Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Remote ischemic conditioning wikipedia , lookup
Cardiovascular disease wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Saturated fat and cardiovascular disease wikipedia , lookup
Electrocardiography wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
History of invasive and interventional cardiology wikipedia , lookup
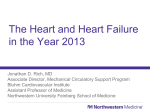
Case Report Acta Cardiol Sin 2004;20:191-6 Successful Percutaneous Coronary Intervention in a Patient with Dextrocardia and Situs Inversus Hung-Shun Lo, Meng-Ling Chen, Po-Chin Chou and Herng-Cheng Chiou Dextrocardia is a rare congenital anomaly of development characterized by a mirror- image position of the heart and abdominal viscera. Unlike dextrocardia with situs solitus or ambiguus, the coincidence of congenital heart disease is relative low among dextrocardic patients with situs inversus. However, patients with dextrocardia may suffer from coronary heart disease as do people with normally positioned hearts. Few cases of coronary angiography and percutaneous coronary intervention in patients with dextrocardia have been reported. We describe a 70-year-old female patient with dextrocardia who developed unstable angina and was able to undergo diagnostic catheterization and percutaneous coronary intervention. We successfully performed percutaneous coronary angioplasty followed by coronary stenting to the right coronary artery (RCA) and left anterior descending coronary artery (LAD) and described our experience in the selection of the guiding catheters (standard preformed catheters), angiographic image views acquisition (mirror-image views with subtle modification) and coronary catheter engaging techniques (opposite-direction catheter rotations). Key Words: Dextrocardia · Situs inversus · Percutaneous coronary intervention · Coronary stenting INTRODUCTION coronary angiography and percutaneous coronary intervention (PCI) in patients with dextrocardia have been reported.3 To the best of our knowledge, this is the first report of successful coronary angiography and ad hoc coronary stenting in a patient with dextrocardia with situs inversus in Taiwan. We herein describe a case of percutaneous transluminal coronary angioplasty (PTCA) followed by coronary stenting to the right coronary artery (RCA) and the left anterior descending artery (LAD) and our experience in the selection of the guiding catheters, angiographic image views acquisition and coronary catheter engaging techniques. Situs inversus with dextrocardia is a rare congenital anomaly of development characterized by a mirror-image position of the heart and abdominal viscera. 1,2 It occurs rarely in the general population, with an estimated incidence of 1:8,000 to 1:10,000.1 Patients with dextrocardia usually have structurally normal hearts and experience normal longevity2 but may suffer from acquired heart disease such as coronary heart diseases as do people with normal positioned hearts.3-5 Few cases of Received: January 6, 2004 Accepted: February 18, 2004 Division of Cardiology, Department of Internal Medicine, Cathay General Hospital, Taipei, Taiwan. Address correspondence and reprint requests to: Dr. Hung-Shun Lo, Division of Cardiology, Department of Internal Medicine, Cathay General Hospital, No. 280, Sec. 4, Ren-Ai Road, Taipei, 106, Taiwan. Tel: 886-2-2708-2121 Ext. 3111; Fax: 886-2-2707-4949; E-mail: [email protected] CASE REPORT A 70-year-old woman presented to our institution with the chief complaint of intermittent retrosternal and right anterior chest tightness for 1 month, aggravated in 191 Acta Cardiol Sin 2004;20:191-6 Hung-Shun Lo et al. eter was passed through the right-sided aortic knob into the left ventricle. The 30° left anterior oblique (LAO) ventriculogram showed no regional wall motion abnormalities, with an ejection fraction of 70%. The ostium of the left main coronary artery was cannulated with simple catheter advancement using a 6 Fr Judkins left 4-cm (JL 4) diagnostic catheter in a right anterior oblique (RAO) 60° view. The selective left coronary angiogram (38° RAO, 18° cranial view and 0° postero-anterior view, 39° cranial view) revealed a 70% tubular stenosis in the proximal left anterior descending (LAD) artery, a 90% stenosis at the ostium of first diagonal branch (DB) and a patent left circumflex (LCX) artery (Figures 2a, 2b). The ostium of the right coronary artery (RCA) was also easily engaged by gentle counterclockwise rotation and slightly withdrawal of a 6 Fr Judkins right 4 cm (JR 4) diagnostic catheter in RAO 60° view. The right coronary angiogram (RAO 60° view) showed an 80% stenosis at the middle RCA (Figure 3a). PCI was subsequently per- recent days. Her risk factor of coronary artery disease was hypertension for more than 10 years. Her family history was noncontributory. Physical examinations were unremarkable except for findings consistent with dextrocardia. Normal heart sound and apical impulse were noted in the right chest. Her electrocardiogram (ECG) showed findings consistent with dextrocardia. The ECG taken with reversed arm and precordial leads showed left ventricular hypertrophy with ST-T abnormalities and T- wave abnormalities at II, III, aVF and V4 to V6 leads indicating possible ischemia (Figures 1a, 1b). Chest X-rays revealed dextrocardia with a right-sided aortic knob as well as gastric bubble. Echocardiography disclosed mitral annulus calcification, no regional wall motion abnormalities and normal left ventricular function without other concomitant congenital abnormalities. Cardiac catheterization was performed via the right femoral artery using mirror-image views and standard Judkins catheters. A 6 French (Fr) angulated pigtail cath- Figure 1. (a) Standard ECG demonstrates findings consistent with dextrocardia. (b) The ECG taken with reversed arm and precordial leads shows left ventricular hypertrophy with ST-T abnormalities and T-wave abnormalities in II, III, aVF and V4 to V6 leads indicating possible ischemia. Acta Cardiol Sin 2004;20:191-6 192 Percutaneous Coronary Intervention in Dextrocardia formed to the RCA. In RAO view, a 6 Fr Cordis JR 4 guide catheter (Cordis Corporation, Miami, FL) was engaged into the right coronary ostium, as described in the diagnostic procedure. The mid-RCA lesion was crossed with a 0.014² ACS floppy wire (Advanced Cardiovascular Systems, Inc., Temecula, CA) and a 3.25 ´ 20-mm Figure 2. Pre-stenting angiogram (a) (38° RAO; 18° cranial), (b) (0° PA; 39° cranial) show a 70% stenosis in the left anterior descending (LAD) artery, a 90% stenosis at the proximal diagonal branch (DB) and a patent left circumflex (LCX) artery. Post-stenting angiogram (c) (38° RAO; 18° cranial), (d) (0° PA; 39° cranial) show an excellent result. The arrows mark lesion sites. Figure 3. (a) Pre-stenting angiogram with 60° RAO view shows an 80% stenosis in the middle RCA; (b) Post-stenting angiogram shows an excellent result. 193 Acta Cardiol Sin 2004;20:191-6 Hung-Shun Lo et al. semi-compliant Adante balloon catheter (Boston Scientific/Scimed, Inc., Maple Grove, MN) and was dilated at 8 atm. A 3.5 ´ 18-mm NIR Elite stent (Boston Scientific/Scimed, Inc., Maple Grove, MN) was deployed by usual standard method. The post-stenting angiography revealed no residual stenosis and no dissection (Figure 3b). Then a 6 Fr Cordis JL 4 guide catheter was engaged into the left coronary ostium using a RAO 60° view. Using a 0.014 ² ACS floppy wire and a 2.75 ´ 20-mm Adante balloon catheter, the proximal LAD was crossed and dilated at 8 atm. A 3.0 ´ 25-mm NIR Elite stent was deployed. Final angiography revealed no residual stenosis and no dissection. (Figures 2c, 2d). The patient experienced an uneventful recovery and was discharged 3 days later. She was free of angina on clinical follow-up for more than 30 months. coronary heart disease, on whom catheterizations were performed without difficulty by using Judkins technique in 5 cases, and Sones technique in four, and with only 1 case requiring additional catheters. Coronary artery bypass surgery in a patient with dextrocardia was described in 1982, 8 and coronary grafting with a right internal mammary artery was reported in 1988.9 As for PCI techniques, 2 patients undergoing coronary angioplasty were reported by Moreyra in 198710 and Gaglani in 1989.11 Lewis reported directional coronary atherectomy in 1993,12 Waster reported coronary angioplasty in a single coronary artery in 1994 13 and Kay reported rotational atherectomy in 200214 for patients with dextrocardia and situs inversus. Moreyra10 concluded that regular coronary catheters (Judkins) are difficult to use because of the reversed position of the coronary ostia. He recommended multipurpose catheters used with of the Sones technique. However, his difficulty was not encountered in our experience and other previous reports.3,10-12 Since the portions of the coronary ostia relative to the sinuses and to the aortic arch are a mirror image of the normal orientation, the mirror-image angiographic views are thus useful for catheter manipulations and image acquisition. In mirror-image positions, catheters can be passed using the standard technique, except that the catheters are rotated in the opposite direction for patients with dextrocardia when compared to patients with normal cardiac anatomy (e.g. counterclockwise rotation is used to cannulate the ostium of the RCA in patients with dextrocardia rather than the standard clockwise catheter rotation).3,10-12 It should be noted that for both the right and the left coronary arteries in biplane angiography, the LAO and RAO angulations are essentially reversed from the normal biplane angulations. Of course, appropriate mirror-image view with somewhat modified angulations to achieve the better visualization of coronary arteries is mandatory. In our experience, we utilized the mirror-image views with subtle modification of angle and opposite-direction catheter rotation. The 30° LAO ventriculogram was used to determine the wall motion abnormalities and global left ventricular function. The selective left coronary angiograms were obtained in the RAO cranial, postero-anterior (PA) cranial and LAO caudal views with some appropriate angulations, respectively. The selective right coronary angiograms were DISCUSSION Situs inversus with dextrocardia is a rare congenital anomaly of development characterized by a mirror-image position of the heart and abdominal viscera. 1,2 Dextrocardia with situs inversus occurs rarely, with an estimated incidence of 1:8,000 to 1:10,000. 1 Unlike dextrocardia with situs solitus or situs ambiguous, the incidence of congenital heart disease is relatively low among dextrocardic patients with situs inversus and is estimated to be about 3 percent.2 Although dextrocardia with situs inversus is a rare disease, the patient with dextrocardia may suffer from coronary heart disease as do people with normally positioned hearts.3-5 However, the presence of coronary heart disease in patients with dextrocardia and situs inversus has been reported infrequently. The patient with dextrocardia lives commonly unnoticed until symptoms related to acquired diseases (e.g. coronary heart disease) force the patient to seek medical attention, which readily uncovers the abnormality. Interestingly, in this patient, the pain was located in the retrosternal and right anterior chest. This atypical pain in patients with situs inversus has been only described by Hynes et al. in 1973.6 Coronary angiography for dextrocardia was first reported in 1974 7 in a patient who underwent left ventricular aneurysmectomy. In 1991, Blankenship 3 summarized a total of 10 cases with dextrocardia and Acta Cardiol Sin 2004;20:191-6 194 Percutaneous Coronary Intervention in Dextrocardia with dextrocardia. Cathet Cardiovasc Diagn 1991;23:103-6. 4. Hymes KM, Gau GT, Titus JL. Coronary heart disease in situs inversus totalis. Am J Cardiol 1973;31:666-9. 5. Pfashkin D, Stein E, Warbasse JR. Congenital dextrocardia, with anterior wall myocardial infarction. Am Heart J 1967;74:262-7. 6. Hynes KM, Gau GT, Titus JL. Coronary heart disease in situs inversus totalis. Am J Cardiol 1973;31:666-9. 7. Richardson RL, Yousufuddin M, Eubanks DR. Ventricular aneurysm, arrhythmia, and open heart operation in a patient with dextrocardia. Am Surg 1974;40:666-70. 8. Irvin RG, Ballenger JF. Coronary artery bypass surgery in a patient with situs inversus. Chest 1982;81:380-1. 9. Abensur H, Ramires JA, Dallan LA, Jatene A. Right mammarycoronary artery anastomosis in a patient with situs inversus. Chest 1988;94:886-7. 10. Moreyra AE, Saviano GJ, Kostis JB. Percutaneous transluminal coronary angioplasty in situs inversus. Cathet Cardiovasc Diagn 1987;13:114-6. 11. Gaglani R, Gabos DK, Sangagni BH. Coronary angioplasty in a patient with dextrocardia. Cathet Cardiovasc Diagn 1989;17: 45-7. 12. Lewis BE, Leya FS, Jones P, et al. Successful directional coronary atherectomy in a patient with dextrocardia and situs inversus. Cathet Cardiovasc Diagn 1993;29:47-51. 13. Wester JPJ, Ernst JMPG, Mast EG, et al. Coronary angioplasty in a patient with situs inversus totalis and a single coronary artery. Cathet Cardiovasc Diagn 1994;31:304-8. 14. Kay J, Kwok OH, Chow WH. Successful rotational atherectomy and stenting in a situs inversus patient. J Invas Cardiol 2002; 14:682-5. obtained in the RAO 60°, PA cranial and LAO 30° views. As for the PCI techniques, they were similar to the diagnostic procedures. We report that the standard angiographic techniques described above using opposite-direction catheter rotations and mirror-image views are useful for both angiography and angioplasty procedures in dextrocardic patients. Furthermore, varieties of PCI (balloon angioplasty, stenting, etc.) are likewise applicable to patients with dextrocardia. ACKNOWLEDGEMENTS The authors would like to thank Mr. Dwan-Chen Chang for technical support and Ms. Su-Tse Hwang for nursing assistance. REFERENCES 1. Rosenberg HN, Rosenberg IN. Simultaneous association of situs inversus, coronary heart disease and hiatus hernia. Ann Intern Med 1949;30:851-9. 2. Perloff JK. The Clinical Recognition of Congenital Heart Disease, 3rd ed. Philadelphia: WB Saunders Co., 1978;19-42. 3. Blankenship JC, Ramiers JA. Coronary arteriography in patients 195 Acta Cardiol Sin 2004;20:191-6 Case Report Acta Cardiol Sin 2004;20:191−6 以經皮穿刺冠狀動脈介入性療法成功治療右位心及 內臟逆位之病患 羅鴻舜 陳孟麟 周柏青 邱恆正 台北市 國泰綜合醫院 心臟內科 右位心乃是一種罕見的先天性發育異常,其特徵為心臟及內臟器官發生鏡像逆位。內臟逆 位的右位心與內臟正位或內臟錯位的右位心病患不同的是,其罹患先天性心臟病的機率相 當的低。然而,右位心且內臟逆位的人,罹患冠狀動脈心臟病的機率與正常人相同。有關 右位心病患接受冠狀動脈血管攝影及經皮穿刺冠狀動脈介入性療法之病例報告並不多見。 在此陳述一位七十歲具有右位心的女性,罹患不穩定型狹心症,接受心導管檢查及經皮穿 刺冠狀動脈介入性治療。我們在有病變的右冠狀動脈及左前降枝成功地實施經皮穿刺冠狀 動脈擴張術暨血管內支架植入術。同時描述一些技術上的問題:導管的選擇為一般常用的 標準成型導管,血管攝影影像之擷取選擇鏡像影像加以略作修飾,以及導管運作採取逆向 等。 關鍵詞:右位心、內臟逆位、經皮穿刺冠狀動脈介入性療法、血管內支架植入術。 196