Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
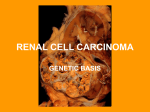
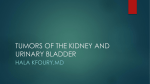
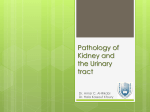
24-2-2014 Pathology/Sheet 4 Rawan Al-Majali Rapidly Progressive Glomerulonephritis (RPGN) Rapidly progressive glomerulonephritis is a renal disease that comes under the heading of nephritic syndrome, which was discussed in the previous lecture. And as a reminder, nephritic syndrome is a component of hematuria, renal impairment, and hypertension. And the causes are post-infectious or post-streptococcal glomerulonephritis, IgA nephropathy, and the last is a syndrome of symptoms called Rapidly Progressive Glomerulonephritis. From the name, there is a rapid progression to renal failure. And if untreated, will lead to death. If any of the glomerunephritis diseases that we talked about persisted for a longer time, or left untreated, Rapidly Progressive Glomerulonephritis comes as an extension for the condition and shows more advanced features. For example IgA nephropathy can lead to RPGL, and postinfectious glomerulonephritis if continues may reach a level of a rapidly progressive glomerulonephritis. So it is not a single disease, it is an entity of different categories. The main effect of RPGN is a rapid deterioration, progressive loss of renal function, with some features of the nephritic syndrome. So it is basically a nephritic syndrome, a severe one, plus minus nephrotic range proteinuria (so It can be presented as nephrotic-nephritic syndrome). Histologic findings observed in patients with RPGN, show glomerular crescents. To give you an idea about the crescent formation; it is when a severe injury to the kidney initiates the proliferation of parietal epithelial cells (the lining of Bowman’s capsule), in addition to the presence of inflammatory infilirate of monocytes and macrophages, and the deposition of fibrin and fibrinogen. All together, change the normal structure of the gomeruli and constitute a crescent-shaped mass as shown in the picture. And this is the main feature histologically for RPGN. Crescents can be seen in post-streptococcal infection or after any severe injury, but if it was very much pronounced and extensive, it is called crescentic glomerulonephritis, especially if it was after a severe nephritic syndrome like RPGN. Rapidly progressive glomerulonephritis or crescentic glomerulonephritis can be classified into three types: 1) Type I: antiglomerular basement membrane antibody. 2) Type II: Immune complex mediated RPGN. 3) Type III: Pauci immune RPGN. Page 1 of 9 24-2-2014 Pathology/Sheet 4 Rawan Al-Majali Type I (anti-glomerular basement membrane antibody): Cause: is it characterized by the production of antibody (of IgG type) reacting against the glomerular basement membrane, resulting in complement activation and deposition, which leads up to crescent formation. Antibodies could also react with the basement membrane of the lung alveoli, so patients with nephritic syndrome (crescentic glomerulonephritis) come presented with lung hemorrhage. This syndrome is called Good Pasture syndrome, a syndrome of Renal impairment and lung hemorrhage. Immunoflorescence pattern: IgG’s are visualized depositing linearly along the whole glomerular basement membrane. Treatment: Type I can be treated by plasmapharesis (washing out the basement membrane antibodies from the plasma, so they can no longer react with the basement membrane). Type II (Immune complex mediated): Cause: this type is due to the deposition of immune complexes in the kidney, which could be circulating, or the antigen is already implanted in the kidney (not in the basement membrane) and a circulating antibody comes and react with the antigen forming an immune complex that will deposit there. Most of these cases are associated with other autoimmune diseases, like Systemic lupus erythematosis, and other Antigen-Antibody complex mediated glomerunepritis (like post-streptococcal GN and IgA nephropathy). So this explains one way how nephritic glomerulonephritis diseases can progress into crescentic GN or RPGN. Immunoflorescence pattern: Lumpy bumpy; deposition of Igs everywhere. Treatment: these individuals cannot be helped with plasmapharesis, because there is no single antibody that attacks the kidney tissues to be removed and reverse the event. (like glomerular basement membrane antibody for example). But they benefit from immune mediated therapy, they’re given corticosteroids to suppress the immunity and the immune complex formation. Type III (Pauci-Immune): Patients have ANCA positive serum (have Anti Neutrophil Cytoplasmic Antibody in their serum). There are neither anti GBM antibodies nor immune complexes. But there is another antibody (ANCA) although it is not involved in the reaction or deposition in the kidney. These patients Page 2 of 9 24-2-2014 Pathology/Sheet 4 Rawan Al-Majali have vasculitis, an immune mediated reaction in vessels which can be associated with crescentic GN (RPGN). The three types present the same clinical presentations; severe nephritic syndrome, hematuria, hypertension, renal impairment, azotemia, high creatinin, oliguria, and proteniuria that can approach the nephrotic syndrome. The prognosis is very severe and the patient needs dialysis or may need transplantation in cases of very severe kidney damage. Prognosis is related to the number of crescents. If we receive the biopsy and 80% or more of the glomeruli show crescent formation, this means the prognosis is very bad and the patient needs transplantation. Tumors of the Renal system Tumors of the renal system are categorized into tumors of the kidney -that arise in the cortex and medulla, named collectively Renal Cell Carcinoma RCC- and tumors of the collecting system, any place lined with urothelial lining, starting from the renal calyces, renal pelvis, and down to the ureter, urinary bladder, and urethra. All of these are lined with urothelial lining, which is transitional epithelium. And they show the same type of tumor; urothelial carcinoma. Renal cell carcinomas (RCC): Renal cell carcinomas account for 2-3% of all the tumors in adults, there are several subtypes of RCC, based mainly on how the cancer cells look under a microscope. 1. Clear cell carcinoma: This is the most common form, and it’s responsible for 65% of all renal cell carcinomas. From the name, the cells that make up the cancer appear clear or pale when seen under the microscope. They can occur in a sporadic fashion or a familiar inherited pattern, the former being more common than the latter. But in both cases, the gene that is involved is called VHL gene (von Hippel-Lindau). Genetic aspect: Von Hippel-Lindau gene is present on chromosome 3, and encodes for VHL protein, which plays a role in the degradation of hypoxia inducible factors (HIF). In patients with abscent or deleted VHL gene, VHL protein is missing and this manifests on the cellular function level, so as a result, hypoxia inducible factors build up in cells, stimulating them to divide abnormally, and they also trigger the production of blood vessels by the activation of vascular epithelial growth factor (a growth factor that normally promotes the growth of new blood vessel “angiogenesis”), because as you know blood supply is a very important element for cancer cells to sustain their life. In the familial cases, they are associated with VHL syndrome, a group of clinical symptoms in many different parts or organs of the body. Page 3 of 9 24-2-2014 Pathology/Sheet 4 Rawan Al-Majali Morphology: most of RCC’s are solitary, means single or one. Usually they are large tumors, and show areas of cystic formation, areas of hemorrhage, and areas of necrosis. The tumor looks ugly, with colors ranging from tan to brown to yellow. It starts in the renal tissue, and as it enlarges it invades the adjacent collecting system and the renal pelvis. And in severe cases, if the patient is unfortunate it may invade the renal vein, which is a very characteristic feature of renal cell carcinomas. Having done so, they continue to the Inferior Vena Cava and to the right side of the heart, so they metastasize by this way. Clear cell carcinomas are categorized into low grade, intermediate, and high (grade 1,2 and 3). Grading: the degree of differentiation, how much the tumor resembles the normal tissue. A lower grade indicates a better prognosis. This picture shows a bad prognostic feature (renal vein invasion) of a large tumor, at the upper pole of the kidney. Notice the thrombosed area (tumor clot) under the large mass in the dilated renal vein. (prognosis: predicting the outcome of the disease) Slide #6: this is what you can see histologically, cells with clear lipidized cytoplasmic. The cells look white under the LM, some cells may show granular pinkish eosinophilic cytoplasm, but most of the tumors show clear cytoplasm. 2. Papillary Renal cell carcinoma: These cancers form little finger-like projections (called papillae), they are much less common than the clear cell RCC, constituting 10-15% of all tumors. In contrast to clear cell RCC, these appear small and multi-focal, and sometimes bilateral. Genetic aspect: occur in either a sporadic fashion, or familial fashion. But the responsible gene here is different than that of clear cell RCC, and it is called the MET gene or MET protooncogene, which is present on chromosome 7 (oncogenes: genes that promote tumor growth) MET proto-oncogen, is a tyrosine kinase receptor, for a growth factor called hepatocyte growth factor. Not only the gene that is different, but also the problem or mechanism related to the disease. In clear cell RCC there was deletion or absence of the gene, but for Papillary RCC, we have extra copies of MET gene, and this takes the probability of two; either there is an extra copy of chromosome 7 (trisomy 7), or a duplication of the same chromosome due to mutation (duplication Page 4 of 9 24-2-2014 Pathology/Sheet 4 Rawan Al-Majali mutation). Either one of the mechanisms constitute the familial pathway of the disease, or the inherited pattern (at the germ level). In the sporadic cases, we might have an extra copy of the chromosome (at the genetic level. Mutations during life, due to any abnormal division of the cell, that produce an extra copy of chromosome 7, which carries an extra copy of MET gene). Papillary RCC’s, originate from the proximal tubular epithelial cells; gene abnormality leads to an abnormal proliferation of the proximal renal tubular epithelial cells. Morphology: papillary growth pattern, tends to be bilateral and multiple. Show areas of cystic formation, hemorrhage, and necrosis, but do not reach the limit of clear cell RCC’s which is very cystic, necrotic and hemorrhagic. They can have clear cells, but most commonly the cells have a pinkish cytoplasm, and the characteristic feature is papillary formation. Slide #9: microscopic slide, shows papillae formation. The course of the papillae here contains foamy macrophages. 3. Chromophobe Renal carcinomas: The least common (5% of renal carcinomas) type, they originate from different cells called the intercalated cells of the collecting duct (the last part of the nephron) and in general, they have a good prognosis. Genetic aspect: there are different pathways, different deletions on different chromosomes, so it is neither involving the VHL gene nor MET gene. Morphology: the main characteristic feature is a clear halo around the nuclei. As you can see in slide #12: pinkish cytoplasm, perinuclear halo, prominent cell membranes between adjacent cells. Ultrastructurally under the electron microscope: numerous macro-vesicles, responsible for the halo visualization. Clinical course of Renal Cell Carcinomas: The different types of RCC’s were classified according to the microscopic or histologic findings, but they all have the same clinical presentation. The classical triad of Renal Cell Carcinoma: Painless hematuria (can be macroscopic or microscopic), palpable renal mass, and a flank or loin pain. But not all the patients come with these three symptoms or triad, which poses a problem in diagnosing the case. Page 5 of 9 24-2-2014 Pathology/Sheet 4 Rawan Al-Majali Most of the patients, 50% of them, are presented with painless macroscopic hemturia (gross hematuria), and this is the most common presenting symptom. Painful hematuria indicates more benign diseases, like infections, and stones. But Painless hematuria is an alarming feature, especially in elderly patients. It is cancer until proven otherwise. In Renal cell carcinomas, the presence of the tumor or overgrowing cells, accompany overfunctioning condition as well, so the kidney secretes high levels of erythropoietin which in turn increases hemoglobin levels (polycythyemia). The other thing is that the production of tumor necrosis factors causes an elevation of the body temperature. So two important manifestations of RCC’s other than the renal effects, are fever and polycythemia. Paraneoplastic syndrome: it is when you have a tumor, and you have associated hormonal imbalance or hormonal manifestations that cannot be explained by the hormones that are natively produced by this tumor, because it is supposed to secrete the same set of hormones that are secreted from the original tissue it resulted from. This is explained for example in a patient with lung tumor, and is presented with cushing syndrome (high levels of corticosteroids). This is a paraneoplastic syndrome because the lung normally does not secrete ACTH or cortisone. Also, when RCC patient has hypercalcemia because of the production of a parathyroid-like material, he’s said to have a paraneoplastic syndrome, whereas being presented with polycythemia, is a predictable or a reasonable state because erythropoietin is produced normally by the kidney. So another set of clinical features could include: hypertension, masculinization (male sexual characteristics), feminization (female sexual characteristics), cushing syndrome and hypercalcemia. All paraneoplastically facilitated. (masculinization and feminization are attributed to the production of sex hormones from the tumor). There is a tendency for RCC (especially clear cell RCC) to go to the lungs and bones, unknown why. They can go everywhere but these two sites the are the most preferred. Tumors of the Renal Collecting System Renal collecting system constitutes renal calyces, pelvis, ureter, urinary bladder and the urethra. And they’re all lined with transitional epithelium. The epithelial tumors arising from the transitional epithelium have the same characteristic features. Tumors above the urinary bladder are uncommon, the most common are those affecting the urinary bladder, they can occur anywhere along the collecting system but most commonly in the urinary bladder, where they tend to be large and fungating masses, and stay there without causing symptoms because the urinary bladder is large. If a small tumor developed in the ureter for example, it may cause obstruction because of the small lumen it is encompassed by, and it can cause devastating consequences like hydronephrosis,and pyeloneohritis, while these occurring in the urinary bladder may pass unnoticed for a long period of time. Page 6 of 9 24-2-2014 Pathology/Sheet 4 Rawan Al-Majali Urinary bladder cancer: They account for 7% of cancers, and 3% of deaths in the USA. 90-95% are urothelial carcinomas arising from transitional epithelium or the urothelium, from where It took its name. however, 37% are squamous cell carcinomas. There is a close relationship between Schistosoma (also known as bilharzia disease) and squamous cell carcinoma, because the responsible parasite causes irritation to the urinary bladder, and may lead to squamous metaplasia as a first event, then dysplasia and carcinoma. In Eygpt and Africa this parasitic infection is very common, so it is more likely to see cases in these areas. Urinary bladder tumors are more common in men, and in industrialized countries where exposure to carcinogens is more frequent. And mostly they occur in elderly, between the ages of 5080 yrs. The third type could be adenocarcinoma, where there’s a glandular formation. But it is rare. Pathogenesis: Bladder cancer is not familial, it is usually acquired, and there are many causative agents and carcinogens that correlate with bladder cancer, for example, there is a close association between cigarette smoking and urinary bladder cancer. In addition, β-naphthylamine, drugs like cyclophosphamide (an anti-cancer drug that can cause hemorrhagic cystitis, inflammation of the urinary bladder and urothelial carcinoma), and schistosoma infections -in areas where it is endemic- are important factors in the causation. Urothelial carcinoma and the precursors of urothelial carcinoma: To summarize the tumors of the urinary collecting system, we can have fungating papillary tumors, or flat tumors. And either of them can be non-invasive (not reaching the basement membrane, lamina properia or the muscular wall of the urinary bladder), or invasive tumors, that invade the underlying tissues. For the papillary tumors, they demonstrate a non-invasive tumors, and demonstrate variable degrees of atypia (low grade or high grade) or absence of atypia in the benign conditions. So they are graded according to that to reflect their behavior. (atypia: means atypical features, progressing to carcinoma, like hyperchromatic nucleus and abundance of mitoses) The most common grading system classifies the papillary tumors according the degree of atypia. The first one which is completely benign, called papilloma, it is just a papillary growth, fibrovascular course, covered by normal urothelium, that lacks atypia. The nuclei all look like the normal urothelium but they’re forming papillae. There is no recurrence, it is completely benign. Page 7 of 9 24-2-2014 Pathology/Sheet 4 Rawan Al-Majali The second category is called PUNLMP, and comes in between, that’s why it is called papillary urothelium neoplasm. Could turn into low grade, or couldn’t recur. It is put in gray zone, neither a carcinoma not a benign. The third and forth categories (low-grade/high-grade papillary urothelial carcinoma) are carcinomas, there is an obvious atypia and a prominent growth and papillary formation but there is no invasion to the underlying tissue, so they’re called non-invasive papillary urothelial carcinomas, that can be low grade (degree of atypia is low), and can be high grade ( the tumor is no longer resembling the normal urothelial cells). Slide #19: this is a low grade papillary urothelial carcinoma. In the center; thin fibrovascular course covered by urothelium. The nuclei look large, densely basophilic (hyperchromatic), with high N:C ratio. And if you look carefully at other parts of the tumor you can find increased number of mitoses. The number of layers is also increased, the normal urothelium is three to seven layers only. With high grade, the tumor looks uglier and more aggressive, and the papillae are fused together. Either low or high grade non-invasive carcinomas can invade the underlying tissue, the lamina properia, or the muscle wall of the urinary bladder. The extent to which a tumor has developed, invaded and spread to distant locations, and lymph node metastasis, is expressed or determined by something called cancer staging. And it is the most important prognostic factor, another important prognostic factor is the grade (low grade vs. high grade). Clinical features of invasive and non-invasive carcinomas: Painless hematuria, they have the tendency to recur after excision, especially low-grade and high-grade papillary urothelial carcinoma. Papilloma never recur, PUNLM could recur. That’s why any patient diagnosed with bladder cancer should follow up, by cystoscopy, urine analysis, and ultra sound to monitor for these recurrences. Treatment: -Excision of the tumor and follow up, if it was small and non-invasive. And the excision can be diagnostic (taking biopsy and examining it) or therapeutic (if it is completely excised). -BCG vaccine in the urinary bladder is used for the treatment of the urothelial carcinomas by infusion in the urinary bladder. It causes an intense inflammatory granulamatous reaction that can destroy the malignant cells. -Follow up, and urine analysis. -In severe cases where the tumor is reaching the muscular wall (very high grade tumor), radical cystectomy and chemotherapy. Page 8 of 9 24-2-2014 Pathology/Sheet 4 Rawan Al-Majali Flat tumors, even If they are sometimes flat and non-invasive, are considered high grade from the start. They are called carcinomas in situ. So they may need for cystectomy (removal of the urinary baldder). Page 9 of 9