Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
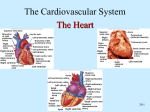
EDITORIAL European Heart Journal (2016) 37, 651–653 doi:10.1093/eurheartj/ehv475 Another jigsaw piece in the complex picture of hormonal regulation of cardiac repolarization Katja E. Odening* Heart Center University of Freiburg, Department of Cardiology and Angiology I, Freiburg, Germany Online publish-ahead-of-print 20 September 2015 This editorial refers to ‘Estradiol regulates human QT-interval: acceleration of cardiac repolarization by enhanced KCNH2 membrane trafficking’†, by L. Anneken et al., on page 640. Albert Einstein once said, ‘The important thing is not to stop questioning . . . It is enough if one tries merely to comprehend a little of this mystery every day’. In this spirit, in their study presented in this issue, Anneken et al.1 tried to add another jigsaw piece in the intriguing and complex puzzle of sex hormones and cardiac repolarization. For quite a while, sex differences in cardiac repolarization, with longer QT intervals in adult women than in men, have been appreciated clinically. This phenomenon can be found in healthy subjects and in patients with inherited long QT syndrome (LQTS) harbouring mutations in repolarizing ion channel genes.2 In addition, changes in QT duration and the concomitant long QT –related arrhythmogenic risk have been observed during the menstrual cycle, pregnancy and the post-partum phase,3,4 strongly suggesting a major role of sex hormones in regulating cardiac repolarization. The more we investigate potential mechanisms underlying these sex hormone effects, however, the more complex is the picture that emerges4 (Figure 1). This may be partly due to the fact that studies have been performed in various species using various hormone concentrations,5 which can exert opposing effects on cardiac repolarization and arrhythmogenic risk,6,7 and partly due to the fact that most studies focus on one ion channel/current at a time without systematically assessing and integrating data on all ion currents. Based on studies in rabbits and guinea pigs, it has been postulated that sex differences in repolarizing voltage-gated rapid delayed rectifier current IKr (HERG/KCNH2) are of major importance for the observed sex differences in cardiac repolarization. Larger IKr current densities have been observed in males than in females due to a testosterone-mediated increase in IKr8 and an oestradiolmediated decrease in IKr,6 causing a longer QT/action potential duration (APD) and a higher propensity of female hearts for long QT –related arrhythmia. Similarly, in human cardiac tissue, reduced mRNA and protein expression of KCNH2/HERG has been demonstrated in females compared vs. males.9 In addition, sex hormone effects on voltage-gated slow delayed rectifier current IKs (increased by testosterone and progesterone10,11) and on L-type Ca2+ current ICa,L (decreased by testosterone and progesterone;7,10 – 12 increased by oestradiol12,13) have been identified. These progesterone effects on IKs and ICa,L and the consecutive QT/APD shortening are thought to mainly account for the observed changes of QT interval during the menstrual cycle and pregnancy. Here, another seemingly diverging piece is introduced to this complex picture by Anneken et al.1 In their detailed, elegantly performed study, they investigate the effect of oestradiol (physiological levels during pregnancy and post-partum and high oestradiol levels during clomiphene stimulation for infertility) on QT duration in human subjects and assess oestradiol effects on IKr and KCNH2/ HERG channel trafficking in vitro in human embryonic kidney (HEK) cells. Unexpectedly, and in contrast to our current knowledge, they identify a QT shortening with increasing oestradiol levels along with increased KCNH2/HERG channel trafficking to the membrane and increased IKr current densities. Even more intriguingly, no such effect on QT duration is seen with increasing progesterone levels, although the data of patients during pregnancy suggest a negative correlation between progesterone levels and QT duration. Here, further studies in larger patient cohorts are clearly warranted. This study, and its pronounced differences compared with previous studies in animal models, demonstrates the importance of investigating mechanisms of sex hormone effects on repolarization in human subjects and human tissue/cells to solve the complex riddle of hormonal regulation of cardiac repolarization and arrhythmogenic risk. In the future, novel techniques such as induced pluripotent stem cell – derived cardiomyocytes might further help us to reveal sex hormone effects in a ‘cardiomyocyte-like’ environment rather than in heterologous expression systems. The clinically observed distinct sex differences in cardiac repolarization and known sex hormone effects on various repolarizing ion The opinions expressed in this article are not necessarily those of the Editors of the European Heart Journal or of the European Society of Cardiology. † doi:10.1093/eurheartj/ehv371. * Corresponding author. Heart Center University of Freiburg, Department of Cardiology and Angiology I, Hugstetter Str. 55, 79106 Freiburg, Germany. Tel: +49 761 270 32470, Fax: +49 761 270 73090, Email: [email protected] Published on behalf of the European Society of Cardiology. All rights reserved. & The Author 2015. For permissions please email: [email protected]. 652 Editorial Figure 1 Oestradiol effects on cardiac ion channels/currents and action potential duration. Illustration of oestradiol effects on KCNH2/HERG (IKr) and Cav1.2a channels (ICa,L) that are mediated either via oestradiol receptors or in a receptor-independent manner (information based on1,6,12,13). Consecutive changes in action potential duration (APD) are depicted in insets. E2, oestradiol; E2 receptor, oestradiol receptor a; HRE, hormone responsive element; Hsp90, heat-shock protein 90; ICa,L, L-type Ca2+ current; IK1, inward rectifier current; IKr, rapid delayed rectifier K+ current; IKs, slow delayed rectifier K+ current; INa, depolarizing Na+ current; Ito, transient outward K+ current; +, increase; –, decrease/ blockade; , prolongation of APD; , shortening of APD. channels/currents suggest that, in the future, sex hormone – based drugs might be utilized as novel anti-arrhythmic therapies. The authors also state that the observed oestradiol-induced QT shortening could potentially be exploited as a therapeutic approach in LQTS. However, this suggestion should be considered very cautiously and might even be premature since oestradiol also exerts a contrasting pronounced pro-arrhythmic effect, increasing the incidence of ventricular arrhythmia and sudden cardiac death in transgenic LQT2 rabbits due to increased ICa,L currents and early afterdepolarization formation.12 Before we better understand this complex interaction and species-dependent variations, it might be too early to exploit hormonal treatment as an anti-arrhythmic therapeutic option. Moreover, in general, it will be challenging to establish future sex hormone–based anti-arrhythmic therapies due to potential systemic side effects via steroid receptors expressed in other organs and since different synthetic hormone derivatives may have unspecific actions via other sex hormone receptors. Several cases and clinical studies have demonstrated that in contrast to pure progesterone,12 synthetic progesterone derivatives that have additional partial oestradiolmimicking effects lack any anti-arrhythmic effects14 and that combined oestradiol–gestagene treatment as it is used for contraception lacks effects on cardiac repolarization and arrhythmogenic risk.15 Overall, the complex hormonal impact on all major repolarizing ion channels/currents and Ca2+ handling proteins, and their partly contrasting and thus (simultaneously) pro- and anti-arrhythmic effects, clearly warrant further detailed investigation. This article adds an interesting, yet only partially fitting, piece to the puzzle. However, if we listen to Isaac Asimov, who said ‘The most exciting phrase to hear in science . . . is not ‘Eureka!’ but ‘That’s funny . . . ,’ ” exciting times are ahead. Acknowledgements Special thanks to Dr Michael Brunner for his valuable comments regarding this editorial. Conflict of interest: The author declares no conflict of interest. Editorial References 1. Anneken L, Baumann S, Vigneault P, Biliczki P, Friedrich C, Xiao L, Girmatsion Z, Takac I, Brandes RP, Kissler S, Wiegratz I, Zumhagen S, Stallmeyer B, Hohnloser SH, Klingenheben T, Schulze-Bahr E, Nattel S, Ehrlich JR. Estradiol regulates human QT-interval: acceleration of cardiac repolarization by enhanced KCNH2 membrane trafficking. Eur Heart J 2016;37:640 –650. 2. Sauer AJ, Moss AJ, McNitt S, Peterson DR, Zareba W, Robinson JL, Qi M, Goldenberg I, Hobbs JB, Ackerman MJ, Benhorin J, Hall WJ, Kaufman ES, Locati EH, Napolitano C, Priori SG, Schwartz PJ, Towbin JA, Vincent GM, Zhang L. Long QT syndrome in adults. J Am Coll Cardiol 2007;49:329 –337. 3. Rodriguez I, Kilborn MJ, Liu XK, Pezzullo JC, Woosley RL. Drug-induced QT prolongation in women during the menstrual cycle. JAMA 2001;285:1322 –1326. 4. Seth R, Moss AJ, McNitt S, Zareba W, Andrews ML, Qi M, Robinson JL, Goldenberg I, Ackerman MJ, Benhorin J, Kaufman ES, Locati EH, Napolitano C, Priori SG, Schwartz PJ, Towbin JA, Vincent GM, Zhang L. Long QT syndrome and pregnancy. J Am Coll Cardiol 2007;49:1092 –1098. 5. Odening KE, Koren G. How do sex hormones modify arrhythmogenesis in long QT syndrome? Sex hormone effects on arrhythmogenic substrate and triggered activity. Heart Rhythm 2014;11:2107 – 2115. 6. Kurokawa J, Tamagawa M, Harada N, Honda S, Bai CX, Nakaya H, Furukawa T. Acute effects of oestradiol on the guinea pig and human IKr channels and drug-induced prolongation of cardiac repolarization. J Physiol 2008;586:2961–2973. 7. Er F, Michels G, Brandt MC, Khan I, Haase H, Eicks M, Lindner M, Hoppe UC. Impact of testosterone on cardiac L-type calcium channels and Ca2+ sparks: acute actions antagonize chronic effects. Cell Calcium 2007;41:467 –477. 653 8. Liu XK, Katchman A, Drici MD, Ebert SN, Ducic I, Morad M, Woosley RL. Gender difference in the cycle length-dependent QT and potassium currents in rabbits. J Pharmacol Exp Ther 1998;285:672–679. 9. Gaborit N, Varro A, Le Boutier S, Szuts V, Escande D, Nattel S, Demolombe S. Gender-related differences in ion-channel and transporter subunit expression in non-diseased human hearts. J Mol Cell Cardiol 2010;49:639 – 646. 10. Furukawa T, Kurokawa J. Non-genomic regulation of cardiac ion channels by sex hormones. Cardiovasc Hematol Disord Drug Targets 2008;8:245 –251. 11. Furukawa T, Kurokawa J, Clancy CE. A combined approach using patch-clamp study and computer simulation study for understanding long QT syndrome and TdP in women. Curr Cardiol Rev 2008;4:244 –250. 12. Odening KE, Choi BR, Liu GX, Hartmann K, Ziv O, Chaves L, Schofield L, Centracchio J, Zehender M, Peng X, Brunner M, Koren G. Estradiol promotes sudden cardiac death in transgenic long-QT type 2 rabbits while progesterone is protective. Heart Rhythm 2012;9:823 –832. 13. Yang X, Chen G, Papp R, Defranco DB, Zeng F, Salama G. Oestrogen upregulates L-type Ca2+ channels via oestrogen-receptor-a by a regional genomic mechanism in female rabbit hearts. J Physiol 2012;590:493 – 508. 14. Giudicessi JR, Brost BC, Traynor KD, Ackerman MJ. Potential depot medroxyprogesterone acetate-triggered torsades de pointes in a case of congenital type 2 long QT syndrome. Heart Rhythm 2012;9:1143 –1147. 15. Abu-Zeitone A, Peterson DR, Polonsky B, McNitt S, Moss AJ. Oral contraceptive use and the risk of cardiac events in patients with long QT syndrome. Heart Rhythm 2014;11:1170 – 1175.