Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Sociality and disease transmission wikipedia , lookup
Kawasaki disease wikipedia , lookup
Vaccination wikipedia , lookup
Childhood immunizations in the United States wikipedia , lookup
Behçet's disease wikipedia , lookup
Transmission (medicine) wikipedia , lookup
Infection control wikipedia , lookup
Ankylosing spondylitis wikipedia , lookup
Rheumatoid arthritis wikipedia , lookup
Chagas disease wikipedia , lookup
Germ theory of disease wikipedia , lookup
Schistosomiasis wikipedia , lookup
Globalization and disease wikipedia , lookup
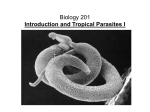
Global Health Landscape Lymphatic filariasis (LF) Background information • What isLymphatic filariasis (LF)? Lymphatic filariasis (LF), also known as elephantiasis, is caused by parasitic worms and leads to severedisfigurement of the extremities. While not directly life-threatening, LF is among the world’s leading causes of permanent and long-term disability. Those infected are disabled in their most productive stage of life, resulting in an economic and psychosocial burden on afflicted individuals, families, and communities. • Global burden More than 120 million people are infected with LF; over 40 million are seriously disfigured by the disease. It is estimated that 1.3 billion people are at risk for the disease. • Geographic distribution LF is endemic in 83 countries. One-third of the people infected with LF live in India, and one-third live in Africa. Most of the remaining cases are distributed throughout South Asia, the Pacific, and the Americas. • Causative agent/transmission The thread-like, parasitic worms Wuchereria bancrofti and Brugia malayi cause lymphatic filariasis. Adult worms lodge in the lymphatic system, where they live for four to six years and produce millions of immature microfilariae (minute larvae) that circulate in the blood. The parasites are transmitted to a mosquito vector when its blood meal includes microfilariae. Inside the mosquito, over the course of one to thee weeks, the larvae mature blood meal. Presentation The worst symptoms of the chronic disease generally appear in adults. Elephantiasis of an entire leg, arm, the vulva, or the breast—swelling up to several times normal size—is common. In endemic communities, some 10 to 50 percent of men suffer from genital damage, especially formation of hydrocoeles (fluid-filled balloon-like enlargements of the sacs around the testes) and elephantiasis of the penis and scrotum. Once hydrocoele formation has begun, the most effective way to deal with it is generally surgery, but this solution is tooexpensive for the majority of people affected by the disease. Trends The Global Programme to Eliminate Lymphatic Filariasis has targeted elimination of LF by 2020. Results from the program’s first eight years (2000-2007) are encouraging. Yearly, single-dose mass drug adminstration has reached 570 million individuals in 48 LF-endemic countries, protecting an estimated 9.5 million people with subclinical disease from progressing to clinical disease and preventing disease in 6.6 million newborns. Existing Products Drugs Combination Treatment — Albendazole with Diethylcarbamazine (DEC) or Ivermectin Vaccines Diagnostics None Microscopy • Difficult because the parasites often have a “nocturnal periodicity” that restricts their appearance in the blood to the hours between 10 p.m. and 2 a.m. • Use of single doses of two drugs administered concurrently is 99 percent effective in removing microfilariae from the blood for a full year after treatment • Does not kill adult worms • Current standard of care is to treat children annually for five years to prevent disease and break the chain of infection • Treatment with DEC can cause serious side effects if onchocerciasis is also present, as occurs in certain African countries; ivermectin is used as an alternative in these regions BinaxnOW® Filariasis Test • Antigen detection test • Rapid; requires 10 minutes • Detects antigens of W. bancrofti in whole blood, serum, or plasma • Simple, very sensitive, and specific • Expensive to use; generally used to identify populations at risk rather than individual diagnosis New Product Needs Drugs • Kills adult worms (macrofilaricidal) and reduces swelling • Decreases necessity of repeated, annual treatment; inhibits microfilariae production Vaccines Diagnostics • Prevents establishment of infection by microfilariae • Further development of diagnostics for B. malayi • Adapt existing serologic assays to work with oral fluids or urine Pipeline Drugs Discovery Pre-Clinical Clinical Phase I Clinical Phase II Clinical Phase III Anti-Wolbachia Consortium: Liverpool School of Tropical Medicine/CombinatoRx/New England Biolabs, and others (anti-Wolbachia treatments) Market Opportunities • The critical issues for LF are delivery into remote, endemic areas and maintenance of treatment over many years to reduce adult disease and break the chain of transmission. Currently, all drugs used to treat LF are donated. • Many current LF treatments are also effective against other diseases common in the developing world; new drugs might likewise have multiple markets. Development Issues Drugs • Recent evidence (June 2007) suggests that ivermectin resistance is emerging in onchocerciasis (a filarial worm disease); this observation reinforces the need for new drugs in the event resistance appears in LF Vaccines • Lack of an in vitro culture system for filariae • Absence of tools for easy genetic manipulation • Need for improved animal models Diagnostics • The major challenge is to reduce cost of each diagnostic to below $1 Additional Information General Disease Links • World Health Organization (WHO) • Centers for Disease Control and Prevention (CDC) Key Organizations • • • • Anti-Wolbachia Consortium The Carter Center The Global Alliance to Eliminate Lymphatic Filariasis Special Programme for Research and Training in Tropical Diseases (TDR) Important Papers • Galvez Tan, JZ. The elimination of lymphatic filariasis: A strategy for poverty alleviation and sustainable development—perspectives from the Philippines. Filaria Journal 2:12 (2003) • Johnston, KL, and Taylor, MJ. Wolbachia in filarial parasites: Targets for filarial infection and disease control. Curr Infect Dis Rep 9:55-9 (2007) • Molyneux, D. Lymphatic filariasis (elephantiasis) elimination: A public health success and development opportunity. Filaria Journal 2:13 (2003) • Ottesen, EA, et al. The global program to eliminate lymphatic filariasis: Health impact after 8 years. PLoS NTD 2:e317 (2008) • Perera, M, et al. Neglected patients with a neglected disease? A qualitative study of lymphatic filariasis. PLoS NTD 1:e128 (2007) • Towards a strategic plan for research to support the global program to eliminate lymphatic filariasis: Summary of immediate needs and opportunities for research on lymphatic filariasis. Supplement 5 to AJTMH 71 (2004) ©2010 BIO Ventures for Global Health.