroma of mandible: A case report and review of literature. Journal of Oral Surg Oral Med Oral Pathol Oral Radio Endod 2004;98(3);295-300. 5. Manekar VS, Dolas RS. Central odontogenic fibroma—A review of literature and report of three cases. Journal of DMERMilestone 2004;3(No.1):31-6. 6. Allen CM, Hammond HL, Stomson PG. Central odontogenic fibroma – WHO type: A case report. Oral surgery, Oral Medicine, Oral Pathology 1992;73:62-6. DISCUSSION Central odontogenic fibroma is a rare and a benign neoplasm of jaw. It is derived from mesenchymal component of odontogenic apparatus that is dental papillae, dental follicle and periodontal ligament.3 Clinically, it is found in maxilla and mandible. More frequently seen in mandible in the posterior region but, in this case it was seen in anterior region of mandible.4 58 INTERNATIONAL JOURNAL OF CLINICAL PEDIATRIC DENTISTRY Submitting a paper to INSTRUCTIONS TO AUTHORS INTERNATIONAL JOURNAL OF CLINICAL PEDIATRIC DENTISTRY is an international journal, the aim of which is to promote education and research in pediatric dentistry. The journal publishes papers on all the aspects of pediatric dentistry. Manuscripts prepared according to “Uniform Requirements of Biomedical Journal” are invited for editorial review and publication. Published papers are the views of the respective authors and do not necessarily represent the views of the editorial board or publishing house. Manuscript submission: Manuscript are received with the understanding that they contain original data that is not previously published or is being considered for publication elsewhere. Only individuals who have made significant contributions to the manuscript should be listed as authors, all other contributions should be noted in acknowledgments. Authors are required to submit two printed copies of the manuscript including all tables and figures (photographs) along with a CD, which should contain both blinded and unblinded article file and introduction file in Microsoft word format and photographs in jpeg, tiff, gif, bmp, eps format. The first or corresponding author should send the following duly signed by all contributing authors along with the manuscript: contribution form, copyright transfer form, corresponding author form and submission form. Send the manuscripts to Editor-in-Chief: Dr Usha Mohan Das Dean, VS Dental College, Bangalore e-mail: [email protected] Online submission: You can also submit your manuscripts online by e-mail to: [email protected], [email protected] or upload your manuscript at www.jaypeebrothers.com (Please note only one mode of submission must be used, i.e. postal or online. For online submission send 1 hard copy of the photographs along with contribution form, copyright transfer form, corresponding author form and submission form to the above address. Type of articles: The journal publishes original articles not exceeding 2500 words and case reports not exceeding 1000 words (excluding introduction file, abstract, legends and references) with not more than 15 references. Preparation of manuscript: Manuscript should be prepared in text file and separate file for illustrations. Times new roman or Arial font with a font size of 12 and double spaced text with one inch margins should be the basis of text files. Introduction file should contain a covering letter, acknowledgment and title page (type of manuscript, title of manuscript, complete address, degree and academic details of all authors including phone numbers and e-mail. The details of corresponding author must be mentioned separately). Abstract: All manuscripts must have an abstract, which provides the reader with a brief but complete summary of the paper. The aim, material and method, results and conclusion must be clearly demarcated. The abstract should not be more than 250 words for an original article and 150 words for a case report. A list of key words must be included at the end of abstract. Introduction: It should provide a concise summary of the research and state the hypothesis to be tested. Material & methods: All relevant attributes of the material forming the subject of the research should be provided. Experimental methodology should be concisely and appropriately explained. Commercially produced materials, devices, software, etc. must be followed by name of manufacturer and location. If an abbreviation has to be used then it should be placed in parentheses following the full spelling of the term for the first time. Statistical methods should be clearly specified. Manuscripts reporting human studies should include evidence that study was ethically conducted in accordance with declaration of Helsinki. Results should be presented sequentially in tables and illustrations. The data in the tables and illustration should not be repeated in text but should indicate the most important result and describe relevant pattern. All units of measure should be in accordance with International system of units. Laboratory data values should be rounded to the number of digits that reflects precision. The statistical comparisons should include statistical test value and p-value. If P > .01, the actual p-value must be expressed in two digits. If P<.01 it should be expressed in three digits and non-significant values should be mentioned as NS. Discussion: This section describes the findings of the study, limitations of materials, interpreting the data and drawing contribution of the study in scientific field. No repetitions of the previous sections should be done. All the controversies, implications and future prospects related to the study should be mentioned. Discussion should end with a brief summary of conclusion. Legends should have detailed explanation of the illustrations. Tables: Each table should be double-spaced typed on separate page and should be numbered in Arabic numericals. Short headings should appear at the top of each column. All non-standard abbreviations should be explained. Figures / Illustrations: Colored photos with minimum 300 dpi resolution of 4 X 6 inch should be sent. Labels citing the legend, figure no., author and title of the manuscript should be pasted on back of photograph. Acknowledgements: Funding and other sources of support must be disclosed in this section. Personal acknowledgment should be limited to professionals who have contributed to the paper but whose contribution does not justify authorship. References should be relevant to the material presented and identified by superscript in Arabic numerals. List of references should appear at the end of paper as they appear in numeric order as they are cited in text and the abbreviations used should be those used by Index Medicus. Authors should verify accuracy of all references and provide direct references whenever possible. Avoid using abstracts or in press papers for references. Journal: Name of author, Title, Journal name, Year of publication, Issue, Page no. Books: Name of author, Chapter name, Book authors, Book name, Edition, Publishers, Year of publication, Page no. Web: “Website name”. Date Copyright: IJCPD holds the copyright of all the editorial content published in this journal. All accepted manuscripts and their accompanying illustrations become a permanent property of IJCPD and may not be published anywhere in part or full, in print or electronically without written permission from IJCPD. Reprint: No free reprints will be provided to the author or others. The journal can be subscribed at a discount of 25 percent by the author of the article. Disclosures: Authors should include all relevant information regarding conflicts of interest and sponsorship statement.