Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Coronary artery disease wikipedia , lookup
Heart failure wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Rheumatic fever wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Myocardial infarction wikipedia , lookup
Cardiac surgery wikipedia , lookup
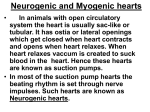
Proceedings of The 20th World Multi-Conference on Systemics, Cybernetics and Informatics (WMSCI 2016) PACEMAKER: An Insight Into the Artificial Heart Rhythm Lubna Moin Department of Engineering, Faculty of Electronics and Power Engineering, PNEC, National University of Sciences and Technology, Islamabad, Pakistan Vali Uddin Department of Engineering, Faculty of Engineering Science and Technology Hamdard University, Karachi, Pakistan Bhawany Shankar Chowdhry Department of Engineering, Faculty of Engineering Science and Technology, Mehran University, Jamshooro, Pakistan and Attaullah Y. Memon Department of Engineering, Faculty of Electronics and Power Engineering, PNEC, National University of Sciences and Technology, Islamabad, Pakistan 70-80 times per minute building up the heart beat. Figure 1 illustrates the conduction system of the heart. ABSTRACT A pacemaker is a small battery powered device, which paces the heart by sending an electrical impulse, to cause rhythmical contraction of the heart muscle. Since the first artificial pacemaker was introduced in 1932, much has changed and will continue to change in future. The complexity and reliability of modern pacemakers has increased significantly, mainly due to development in the integrated circuit design. This paper basically will discuss the electronic perspective of the pacemakers, the advancements done in this regard and the ongoing research to make it more competent, capable and useful. Keywords: Cardiac pacemaker, integrated electrocardiograph, biological pacemakers. circuits, Figure 1: Heart Conduction System [1] The figure 2 drawn below illustrates a single heart beat. As shown below the atrial depolarization gives rise to P wave. The PR interval is due to the delay at AV node. It is measured from the beginning of the P wave to the beginning of the QRS complex. The QRS represent the rapid depolarization of the right and the left ventricle. The ST segment delineates the depolarization of the ventricles. 1. INTRODUCTION The heart is bestowed with certain specialized cells meant for two main purposes. First purpose is to provoke the rhythmical electrical impulses that can cause co-ordinated contraction of heart muscles. Second objective is the proper guidance of the conduction of these impulses rapidly through the whole heart. Under normal conditions the atria contracts about 1/6 th of a second before the ventricular contraction, allowing the filling of the ventricle for further pumping. An added importance of this system is that it allows both the ventricles to contract proximately at the same time which is necessary for compelling pressure of the ventricles. These specialized cells are present in Sinoatrial SA node present in the right atrium. The signal generated in the cells of the SA node is conducted toward left atrium through Bachman Bundle. The signals from SA node travels downwards through Atrioventricular AV node. The AV node transfers the signal to the ventricles in the form of HIS Bundles and Purkinje Fibers. So the SA node, Bachman Bundles, HIS Bundles and Purkinje Fibers together form the conduction system of the heart. The signal generated in the cells of the SA node is conducted toward left atrium and to AV node. SA node is made up of a group of cells called myocytes. These cells contract due to depolarization and repolarization at rate of Figure 2: Typical Electrocardiogram [1] Lastly the ventricular contraction is depicted by R wave. The repolarization of ventricle is portrayed by T wave. All these waves have different voltage peaks and duration as shown in table 1 below 116 Proceedings of The 20th World Multi-Conference on Systemics, Cybernetics and Informatics (WMSCI 2016) Peak Table 1: ECG Voltage Levels Av. Voltage Duration P 0.25mv R-P 488ms R 1.6mv R-R 833ms T 0.1mv-0.5mv R-T 145ms It was noticed by a Canadian electrical engineer John Hopps while investigating the upshots of radio frequency in 1941 that if the heart abdicate generating pulses due to fall in temperature, it can be proceeded to beat artificially using mechanical and electrical stimulations. This research confesses the evolution of the first cardiac defibrillation machine in 1949. Hayman was the scientist who designed the first experimental pacemaker in 1932. Hyman‟s pacemaker was powered by a hand-wound spring driven generator that provided 6 minutes of pace making without rewinding. The block diagram of his pacemaker is given in figure 5, shown below. 2. ARTIFICIAL PACEMAKER Speed control The pacemaker, or sinoatrial node, is responsible for controlling heart rate. The cells of SA node are self firing cells. The depolarization and repolarization action is analogous to the relaxation oscillator if compared to electronic devices which is used to produce a periodic flash from the source of light. When the natural pacemaker does not function properly, the heart can suffer from arrhythmias such as bradycardia (heart pumps too slow), tachycardia (heart pumps too fast), or irregular heartbeats. The most common way of taking care of these conditions is by use of an artificial pacemaker that is implanted with the heart, shown in figure 3. Artificial pacemakers are the electronic devices that stimulate the heart by generating electrical impulses to restore or maintain the normal rhythm. The implanted pacemaker can send out an electrical impulse similar to the one a natural pacemaker. It can control the impulses sent out per minute with a computer chip and circuitry [2]. Hand Crank Winds up Spring motor Magneto-generator Drives Impulse control Current Drives ; Interrupter Disc Stimulus Pulsed current Heart (Right Atrium) Needle Electrode Figure 5: Block diagram of Hyman‟s pacemaker [4] The first implantable pacemaker was invented by Dr. Rune Elmqvist in the year 1958. Later in 1959 engineer Wilson Greatbatch and the cardiologist W.M Chardack developed first fully implantable pacemaker. Engineer Wilson Greatbatch while modeling an oscillator to record heart sounds negligently fitted a wrong value resistor in his circuit. The whole circuitry began output a pulse with a steady pace, just like a beating heart. This was the discovery of the first implantable rhythm maker. This pacemaker basically consists of a blocking oscillator. A blocking oscillator is a simple configuration of discrete electronic components which produce a free running (moving smooth and uninterrupted), signal and consist of only a resistor, a transformer and one amplifying transistor. It is shown in figure 6 below. Here the target of blocking oscillator is to produce a narrow pulse. The transistor of the blocking oscillator is normally cut-off between non conduction phase of pulses and conducting during the time that a pulse is generated. The operation of the blocking oscillator during a single cycle can be classified into three phases, turn on period, pulse period and relaxation period. Such a pacemaker is also named asynchronous pacemakers Figure 3: Pacemaker and leads Functionally, a pacemaker comprises at least three parts: a electrical pulse generator, a power source (battery) and an electrode (lead) system as indicated in figure 4 [3]. Power Source Pulse Generator Electrodes Figure 4: Basic pacemaker functional block diagram 3. FIRST IMPLANTABLE PACEMAKER Figure 6: Circuitry of first implantable pacemaker 117 Proceedings of The 20th World Multi-Conference on Systemics, Cybernetics and Informatics (WMSCI 2016) 4. DEMAND PACEMAKER Because they are set at fixed value and do not change with demand of the patient. The rate of asynchronous pacemaker may be altered by the physician, but once set it will continue to generate an electric pulse at regular intervals. Most are set at 70 to 75 beats per minute. Later in 1964 Berkovits invented a demand pacemaker. Demand pacemaker provides electrical impulses only in the absence of natural heart beat. Other important aspect of the demand pacemaker is the life span of the battery because it is only activated when pacing stimulus is needed [27]. Fig 7: Block diagram of demand pacemaker [30] The demand pacemakers are designed by adding a sensing amplifier to the asynchronous pacemakers so that it can detect congenital heart activity. This synchronous pacemaker has rate responsive pacing modalities in respect to physiological situations and pathological conditions [27]. Injecting a gene TB-18 into the heart can convert heart muscle cells to pacemaker cells that can initiate a heartbeat. This method could be useful for certain patients, such as those who develop infections from electronic pacemakers and need to have the devices temporarily removed, or with life-threatening heart disorders who cannot have an electronic pacemaker implanted. So far this technique is applied on animals and now the research of inducing this gene into human body is in progress [26]. 5. LEADLESS PACEMAKER The entire pacemaker discussed above follow a surgical cleavage in the chest under the collar base where the pacemaker enduringly placed in a pocket inside the skin. The surgeon then embeds leads from pacemaker through the veins into the right ventricle. These leads convey electrical pulses that expedite the heart to beat normally [28]. Contradictory to the Conventional pacemakers, leadless pace meters are placed directly into the heart without any surgical cleavage and passing on leads. The leadless pace meter are much minor in size. It is a less invasive approach. It consists of a pulse generator that includes a battery and a steroid eluding electrode that sends the pulses to the heart whenever it senses irregular heartbeats. 7. CONCLUSIONS Artificial pacemakers are the electronic devices that stimulate the heart by generating electrical impulses to restore or maintain the normal rhythm. It controls the pumping action of the heart restoring the communication between the atria and ventricles; therefore it increases the survival capacity tremendously. It is used to meet the challenge of branchardia, tachyarrhythmia. It has the sensor which itself maintains the level of periodic signal. It basically performs the following function: Stimulate cardiac depolarization Sense intrinsic cardiac function Respond to increased metabolic demand by providing rate responsive pacing Provide diagnostic information stored by the pacemaker The pacemaker technology is an active area of research. The field is developing each year, starting from a lab setup of huge pacemaker to the implantable lead pacemaker. Then the lead less pacemakers arrived and now the biological pacemakers are making their approach. There is also some risk or disadvantages. Sometimes the risk factor arises due to high threshold of cardiac excitation, battery failure or electromagnetic interference. Sometimes the air on bubble occurs in the space between lungs and chest wall. The perforation of the heart might also take place. But new Figure 8: Leadless Pacemaker [29] 6. BIOLOGICAL PACEMAKERS 118 Proceedings of The 20th World Multi-Conference on Systemics, Cybernetics and Informatics (WMSCI 2016) researches are in progress to overcome the stated problems regarding artificial pacemaker. [12] Zhihao Jiang, Rahul Mangharam,‟ Modeling Cardiac Pacemaker Malfunctions With the virtual Heart Model, University of Pennsylvania, scholarly commons,2011. 8. ACKNOWLEDGEMENTS [13]B. Fuertes and J. Toquero et. al. Pacemaker Lead Displacement: Mechanisms And Management. Indian Pacing Electrophysiology, Journal, 2003. I am very grateful to Dr. Faisal Qadir of The National Institute of Cardiovascular Diseases NICVD, for his support and guidance [14]Z. Jiang, M. Pajic, A. T. Connolly, S. Dixit, and R. Mangharam. Real-time Heart Model for Implantable Cardiac Device Validation and Verification. 22st Euromicro Conference on Real-Time Systems, (IEEE ECRTS), 2010. 9. REFERENCES [1] Guytan Arthur C, Hall John E (2006) Text book on Medical physiology 11th edition, elsevier, Philadelphia. [15]Z. Jiang, M. Pajic, and R. Mangharam. Model-based Closed-loop Testing of Implantable Pacemakers. In ICCPS‟11: Proceedings of the ACM/IEEE Second International Conference on Cyber-Physical Systems, April 2011. [2] Daniel Mercader, „Artificial Pacemakers: Why we need them to be compatible with MRI‟, University of Pittsburg. [16]Z. Jiang, A. T. Connolly, and R. Mangharam. Using the Virtual Heart Model to Validate the Mode Switch Pacemaker Operation. 32nd Annual International Conference of the IEEE Engineering in Medicine and Biology Society, (IEEE EMBC‟10), 2010. [3] The Evolution of Pacemakers: An Electronics Perspective, published in Ultra Low- Power Biomedical Signal Processing, An Analog Wavelet Filer approach for Pacemaker, Haddad, 978-1-4020-9072-1, Springer. [4] Yu-Feng Hu et.al, Biological pacemaker created by minimally invasive somatic reprogramming in pigs with complete heart block, Science Translational Medicine 16 Jul 2014:Vol. 6, Issue 245,pp.245ra94,DOI:10.1126/scitranslmed.3008681. [17]M.E. Josephson. Clinical Cardiac Electrophys. Lippincot Williams and Wilkins, 2008. [18]PACEMAKER System Specification. Boston Scientific. 2007. [5] Daniel Halperin etal. , Pacemakers and Implantable cardiac Defibrillators: Software Radio attacks and Zero Power Defenses, IEEE Symposium on Security and Privacy, 2008. [19] W. G. Stevenson and K. Soejima. Recording techniques for clinical electrophysiology. J Cardiovasc Electrophys., 2005. [20]R.N. Fogoros. Electrophysiologic Testing. Wiley, 1999. [6] RR Bigelow WG, Callaghan JC, Hopps JA.,General hypothermia for experimental intracardiac surgery;the use of electrophrenic respiration an artificial pacemaker for cardiac standstill and radio-frequency rewarming in general hypothermia. ,Ann Surg. 1950 Sep;132(3):531-539. [21]D. Wei et. al. Computer Simulation of Supraventricular Tachy-cardia with the Wolff-Parksinson-White Syndrome using Three-dimensional Heart Models. J. of Electrocardiology, 23(3), 1990. [7] Endresen,L.P,etal.‟Limit Cycle Oscillations in Pacemaker Cells, Biomedical Engineering, IEEE Transactions vol 47, issue 8,1134-1137 [22]D. M. Harrild and C. S. Henriquez. A Computer Model of Normal Conduction in the Human Atria. Circ Res, 87(7), 2000. [8] Hayes DL. Indications for permanent cardiac pacing. 2014 Jul 14 [cited 2015 Feb 5]. [22]N. Virag, J Vesin, and L. Kappenberger. A Computer Model of Cardiac Electrical Activity for the Simulation of Arrhythmias.PACE, 21(11), 2006. [9] Pacemakers [Internet]. In: Heart rhythm health resources. Ottawa: Canadian Heart Rhythm Society; 2015. [23]J. Beaumont et. al. A Model Study of Changes in Excitability of Ventricular Muscle Cells. Am J Physiol Heart Circ Phys.), 1995. [10]Kirkfeldt RE, Johansen JB, Nohr EA, Jorgensen OD, Nielsen JC. Complications after cardiac implantable electronic device implantations: an analysis of a complete, nationwide cohort in Denmark. Eur Heart J [Internet].2014 May [cited 2015 Feb 5];35(18):1186-94. Availablefrom:http://www.ncbi.nlm.nih.gov/pmc/articles/P MC4012708 [24]Medtronic ViP-II Virtual Interactive Patient: User‟s Manual Soft-ware v1.5. Rivertek Medical Systems, 2006. [25]Case study # 9 The Artificial Heart Cost, River and Benefits “Appendix A” by Thomas Preston. 2014,doi:10.1161/CIRCULATIONAHA.113.006987 [11]Hauser RG, Hayes DL, Kallinen LM, Cannom DS, Epstein AE, Almquist AK, et al. Clinical experience with pacemaker pulse generators and transvenous leads: an 8year prospective multicenter study. Heart Rhythm.2007 Feb;4(2):154-60. [26]Amir Weissman et al. „Human Embryonic and Induced Pluripotent Stem Cell–Derived Cardiomyocytes Exhibit Beat Rate Variability and Power-Law Behavior‟, Circulation. 2012;125:883-893, published online before 119 Proceedings of The 20th World Multi-Conference on Systemics, Cybernetics and Informatics (WMSCI 2016) print January18,2012, doi:10.1161/CIRCULATIONAHA.1 11.045146 [27]J Sperze, „State of the art of leadless pacing‟, Europace. 2015;17:1508-1513 [28]FVY Tjong,‟Postmortem Histopathological Examination of a Leadless Pacemaker Shows Partial Encapsulation After 19 Month‟,Circ Arrhythm Electrophysiol. 2015;8:1293-1295 [29]Dwight Reynolds et al., „A leadless intracardiac transcatheter pacing system‟, The new England Journal of Medicine, November 9, 2015DOI: 10.1056/NEJMoa1511643 [30]Patent US3999556-Demand Cardiac Pacemaker. 120