Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
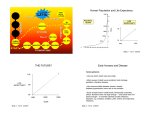
The Contribution of Personal Health Services to Longevity, Population Health and Economic Growth Link between Health and Economic Sectors Economists show links between (1) flows of funds and (2) flows of goods and services. These can be linked to the health sector. Allocations to health care one of the allocation decisions—affects quantity and mix of resources available for health care. Investments in health care in turn affect growth of economy Fig. 16.1. Links between Health and Economic Sectors Economic Sector 1 ○ 2 ○ Health Care Financing (Input) 4 ○ 3 ○ Population Health (Output) Health Sector = Flow of dollars = Flow of goods and services = Feedback connection 1. Affecting macroeconomic outcomes 2. Boosting economic performance 3. Increasing employment and income 4. Changing disease patterns Funds Flows from Economic Sector Components Out-of-pocket spending by individuals Private health insurance General tax revenue Earmarked tax revenue Relationship between Improved Health and Longevity and Economic Growth Two important questions: (1) How much of the long-term gains in population health can be attributed to provision of personal health care services? (2) What are the major pathways through which health gains boost economic performance? Some Research Suggests That Spending on Health Care has Minor Impact on Economic Growth Rand Health Insurance Experiment: little effect of health insurance on personal health, but observational period short There is much more variation in share of GDP devoted to health care than there is variation in personal health among countries. Text disagrees that little effect of health care on economic growth for several reasons. Why Evidence on Previous Slide May be Misleading There are many dimensions of personal health, not only mortality. There are important lags between investments in health and the return on such investments—takes decades for many such investments to yield return. Other factors affect health outcomes, not just per capita GDP. Longitudinal and Time Series Studies These studies show impacts of health care use on health outcomes and other outcomes --effects of health care on demographic structure— people are productive for longer, which in turn influences work hours and labor productivity per hour; when healthier people learn more while in school. --reductions in infant and preschool child mortality decrease numbers of births per women in child-bearing ages. Effects of Health Care Financing on National Economies: Savings Behavior Reduced precautionary savings when people are covered by health insurance. Why? Effects on macroeconomy? Precautionary savings inefficient way for household to protect against expenditure risk. Why so? Crowding out of private savings, private health insurance, and work when public means-tested health insurance, e.g., Medicaid, provided. Explain why this is so. Effects of Health Care Financing on National Economies: Labor Market Outcomes Employer-based health insurance and “job lock.” What is job lock and why does it represent a source of inefficiency in an economy? Effects of employer-provided health insurance coverage on personal retirement decisions Effects of provision of employer-provided health insurance as a fringe benefit on wage compensation Effects of such insurance on labor force participation rate of women Effects of Health Care Financing on National Economies: Welfare Loss of Taxation Two sources of general tax revenue: (1) direct taxes, e.g., personal and corporate income taxes; and (2) indirect taxes, e.g., excise taxes. Direct taxes on personal income create deadweight loss through distortion of labor supply decision. Why? Excise taxes affect individuals’ consumption choices because consumption is taxed relative to other choices, e.g., savings, consumption of goods and services not subject to the excise tax. Consumer’s work–leisure choice distorted as well. Empirical evidence Fig. 16.2. Excess Burden of an Indirect Tax $ Discussion of Fig. 16.2 Since the sum of losses in consumer surplus and producer surplus (A+B+C+D) exceeds the amount of revenue collected (A+C), there is deadweight loss in amount (B+D). Summers (1989): Increase of $1 in tax revenue leads to deadweight loss from $1.07-$1.33. Deadweight Loss and Payroll Tax Most countries collect revenue for health insurance from payroll tax Impact of payroll tax on economic activity depends on tax incidence, i.e., who bears the tax Is the tax shifted forward to consumers in the form of higher product prices? Forward shifting Is the tax shifted backward to employees in the form of lower compensation? Backward shifting Is the tax cost absorbed by employers? No shifting Empirical Evidence on Payroll Tax Shifting Most research indicates backward shifting—thus, little/no adverse impact of payroll tax on employment levels Secular Trends in Expenditures on Personal Health Care Services At single point in time, there is considerable variation in health expenditures among OECD countries, both in levels and as percent of GDP. Trends in expenditures are similar among OECD countries. Determinants of Personal Health Expenditures (Countries) National income (most important determinant) Population aging Increased health insurance coverage (related to national income changes) Technological change—but hard to quantify Hall and Jones (2007): Perhaps Countries Like the U.S. Are Not Spending Too Much on Health After All. Theory: marginal utility of consumption of goods and services other than health declines with increased consumption. After all, one does not get that much utility out of the third big screen TV or the 14th trip in a year. But the marginal utility of health care services do not decline. More services increases longevity. So there are more periods during which to consume other goods and services. Hence, there is good reason that more affluent countries spend more of health services. Secular Trends in Health Outcomes At single point in time, there is substantial variation in life expectancy among OECD countries. Life expectancy has increased in almost all countries. There is appreciable variation in life expectancy within countries—health disparities. Determinants of Mortality Cutler et al (2006) attributed longevity gains to improvements in (1) nutrition. (2) public health, and (3) vaccination and medical treatment. Authors emphasized important role of technological change in health improvements. Contributions of Personal Health Care Services to Improved Population Health: Conceptual Framework Health production function as described in Chapter 2 See Fig. 16.3. “Process” versus “product” innovations in general and applied to health care Fig. 16.3. Health Production Function in a Static and Dynamic Context Output (Health) C H2 Health gains due to technology change B H1 H0 0 C’ Health Production Function at Period 1: H(M; 1) A M0 Health Production Function at Period 0: H(M; 0) Health gains due to medical input M1 Input (Health Care) Contributions of Personal Health Care Services to Improved Population Health: Empirical Evidence Auster et al. (1969) Rand HIE Data from 175 countries. Figs. 16.4 and 16.5: get different shapes of production function for highversus low-income countries Fig.16.4. The Relationship between Annual Health Expenditures Per Capita Population and Health Outcomes in High-Income Countries Life Expectancy 85 80 75 70 65 60 55 50 45 40 0 1000 2000 3000 4000 Health 5000 Expenditure Sources: Data for annual health expenditures and life expectancy are from World Bank Development Indicators (The World Bank Group. 2009). Both health expenditures and life expectancy at birth are for the year 2000 and health expenditures are measured in constant 2000 US dollars. Note: High-income countries indicate countries with a GDP per capita greater than the 50th percentile of world income distribution. Fig.16.5. The Relationship between Health Expenditures per Capita Population and Health Outcomes in Low-Income Countries Life Expectancy 80 75 70 65 60 55 50 45 40 35 0 20 40 60 80 100 120 140 Health Expenditure Sources: Data for health expenditures and life expectancy are from World Bank Development Indicators (The World Bank Group. 2009). Both health expenditures and life expectancy at birth are for the year 2000 and health expenditures are measured in constant 2000 US dollars. Note: Low-income countries indicate countries whose GDP per capita are less than 50th percentile of world income distribution. Attributing Health Improvements to Technological Change: Methodological Approaches Quantifying influence of technological change on health and longevity is challenging task 3 approaches --Disease approach: analysis of data on individuals focusing on single disease or therapeutic procedure --Proxy variable approach: find a proxy variable for technological change such as cumulative number of new drugs available --Accounting method Disease Approach Case studies for e.g. heart attack treatment, treating low-birthweight infants, breast cancer Treatment substitution versus treatment expansion effects Skinner et al. (2006) evidence that benefits from treatment for a specific disease may decrease over time Proxy Approach Methodological problems --quantifying health overall (more difficult than when dealing with a single disease) --selecting an adequate proxy --omitted variables bias Applications Accounting Method Parse out effect of health care technological change on health improvement from the other factors that led to health improvement Example: Cutler et al. (2006): Concluded that > 40% of longevity gain in the U.S. attributable to technological change in medicine Contribution of Improved Health to Economic Growth Direct Effect on Productivity Bhargava et al. (2001) used aggregate data on adult survival rates (ASRs) to measure health and estimate impact of change in ASR on economic growth. Found a positive effect of ASR on growth, but not consistent patterns. Bloom et al. (2004) used life expectancy as proxy for health. Found that each extra year of life expectancy leads to increase in national output of 4%. Jamison et al. (2004) also found effect but found that stock of physical capital and educational attainment of country’s population had larger effects on economic growth. Weil (2007) studied gaps in national income between rich and poor countries. Concluded that health differences explained 10% of national income gap. Indirect Effects Operating through Fertility, Education, and Saving If children more likely to die, parents tend to have more children so that they will have family support when old. When children have a higher probability of reaching adulthood, there is greater incentive for families to invest in children’s education. With longer period of expected retirement, families save more during pre-retirement for consumption during retirement years. Other Indirect Effects Good health during children may lead to more creativity in adulthood. Improved child and maternal health may improve children’s ability to cope with stress and adapt to new technology as adults. Countries with higher levels of population health tend to have lesser income inequality. Contested Issues Health affects economic activity but economic activity may also affect health, but this not always so, e.g., China before and after 1978. Are health differences among countries becoming smaller or larger? Health Sector as Job Machine Health sector a major employer Channels: (1) demand for labor to work in health sector a derived demand; (2) countries promote health industries, e.g., pharmaceutical manufacturer as source of employment with products traded globally Economic Growth and Disease Patterns With economic growth comes reductions in death caused by respiratory and digestive diseases In high-income countries which have experience above reductions historically, see reductions in deaths due to diseases of nervous system and sense organs (e.g., multiple sclerosis, Parkinson’s disease, stroke); and heart and circulatory conditions over time Unemployment and Health Ruhm (2000): health improves as unemployment increases. See Fig. 16.6. Why this relationship? --time prices fall during recession, lowers price of health investments --fewer work-related accidents during recessions Fig. 16.6 Total Mortality and Unemployment Rates in the United States Source: Ruhm (2000)