Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Remote ischemic conditioning wikipedia , lookup
Electrocardiography wikipedia , lookup
Coronary artery disease wikipedia , lookup
Heart failure wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Antihypertensive drug wikipedia , lookup
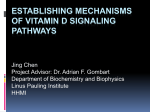
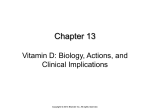
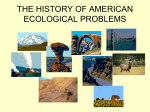
J Appl Physiol 114: 979–987, 2013. First published February 21, 2013; doi:10.1152/japplphysiol.01506.2012. Vitamin D signaling pathway plays an important role in the development of heart failure after myocardial infarction Soochan Bae,1 Sylvia S. Singh,1 Hyeon Yu,1,2 Ji Yoo Lee,1 Byung Ryul Cho,1,3 and Peter M. Kang1,2 1 Cardiovascular Division, Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, Massachusetts; Department of BIN Fusion Technology, Chonbuk National University, Jeonju; 3Division of Cardiology, Kangwon National University, Chuncheon, South Korea 2 Submitted 17 December 2012; accepted in final form 17 February 2013 heart failure; myocardial infarction; vitamin D; apoptosis; inflammation CARDIOVASCULAR DISEASE is the leading cause of morbidity and mortality in developed countries. Coronary heart disease, particularly myocardial infarction (MI) and heart failure, affects 7.9 million and 5.7 million US adults, respectively (39). Occurrence of left ventricular abnormalities related to remodeling (predominantly progressive chamber dilation, fibrosis, and systolic/diastolic dysfunction) and heart failure often complicates MI (1). Recent data suggest that the prevalent myocardial dysfunctions and heart failure are associated with decreased levels of vitamin D (21, 23, 28). However, the role of vitamin D signaling in the development of heart failure is not well characterized. Vitamin D plays an important physiological role in controlling cardiac functions, and vitamin D-dependent signaling systems are present in cardiac myocytes and fibroblasts (9). Vitamin D deficiency has been shown to lead to derangements in cardiac myocyte contraction, abnormal cardiac relaxation, Address for reprint requests and other correspondence: P. M. Kang, Cardiovascular Division, Beth Israel Deaconess Medical Center, 3 Blackfan Circle, CLS 910, Boston, MA 02215 (e-mail: [email protected]). http://www.jappl.org proliferation, protein expression, and increased cardiac renin gene expression (5, 35, 36, 44, 47). Previously, we have demonstrated that vitamin D therapy prevents the progression to cardiac hypertrophy (6) and attenuates the development of heart failure in a salt-sensitive rat model (4). Numerous investigators have also showed that vitamin D therapy is renoprotective in various experimental nephropathy models via its anti-inflammatory and antifibrotic actions (2, 32, 42, 43). Because the prevalence of vitamin D deficiency has been shown to be common and treatable (27), it is imperative to better understand the mechanism of vitamin D signaling in heart, which may potentially precede to novel therapeutic strategies in cardiovascular diseases. However, the cardioprotective mechanisms that are involved are not well understood, and our understanding of the role of vitamin D in the maintenance of cardiac function remains unclear (15). In this study, we examine the role of vitamin D signaling in preventing heart failure after MI with the activation or inhibition of vitamin D signaling using paricalcitol (PC) and vitamin D receptor (VDR) knockout (KO) mice, respectively. We hypothesize that vitamin D therapy may attenuate the progression of heart failure after MI through anti-inflammatory, antifibrotic, and antiapoptotic mechanisms. MATERIALS AND METHODS Materials. Materials and antibodies were obtained from flowing sources as follows: PC (provided by Abbott Laboratories, Abbott Park, IL), VDR antibody (sc-1008) (Santa Cruz Biotechnology, Santa Cruz, CA), and GAPDH antibody (Cell Signaling Technology, Danvers, MA). Adult cardiomyocyte culture and apoptotic stimulation. Primary cultures of cardiomyocytes from 6-wk-old Sprague-Dawley rats were prepared as described (14, 22). Twenty-four hours after PC pretreatment (20 M), cardiomyocytes were exposed to hydrogen peroxide (H2O2) at 0.1 mM for 24 h to induce apoptosis. Animal surgery and treatment. Male VDR KO mice (Jackson Laboratory, Bar Harbor, ME) and their littermates in a C57BL/6 background were used as a model for defective vitamin D signaling. To activate vitamin D signaling, 10 –12-wk-old male mice were administered with PC or vehicle (Veh) 1 wk before MI and continued until the end of the experiment. Wild-type (WT) mice underwent sham or MI operation with either Veh treatment or PC therapy (15 ng/mouse, i.p., 3 times per week). Coronary artery ligation was performed as described previously (46). After anesthesia with isofluorane (initially 4 –5% in an induction chamber then 2% via intubation tube) via a precise vaporizer inhaler, each mouse was intubated, and the heart was exposed and the left anterior descending (LAD) artery ligated proximally with a 7– 0 silk suture. We confirmed the occlusion by the pallor of the anterior left ventricular wall. All groups of mice were age- and sex-matched littermates. For sham operations, the mice underwent the same procedure except for LAD ligation. Euthanasia 8750-7587/13 Copyright © 2013 the American Physiological Society 979 Downloaded from http://jap.physiology.org/ by 10.220.32.247 on June 15, 2017 Bae S, Singh SS, Yu H, Lee JY, Cho BR, Kang PM. Vitamin D signaling pathway plays an important role in the development of heart failure after myocardial infarction. J Appl Physiol 114: 979–987, 2013. First published February 21, 2013; doi:10.1152/japplphysiol.01506.2012.—Accumulating evidence suggests that vitamin D deficiency plays a crucial role in heart failure. However, whether vitamin D signaling itself plays an important role in cardioprotection is poorly understood. In this study, we examined the mechanism of modulating vitamin D signaling on progression to heart failure after myocardial infarction (MI) in mice. Vitamin D signaling was activated by administration of paricalcitol (PC), an activated vitamin D analog. Wild-type (WT) mice underwent sham or MI surgery and then were treated with either vehicle or PC. Compared with vehicle group, PC attenuated development of heart failure after MI associated with decreases in biomarkers, apoptosis, inflammation, and fibrosis. There was also improvement of cardiac function with PC treatment after MI. Furthermore, vitamin D receptor (VDR) mRNA and protein levels were restored by PC treatment. Next, to explore whether defective vitamin D signaling exhibited deleterious responses after MI, WT and VDR knockout (KO) mice underwent sham or MI surgery and were analyzed 4 wk after MI. VDR KO mice displayed a significant decline in survival rate and cardiac function compared with WT mice after MI. VDR KO mice also demonstrated a significant increase in heart failure biomarkers, apoptosis, inflammation, and fibrosis. Vitamin D signaling promotes cardioprotection after MI through anti-inflammatory, antifibrotic and antiapoptotic mechanisms. Vitamin D Signaling Pathway After Myocardial Infarction H2O2 * 2.0 † 1.5 1.0 0.5 0.0 Veh PC Veh E Sham 2.5 * 2.0 1.5 † 1.0 0.5 0.0 PC Veh Sham H2O2 Veh PC Veh Sham Sham MI ANF BNP 18S MI D Sham MI 10 8 * † 6 4 2 * 8 † 6 4 2 0 0 Veh F PC MI PC C Fold of Veh-Sham 2.5 B PARP-1 Activity (Fold of Veh-Sham) Caspase-3 Activity (Fold of Veh-Sham) Sham PC Veh Veh-Sham Veh-MI 2.5 2.0 PC PC-Sham PC-MI * * † † 1.5 1.0 0.5 0.0 ANF G Sham MI MI H Veh 50 Infarct Size (%) PC BNP * 40 Sham MI 30 *† 20 10 0 Veh PC Fig. 1. Effect of paricalcitol (PC) therapy after myocardial infarction (MI) in vitro and in vivo. A–B: effect of PC on Caspase-3 activity (A) and poly(ADP-ribose) polymerase (PARP)-1 activity (B) after H2O2 (0.1 mM) in adult cardiomyocytes. [N ⫽ 4/group; *P ⬍ 0.05 vs. vehicle (Veh), †P ⬍ 0.05 vs. Veh-H2O2]. C–D: heart weight over body weight (HW/BW) ratio (C), and lung weight over body weight (LUW/BW) ratio (D) in sham and MI groups with or without PC. (N ⫽ 4 – 6 mice in each group; *P ⬍ 0.05 vs. sham of each group, †P ⬍ 0.05 vs. Veh-MI). E: representative image of heart failure markers, atrial natriuretic factor (ANF) and brain natriuretic peptide (BNP) in sham and MI groups with or without PC. F: quantitative analysis of heart failure markers, ANF and BNP. (N ⫽ 4 – 6 mice in each group; *P ⬍ 0.05 vs. sham of each group, †P ⬍ 0.05 vs. Veh-MI). G: representative photomicrographs from histological sections stained with Masson’s Trichrome. H: infarct size analysis of sham and MI with and without PC. J Appl Physiol • doi:10.1152/japplphysiol.01506.2012 • www.jappl.org Downloaded from http://jap.physiology.org/ by 10.220.32.247 on June 15, 2017 A Bae S et al. Terminal deoxynucleotidyl transferase dUTP nick-end labeling (TUNEL) staining was performed using in situ fluorescein-based Cell Death Detection Kits (Roche Applied Science, Indianapolis, IN) as described previously (3). Quantitative analysis of apoptotic nuclei were performed in border zones of infarcted hearts. To distinguish cardiomyocyte from noncardiomyocyte nuclei, we triple stained for nuclei [4=,6-diamidino-2-phenylindole (DAPI) staining], apoptotic nuclei (TUNEL staining), and cardiomyocytes (␣-actinin staining) and analyzed the stained sections using confocal microscopy. A minimum of 200 nuclei/field were counted for each sample. RT-PCR for mRNA expression. Heart tissues were collected just below the level of papillary muscles and processed for molecular analysis 4 wk after MI. Semiquantitative RT-PCR was performed as described previously (4). The mRNA expression levels were analyzed by RT-PCR by specific primers (see Supplemental Methods; supplemental material for this article is available online at the Journal of Applied Physiology website). Ribosomal 18S primers acted as internal controls, and all RT-PCR signals were normalized to the 18S expression. HW/BW (mg/g) was performed by CO2 via a gas cylinder followed by heart extraction. All procedures were approved by and performed in accordance with Beth Israel Deaconess Medical Center Institutional Animal Care and Use Committee guidelines. Cardiac function analysis. Cardiac function was evaluated by measuring the left ventricular (LV) pressure-volume (PV) loop to calculate hemodynamic parameters, including cardiac output (CO), stroke work (SW), stroke volume (SV), and isovolumetric relaxation as described previously (3, 13). Apoptosis assays. The activities of caspase-3 and poly(ADP-ribose) polymerase (PARP)-1 were determined with colorimetric assay kit (R&D Systems, Minneapolis, MN) as described previously (3, 13). Briefly, for caspase-3 activity assay, protein samples were added to substrates of Acetyl-Asp-Glu-Val-Asp-p-nitroanilide, and enzymecatalyzed release of p-nitroanilide was then measured at 405 nm. For PARP activity assay, activity was measured at 450 nm by incorporation of biotinylated poly (ADP-ribose) onto histone-coated proteins in the plate using colorimetric assay kit. • LUW/BW (mg/g) 980 Vitamin D Signaling Pathway After Myocardial Infarction Immunoblot. Immunoblot analyses were also performed as described previously (4). Total protein of VDR from heart tissue was probed with an anti-VDR rabbit polyclonal antibody. GAPDH was used as an internal control. Resulting bands were quantified as optical density (OD) ⫻ band area by NIH ImageJ software (version 1.38⫻; NIH, Bethesda, MD). Histology. Hearts were fixed in 10% formalin and paraffin embedded. Sections were stained with Masson-Trichrome at the Histology Core facility at BIDMC. Infarct size was calculated as described previously (25). Briefly, the infarct length was calculated by measuring the endo- and epicardial surface length delimiting the infarcted region. Infarct size percentage was calculated as infarct length divided by the total LV circumference using ImageJ software. Statistical analysis. Data were expressed as means ⫾ SE. Comparisons between and within groups were conducted with unpaired Student’s t-tests and repeated-measures ANOVA using GraphPad Prism 5.0 (San Diego, CA), respectively. Survival curves after MI were created by the Kaplan-Meier method and compared by a log rank test. P values of ⬍0.05 were considered significant. PC therapy attenuates the development of heart failure after myocardial infarction. We initially determined whether PC treatment exerts a protective effect against H2O2-induced apoptotic A Sham MI Sham MI COL 1A1 COL 3A1 18S 2 MI Sham MI TNF-α MCP-1 18S PC-Sham PC-MI * * 1.5 Fig. 2. Effect of PC on mRNA expression of biochemical markers of fibrosis, inflammation, and renin-angiotensin system (RAS) after MI. A: representative mRNA expression of collagenase (COL) 1A1 and 3A1. B: quantitative analysis of mRNA expression of collagenase 1A1 and 3A1. (N ⫽ 4 – 6 mice in each group; *P ⬍ 0.05 vs. sham of each group, †P ⬍ 0.05 vs. Veh-MI). C: representative image of inflammatory markers, tumor necrosis factor-␣ (TNF-␣) and monocyte chemoattractant protein-1 (MCP-1) in sham and MI groups with or without PC. D: quantitative analysis of inflammatory markers, TNF-␣ and MCP-1. (N ⫽ 4 – 6 mice in each group; *P ⬍ 0.05 vs. sham of each group, †P ⬍ 0.05 vs. Veh-MI) E: representative image of RAS genes [angiotensinogen (ANGTSN), renin, and renin receptor (ReninR)] in sham and MI groups with or without PC. F: quantitative analysis of RAS genes (N ⫽ 4 – 6 mice in each group; *P ⬍ 0.05 vs. sham of each group, †P ⬍ 0.05 vs. Veh-MI). COL3A1 Veh-Sham Veh-MI 2.0 Fold of Veh-Sham Sham PC † COL 1A1 D Veh * † 1 0 C PC-Sham PC-MI * 3 PC Fold of Veh-Sham Veh † † 1.0 0.5 0.0 TNF-α E F ANGTSN ReninR Renin 18S MI PC Sham MCP-1 Veh-Sham Veh-MI 2.0 MI Fold of Veh-Sham Veh Sham 981 cell death in rat adult cardiomyocytes and whether such protection is associated with decreased activation of caspase-3 and PARP-1 activities. H2O2 significantly increased activation of caspase-3 and PARP-1 compared with vehicle control (Fig. 1, A and B). However, PC treatment significantly attenuated activation of caspase-3 and PARP-1. These data suggest that PC protected adult cardiomyocytes against H2O2-induced apoptosis. Then, to study the effect of activating vitamin D signaling in cardiac apoptosis in vivo, we examined the mice assigned to four groups: 1) Veh ⫹ Sham, 2) Veh ⫹ MI, 3) PC ⫹ Sham, and 4) PC ⫹ MI. Mice underwent sham or MI operation with either Veh treatment or PC therapy (15 ng/mouse, i.p. 3 times per week) before MI. We found that PC treatment resulted in significant decrease in heart weight (HW)/body weight (BW) ratio (P ⬍ 0.05) and lung weight (LuW)/BW ratio (P ⬍ 0.05) in PC ⫹ MI group compared with the Veh ⫹ MI group (Fig. 1, C and D). No significant differences were observed in the sham-operated mice treated with PC or Veh. We next sought to determine whether the pathophysiological findings correlated with other biological and molecular measures. The analyses of mRNA expression levels of atrial natriuretic factor (ANF) and brain natriuretic peptide (BNP) of Veh-Sham Veh-MI B Bae S et al. * PC-Sham PC-MI * * 1.5 † † † 1.0 0.5 0.0 ANGTSN ReninR Renin J Appl Physiol • doi:10.1152/japplphysiol.01506.2012 • www.jappl.org Downloaded from http://jap.physiology.org/ by 10.220.32.247 on June 15, 2017 RESULTS • Vitamin D Signaling Pathway After Myocardial Infarction A Sham MI D Sham C MI Sham 2.0 MI Sham * 1.0 † 0.5 0.0 8 6 *† 4 * 2 0 Veh PC Sham MI Veh F 20 900 600 * 300 *† 10 * 5 TAU (ms) *† SV (µL) 15 0 0 Veh PC PC Sham 30 MI * 1500 1200 MI 10 1.5 E 1800 SW (mmHg*µL) Activation of circulating and tissue RAS leads to ventricular remodeling after MI, a process that is associated with altering myocardial apoptosis, myocardial hypertrophy, and increasing the content of collagen (33). There were significant increases in mRNA expression of components of the RAS gene 4 wk after MI (Fig. 2, E and F). The mRNA expressions of angiotensinogen, renin, and renin receptors were significantly reduced by PC treatment compared with Veh-treated mice after MI. Effect of PC on apoptosis and cardiac function after MI. Because adverse LV remodeling after MI has been associated with increased apoptosis in the myocardium (37), we examined the effects of PC on cardiomyocyte apoptosis. The number of TUNEL-positive myocytes in the ischemia border zone were significantly greater in animals subjected to MI (Veh ⫹ MI) than in sham-operated animals (Fig. 3, A and B), suggesting that apoptosis is enhanced during cardiac remodeling. Conversely, the number of TUNEL-positive myocytes in ischemia border zone was significantly lower in PC ⫹ MI than in Veh ⫹ MI groups (0.39% vs. 1.64%, P ⬍ 0.05). These data confirmed our notion that PC therapy inhibits apoptosis. Finally, cardiac function was evaluated by measuring the LV PV loop 4 wk after MI. PV loop analysis revealed that PC after MI resulted in a significant improvement of CO, SW, and SV and a significant reduction in isovolumetric relaxation () compared with the vehicle group after MI (Fig. 3, C–F). Effect of PC on VDR expression after MI. Key components of vitamin D-dependent signaling system are present in the B PC TUNEL + Cardiomyocyte (%) Veh Bae S et al. *† 20 10 0 Veh PC Veh PC Fig. 3. Effect of PC on apoptosis and cardiac function after MI. A: representative terminal deoxynucleotidyl transferase dUTP nick-end labeling (TUNEL) staining of cardiomyocytes in sham and MI groups with or without PC. B: quantification of TUNEL-positive cardiomyocytes/total cells. (N ⫽ 4 – 6 mice in each group; *P ⬍ 0.05 vs. sham of each group, †P ⬍ 0.05 vs. Veh-MI). C–F: hemodynamic measurements by pressure-volume (PV) loop after MI, cardiac output (CO), stroke work (SW), stroke volume (SV), and tau () in sham and MI groups with or without PC. (N ⫽ 4 – 6 mice in each group; *P ⬍ 0.05 vs. sham of each group, †P ⬍ 0.05 vs. Veh-MI). J Appl Physiol • doi:10.1152/japplphysiol.01506.2012 • www.jappl.org Downloaded from http://jap.physiology.org/ by 10.220.32.247 on June 15, 2017 the LV tissues showed that PC significantly attenuated ANF (⫺33%) and BNP (⫺29%), which were both increased after MI (P ⬍ 0.05 for all) (Fig. 1, E and F). We also found that the infarct size after MI is significantly decreased in PC ⫹ MI group than in Veh ⫹ MI group (16.8 ⫾ 4.3 vs. 42 ⫾ 6.0) (Fig. 1, G and H). There were no significant differences observed between the two sham groups. Effect of PC on fibrosis and inflammation after MI. To examine the potential vitamin D signaling-induced cardioprotective mechanisms after MI, we examined the effect of PC on fibrosis, inflammation, and renin-angiotensin system (RAS). Because studies have shown that vitamin D therapy has an antifibrotic effect (4, 29, 32, 41), the degree of fibrosis was quantified by examining the expression of collagen 1A1 and 3A1, the main forms of collagen in the heart. PC effectively reduced Col1A1 and Col3A1 mRNA levels in the infarct zone compared with the Veh ⫹ MI group (Fig. 2, A and B), suggesting that PC treatment attenuates increased fibrosis 4 wk after MI. Inflammation is known to play an important role in the development and progression to heart failure (34). To establish whether PC suppresses inflammation in the heart, we examined mRNA level of tissue necrosis factor-␣ (TNF-␣) and monocyte chemoattractant protein (MCP)-1. TNF-␣ and MCP-1 mRNA levels were significantly elevated in Veh ⫹ MI than in shamoperated animals (Fig. 2, C and D). These increases were significantly reduced by PC treatment (P ⬍ 0.05 for both). • CO (ml/min) 982 Vitamin D Signaling Pathway After Myocardial Infarction A B Effect of defective vitamin D signaling on apoptosis, cardiac function, and survival rate after MI. Because our PC study exhibited elevated VDR expression in cardiomyocytes and inhibition of apoptosis after MI, we next investigated the effects of defective vitamin D signaling on apoptosis. TUNELpositive cardiomyocytes exhibited higher levels of apoptosis in VDR KO mice compared with WT mice 2 days after MI (4.25% vs. 1.55%, P ⬍ 0.05) (Fig. 6, A and B), thereby confirming that deletion of VDR does indeed display significant apoptotic effects in the myocardium after MI. PV loop analysis after MI also demonstrated that cardiac function parameters were significantly worsened in VDR KO ⫹ MI mice than in WT ⫹ MI group. VDR KO ⫹ MI group displayed a significant reduction in the CO, SW, and SV and a significant increase in isovolumetric relaxation () in VDR KO mice compared with the WT ⫹ MI mice (Fig. 6, C–F). Finally, we explored whether mice lacking VDR or defective vitamin D signaling may exhibit significant mortality 4 wk after MI. We compared survival rates after MI surgery among WT ⫹ sham, VDR KO ⫹ sham, WT ⫹ MI, and VDR KO ⫹ MI mice. The survival rate was found to be significantly lower in VDR KO ⫹ MI mice than in WT ⫹ MI mice at 4 wk (77% vs. 54%, P ⬍ 0.05) (Fig. 6G). All the deaths occurred early within a week with a 45% decline in VDR-KO mice and 20% decline in WT-MI mice after MI. These results indicate that VDR deficiency may cause fulminant and aggressive heart failure after MI. DISCUSSION The key findings of the present study are that 1) the activation of VDR pathway by PC may offer cardioprotection as it attenuates cardiac dysfunction, cardiac myocyte apoptosis, and upregulation of proinflammatory cytokines in mouse models and 2) deficiency of VDR causes fulminant and aggressive Sham MI Sham MI VDR 18S VDR mRNA (Fold of WT Sham) Sham PC MI ** 1.5 Veh † 1.0 * 0.5 0.0 Veh C D Sham VDR GAPDH MI Sham PC MI MI Sham 2.0 PC VDR Protein (Fold of WT Sham) Veh 983 ** † 1.5 1.0 Fig. 4. Effect of PC on mRNA and protein expression of vitamin D receptor(VDR) after MI. A: representative image of tissue mRNA level of VDR in sham and MI groups with or without PC. B: quantitative analysis of tissue mRNA level of VDR. (N ⫽ 4 – 6 mice in each group; *P ⬍ 0.05 vs. sham of each group, **P ⬍ 0.05 vs. Veh-sham, †P ⬍ 0.05 vs. Veh-MI). C: representative image of tissue protein level of VDR in sham and MI groups with or without PC. D: quantitative analysis of tissue protein level of VDR. (N ⫽ 4 – 6 mice in each group; *P ⬍ 0.05 vs. sham of each group, **P ⬍ 0.05 vs. Veh-Sham, †P ⬍ 0.05 vs. Veh-MI). WT, wild-type. * 0.5 0.0 Veh PC J Appl Physiol • doi:10.1152/japplphysiol.01506.2012 • www.jappl.org Downloaded from http://jap.physiology.org/ by 10.220.32.247 on June 15, 2017 heart (9), and the loss of VDR expression may increase the likelihood of heart failure progression. Thus we investigated mRNA and protein levels of VDR after MI. We confirmed that, 4 wk after MI, mRNA and protein expression of VDR were notably reduced in Veh ⫹ MI group when compared with sham controls (Fig. 4, A–D). Consistent with other findings in the kidneys (42), PC amplifies VDR expression in both mRNA and protein expression in cardiac myocytes after MI. In addition, the significant reduction of VDR mRNA and protein levels by MI was abrogated by PC treatment. Together, we conclude that VDR activation by PC may play a cardioprotective role in the progression to heart failure caused by MI. Effect of defective vitamin D signaling on heart failure after MI. The consequences of VDR disruption on cardiac myocytes were then examined as we compared the VDR KO mice and their WT controls. VDR KO mice did not express any VDR expression in the heart (Fig. 5A). Morphology data showed that, after MI, the HW/BW ratio and the LuW/BW ratio were significantly higher in VDR KO mice than in WT group (Fig. 5, B and C). Although there was a modest increase at baseline in WT sham group, MI caused a much more significant increase, not only in absolute percentage changes, in HW/BW ratio and LuW/BW ratio of VDR KO sham mice. Thus these findings suggest that VDR KO mice developed a more severe progression to heart failure at 4 wk after MI than WT mice. We also observed an upregulation in mRNA levels of ANF and BNP gene expression in VDR KO mice compared with WT mice after MI (P ⬍ 0.05 for all) (Fig. 5, D and E). In addition, inflammatory markers TNF-␣ and MCP-1 mRNA levels were significantly higher in VDR KO-MI groups than in the WT-MI group (Fig. 5, F and G). VDR KO at baseline did not show increases in biochemical and inflammatory markers for heart failure. Bae S et al. • 984 Vitamin D Signaling Pathway After Myocardial Infarction B Sham HW/BW (mg/g) WT VDR KO VDR GAPDH C MI 10 * 6 4 2 0 MI Sham MI BNP 18s * 4 2 2.0 WT *† * * Sham VDR KO MI Sham MI Fold of WT Sham G WT 18S WT-MI VDRKO-MI 1.0 0.5 0.0 F MCP-1 WT-Sham VDRKO-Sham 1.5 ANF TNF-α VDR KO 3 2 BNP *† *† * * WT-Sham WT-MI VDRKO-Sham VDRKO-MI 1 0 TNF-α MCP-1 Fig. 5. Effect of defective vitamin D signaling on heart failure after MI. A: VDR protein expression in WT and VDR knockout (KO) mice heart. B–C: HW/BW ratio (B) and LUW/BW ratio (C) in sham and MI groups. (N ⫽ 4 – 6 mice in each group; *P ⬍ 0.05 vs. sham of each group, †P ⬍ 0.05 vs. WT-MI). D: representative image of tissue mRNA level of ANF and BNP in sham and MI groups. E: quantitative analysis of tissue mRNA level of ANF and BNP. (N ⫽ 4 – 6 mice in each group; *P ⬍ 0.05 vs. sham of each group, †P ⬍ 0.05 vs. WT-MI). F: representative image of tissue mRNA level of TNF-␣ and MCP-1 in sham and MI groups. G: quantitative analysis of tissue mRNA level of TNF-␣ and MCP-1. (N ⫽ 4 – 6 mice in each group; *P ⬍ 0.05 vs. sham of each group, †P ⬍ 0.05 vs. WT-MI). progression of heart failure after MI because they lack cardioprotective signaling through the VDR pathway. These findings demonstrate that vitamin D therapy could be an effective, preventive, and therapeutic candidate against progression of heart failure after MI. Vitamin D and its biological activities are mediated by a specific high-affinity receptor, the VDR, a member of the superfamily of nuclear receptors for steroid hormones (16). Analogous to other members of the steroid family, VDR acts as a ligand-activated transcription factor, and, upon activation by its ligand, VDR forms a heterodimeric complex with its obligatory partner, retinoid X receptor, and binds to the vitamin D response element. Hence, loss of VDR could lead to an eradication of vitamin D signaling, even without any reduction in levels of active vitamin D (42). Several cardioprotective mechanisms of vitamin D signaling could be postulated from our study. Earlier studies have stated that there may be a direct connection between vitamin D and apoptosis (31, 42) although this connection had not been shown in cardiomyocytes. A study using an obstructive nephropathy rat model, consistent with our findings, demonstrated that vitamin D treatment upregulated VDR levels in vehicle rats and significantly decreased the number of TUNEL-positive cells in obstructed animals (20). Additionally, pretreatment with 1,25(OH)2D3 (calcitriol) increases VDR gene expression in cardiomyocyte but has no effect in cardiac fibroblasts (10). Collectively, these results suggest that upregulation/activation of liganded VDR signaling may protect cardiomyocyte against MI-induced apoptosis. Therefore, beneficial effects of PC may be linked to attenuation of cardiac dysfunction after MI. The results from our study, to our knowledge, are the first to suggest that vitamin D therapy could be a possible approach to the reduction of apoptosis in cardiomyocytes in MI-induced heart failure. We showed that vitamin D therapy significantly decreased cardiac fibrosis and extracellular matrix remodeling, a pathological feature of heart failure, after MI. Tan et al. (42) J Appl Physiol • doi:10.1152/japplphysiol.01506.2012 • www.jappl.org Downloaded from http://jap.physiology.org/ by 10.220.32.247 on June 15, 2017 ANF Fold of WT Sham Sham † 6 *† 2.5 VDR KO * 8 VDR KO E WT MI 0 WT D Sham 10 † * 8 Bae S et al. LUW/BW (mg/g) A • Vitamin D Signaling Pathway After Myocardial Infarction A WT • 985 Bae S et al. B VDR KO TUNEL + Cardiomyocyte (%) Sham Sham MI MI 5 * 4 3 * 2 1 0 WT *† 2 1500 * 1000 † * 500 WT * † 0 VDR KO WT F * 10 5 0 0 MI 15 SV (µL) SW (mmHg*µL) * 4 20 MI 8 6 Sham Sham 2000 MI CO (ml/min) E D Sham 10 VDR KO G VDR KO WT 100 VDR KO WT-Sham Sham 80 WT-MI Survival (%) * 20 TAU (ms) VDR KO-Sham MI 25 * 15 10 5 VDR KO-MI 60 * † 40 20 0 WT VDR KO 0 0 4 8 12 16 20 24 28 Time after MI (d) Fig. 6. Effect of defective vitamin D signaling on apoptosis, cardiac function, and survival rates after MI. A: representative TUNEL staining of cardiomyocytes in sham and MI groups. B: quantification of TUNEL-positive cardiomyocytes/total cells. (N ⫽ 4 – 6 mice in each group; *P ⬍ 0.05 vs. sham of each group, †P ⬍ 0.05 vs. WT MI). C–F: hemodynamic measurements by PV loop in sham and MI groups. (N ⫽ 4 – 6 mice in each group; *P ⬍ 0.05 vs. sham of each group, †P ⬍ 0.05 vs. WT MI). G: survival rates after MI in WT and VDR KO mice. Survival curves up to 4 wk after MI were created by Kaplan-Meier method and compared by a log-rank test. (N ⫽ 10 –15 mice in each group; *P ⬍ 0.05 vs. sham of each group, †P ⬍ 0.05 vs. WT-MI). observed that dramatic downregulation of VDR in the fibrotic kidney was completely restored by administration of vitamin D, resulting in an increase in VDR expression and further suggesting that deficiency in vitamin D signaling in the diseased kidney is far greater than it was anticipated earlier. Mizobuchi et al. (32) also showed that vitamin D therapy suppresses the progression of perivascular fibrosis and myocardial arterial vessel thickness and inhibits collagen synthesis after MI in vivo, presumably due to the upregulation/activation of VDR signaling. These findings coincide with our data where vitamin D demonstrates a significant increase in VDR expression after MI. Hence, these data along with the findings from this study suggest that cardiac fibrosis after MI may be regulated by the degree of vitamin D signaling in the heart. Activation of circulating and tissue RAS plays a key role in the pathophysiology of heart failure and ventricular remodel- J Appl Physiol • doi:10.1152/japplphysiol.01506.2012 • www.jappl.org Downloaded from http://jap.physiology.org/ by 10.220.32.247 on June 15, 2017 C † 986 Vitamin D Signaling Pathway After Myocardial Infarction GRANTS This work was supported in part by NIH Grants R01 HL65742 (P. Kang), the World Class University program (R31-20029) from Ministry of Education, Science and Technology, South Korea (P. Kang), and research support from Abbott Laboratories (P. Kang). DISCLOSURES The study was supported in part by Abbott Laboratories. AUTHOR CONTRIBUTIONS Author contributions: S.B., S.S.S., B.R.C., and P.M.K. conception and design of research; S.B., S.S.S., H.Y., J.Y.L., and B.R.C. performed experiments; S.B., S.S.S., H.Y., J.Y.L., B.R.C., and P.M.K. analyzed data; S.B., S.S.S., H.Y., J.Y.L., and P.M.K. interpreted results of experiments; S.B., S.S.S., H.Y., J.Y.L., and P.M.K. prepared figures; S.B., S.S.S., and P.M.K. drafted manuscript; S.B., S.S.S., and P.M.K. edited and revised manuscript; S.B., S.S.S., H.Y., J.Y.L., B.R.C., and P.M.K. approved final version of manuscript. Bae S et al. REFERENCES 1. Abbate A, Biondi-Zoccai GG, Bussani R, Dobrina A, Camilot D, Feroce F, Rossiello R, Baldi F, Silvestri F, Biasucci LM, Baldi A. Increased myocardial apoptosis in patients with unfavorable left ventricular remodeling and early symptomatic post-infarction heart failure. J Am Coll Cardiol 41: 753–760, 2003. 2. Agarwal R, Acharya M, Tian J, Hippensteel RL, Melnick JZ, Qiu P, Williams L, Batlle D. Antiproteinuric effect of oral paricalcitol in chronic kidney disease. Kidney Int 68: 2823–2828, 2005. 3. Bae S, Siu PM, Choudhury S, Ke Q, Choi JH, Koh YY, Kang PM. Delayed activation of caspase-independent apoptosis during heart failure in transgenic mice overexpressing caspase inhibitor CrmA. Am J Physiol Heart Circ Physiol 299: H1374 –H1381, 2010. 4. Bae S, Yalamarti B, Ke Q, Choudhury S, Yu H, Karumanchi SA, Kroeger P, Thadhani R, Kang PM. Preventing progression of cardiac hypertrophy and development of heart failure by paricalcitol therapy in rats. Cardiovasc Res 91: 632–639, 2011. 5. Baksi SN, Hughes MJ. Deficiency in dietary vitamin D, not calcium, alters noradrenergic responsiveness in rat atria in vitro. J Mol Cell Cardiol 18: 653–656, 1986. 6. Bodyak N, Ayus JC, Achinger S, Shivalingappa V, Ke Q, Chen YS, Rigor DL, Stillman I, Tamez H, Kroeger PE, Wu-Wong RR, Karumanchi SA, Thadhani R, Kang PM. Activated vitamin D attenuates left ventricular abnormalities induced by dietary sodium in Dahl salt-sensitive animals. Proc Natl Acad Sci USA 104: 16810 –16815, 2007. 7. Brondum-Jacobsen P, Benn M, Jensen GB, Nordestgaard BG. 25hydroxyvitamin D levels and risk of ischemic heart disease, myocardial infarction, and early death: population-based study and meta-analyses of 18 and 17 studies. Arterioscler Thromb Vasc Biol 32: 2794 –2802, 2012. 8. Brown AJ, Slatopolsky E. Drug insight: vitamin D analogs in the treatment of secondary hyperparathyroidism in patients with chronic kidney disease. Nat Clin Pract Endocrinol Metab 3: 134 –144, 2007. 9. Chen S, Glenn DJ, Ni W, Grigsby CL, Olsen K, Nishimoto M, Law CS, Gardner DG. Expression of the vitamin d receptor is increased in the hypertrophic heart. Hypertension 52: 1106 –1112, 2008. 10. Chen S, Law CS, Grigsby CL, Olsen K, Hong TT, Zhang Y, Yeghiazarians Y, Gardner DG. Cardiomyocyte-specific deletion of the vitamin D receptor gene results in cardiac hypertrophy. Circulation 124: 1838 – 1847, 2011. 11. Cheskis BJ, Freedman LP, Nagpal S. Vitamin D receptor ligands for osteoporosis. Curr Opin Investig Drugs 7: 906 –911, 2006. 12. Choi JH, Ke Q, Bae S, Lee JY, Kim YJ, Kim UK, Arbeeny C, Thadhani R, Kang PM. Doxercalciferol, a pro-hormone of vitamin D, prevents the development of cardiac hypertrophy in rats. J Card Fail 17: 1051–1058, 2011. 13. Choudhury S, Bae S, Ke Q, Lee JY, Kim J, Kang PM. Mitochondria to nucleus translocation of AIF in mice lacking Hsp70 during ischemia/ reperfusion. Basic Res Cardiol 106: 397–407, 2011. 14. Choudhury S, Bae S, Kumar SR, Ke Q, Yalamarti B, Choi JH, Kirshenbaum LA, Kang PM. Role of AIF in cardiac apoptosis in hypertrophic cardiomyocytes from Dahl salt-sensitive rats. Cardiovasc Res 85: 28 –37, 2010. 15. Cozzolino M, Ketteler M, Zehnder D. The vitamin D system: a crosstalk between the heart and kidney. Eur J Heart Fail 12: 1031–1041, 2010. 16. Dusso AS, Brown AJ, Slatopolsky E. Vitamin D. Am J Physiol Renal Physiol 289: F8 –F28, 2005. 17. Fogh K, Kragballe K. New vitamin D analogs in psoriasis. Curr Drug Targets Inflamm Allergy 3: 199 –204, 2004. 18. Freundlich M, Quiroz Y, Zhang Z, Zhang Y, Bravo Y, Weisinger JR, Li YC, Rodriguez-Iturbe B. Suppression of renin-angiotensin gene expression in the kidney by paricalcitol. Kidney Int 74: 1394 –1402, 2008. 19. Fryer RM, Rakestraw PA, Nakane M, Dixon D, Banfor PN, Koch KA, Wu-Wong JR, Reinhart GA. Differential inhibition of renin mRNA expression by paricalcitol and calcitriol in C57/BL6 mice. Nephron Physiol 106: 76 –81, 2007. 20. Garcia IM, Altamirano L, Mazzei L, Fornes M, Molina MN, Ferder L, Manucha W. Role of mitochondria in paricalcitol-mediated cytoprotection during obstructive nephropathy. Am J Physiol Renal Physiol 302: F1595–F1605, 2012. 21. Gotsman I, Shauer A, Zwas DR, Hellman Y, Keren A, Lotan C, Admon D. Vitamin D deficiency is a predictor of reduced survival in patients with heart failure; vitamin D supplementation improves outcome. Eur J Heart Fail 14: 357–366, 2012. J Appl Physiol • doi:10.1152/japplphysiol.01506.2012 • www.jappl.org Downloaded from http://jap.physiology.org/ by 10.220.32.247 on June 15, 2017 ing. In present study, vitamin D therapy significantly attenuated RAS gene activation in the heart, thereby demonstrating additional beneficial effects of vitamin D after MI. Several experimental studies have exhibited that vitamin D therapy effectively reduces renin transcript levels and plasma renin activity in mice (19, 30). Previous finding have also suggested that liganded VDR may play a direct role as a negative regulator of renin gene by specifically interacting with cyclic AMP response element (CRE) binding protein and preventing its association with CRE in the renin gene promoter (48). Furthermore, as a marker of chronic heart failure, vitamin D signaling downregulated several components of RAS in the kidneys of nephrectomized rats, including renin, renin receptor, angiotensinogen, and angiotensin II type 1 receptor (18, 38). In contrast, VDR KO mice have marked overproduction of renin (30, 47), leading to hypertension, cardiac enlargement, and elevation of natriuretic peptides. Thus these findings, along with our data, demonstrate that vitamin D therapy would be desirable for the treatment of heart failure after MI. In patients with end-stage heart failure, significantly low levels of serum 25-D levels are an independent risk factor associated with poor clinical outcomes and prolonged decompensated heart failure (7, 24, 26, 49). Distinctive VDR agonists such as calcitriol and its analogs, PC and doxercalciferol, were developed to treat secondary hyperparathyroidism in chronic kidney disease (8), osteoporosis (11), and psoriasis (17). In animal models, PC and doxercalciferol have demonstrated a beneficial effect on preventing cardiac dysfunction (12). However, calcitriol has caused nondesired hypercalcemic actions and contains a narrow therapeutic window. Therefore, correction may be better accomplished by analogs of calcitriol with a wider safety margin (45). Presently, researchers are focused on developing another selective VDR agonist drug candidate with high selectivity and efficacy to treat the heart failure phenotype and high-renin-associated dysfunctions (40). In summary, we have shown that activation of vitamin D signaling attenuates the progression to heart failure after MI, but defective VDR signaling exacerbates this deleterious effect. Given our evolving understanding of vitamin D and cardiovascular diseases, future studies are needed to determine whether vitamin D therapy could be an effective therapeutic agent for the treatment of heart failure. • Vitamin D Signaling Pathway After Myocardial Infarction Bae S et al. 987 36. O’Connell TD, Weishaar RE, Simpson RU. Regulation of myosin isozyme expression by vitamin D3 deficiency and 1,25-dihydroxyvitamin D3 in the rat heart. Endocrinology 134: 899 –905, 1994. 37. Odashima M, Usui S, Takagi H, Hong C, Liu J, Yokota M, Sadoshima J. Inhibition of endogenous Mst1 prevents apoptosis and cardiac dysfunction without affecting cardiac hypertrophy after myocardial infarction. Circ Res 100: 1344 –1352, 2007. 38. Porsti IH. Expanding targets of vitamin D receptor activation: downregulation of several RAS components in the kidney. Kidney Int 74: 1371– 1373, 2008. 39. Roger VL, Go AS, Lloyd-Jones DM, Benjamin EJ, Berry JD, Borden WB, Bravata DM, Dai S, Ford ES, Fox CS, Fullerton HJ, Gillespie C, Hailpern SM, Heit JA, Howard VJ, Kissela BM, Kittner SJ, Lackland DT, Lichtman JH, Lisabeth LD, Makuc DM, Marcus GM, Marelli A, Matchar DB, Moy CS, Mozaffarian D, Mussolino ME, Nichol G, Paynter NP, Soliman EZ, Sorlie PD, Sotoodehnia N, Turan TN, Virani SS, Wong ND, Woo D, Turner MB. Heart disease and stroke statistics– 2012 update: a report from the American Heart Association. Circulation 125: e2–e220, 2012. 40. Simpson RU. Selective knockout of the vitamin d receptor in the heart results in cardiac hypertrophy: is the heart a drugable target for vitamin D receptor agonists? Circulation 124: 1808 –1810, 2011. 41. Simpson RU, Hershey SH, Nibbelink KA. Characterization of heart size and blood pressure in the vitamin D receptor knockout mouse. J Steroid Biochem Mol Biol 103: 521–524, 2007. 42. Tan X, Li Y, Liu Y. Paricalcitol attenuates renal interstitial fibrosis in obstructive nephropathy. J Am Soc Nephrol 17: 3382–3393, 2006. 43. Tan X, Wen X, Liu Y. Paricalcitol inhibits renal inflammation by promoting vitamin D receptor-mediated sequestration of NF-kappaB signaling. J Am Soc Nephrol 19: 1741–1752, 2008. 44. Weishaar RE, Simpson RU. Involvement of vitamin D3 with cardiovascular function. II. Direct and indirect effects. Am J Physiol Endocrinol Metab 253: E675–E683, 1987. 45. Wu-Wong JR. Potential for vitamin D receptor agonists in the treatment of cardiovascular disease. Br J Pharmacol 158: 395–412, 2009. 46. Wu G, Rana JS, Wykrzykowska J, Du Z, Ke Q, Kang P, Li J, Laham RJ. Exercise-induced expression of VEGF and salvation of myocardium in the early stage of myocardial infarction. Am J Physiol Heart Circ Physiol 296: H389 –H395, 2009. 47. Xiang W, Kong J, Chen S, Cao LP, Qiao G, Zheng W, Liu W, Li X, Gardner DG, Li YC. Cardiac hypertrophy in vitamin D receptor knockout mice: role of the systemic and cardiac renin-angiotensin systems. Am J Physiol Endocrinol Metab 288: E125–E132, 2005. 48. Yuan W, Pan W, Kong J, Zheng W, Szeto FL, Wong KE, Cohen R, Klopot A, Zhang Z, Li YC. 1,25-dihydroxyvitamin D3 suppresses renin gene transcription by blocking the activity of the cyclic AMP response element in the renin gene promoter. J Biol Chem 282: 29821–29830, 2007. 49. Zittermann A, Schleithoff SS, Gotting C, Dronow O, Fuchs U, Kuhn J, Kleesiek K, Tenderich G, Koerfer R. Poor outcome in end-stage heart failure patients with low circulating calcitriol levels. Eur J Heart Fail 10: 321–327, 2008. J Appl Physiol • doi:10.1152/japplphysiol.01506.2012 • www.jappl.org Downloaded from http://jap.physiology.org/ by 10.220.32.247 on June 15, 2017 22. Han Y, Chen YS, Liu Z, Bodyak N, Rigor D, Bisping E, Pu WT, Kang PM. Overexpression of HAX-1 protects cardiac myocytes from apoptosis through caspase-9 inhibition. Circ Res 99: 415–423, 2006. 23. Holick MF. Vitamin D deficiency. N Engl J Med 357: 266 –281, 2007. 24. Karakas M, Thorand B, Zierer A, Huth C, Meisinger C, Roden M, Rottbauer W, Peters A, Koenig W, Herder C. Low levels of serum 25-Hydroxyvitamin D are associated with increased risk of myocardial infarction, especially in women: results from the MONICA/KORA Augsburg Case-Cohort Study. J Clin Endocrinol Metab 98: 272–280, 2013. 25. Kitahara T, Takeishi Y, Harada M, Niizeki T, Suzuki S, Sasaki T, Ishino M, Bilim O, Nakajima O, Kubota I. High-mobility group box 1 restores cardiac function after myocardial infarction in transgenic mice. Cardiovasc Res 80: 40 –46, 2008. 26. Laguardia SP, Dockery BK, Bhattacharya SK, Nelson MD, Carbone LD, Weber KT. Secondary hyperparathyroidism and hypovitaminosis D in African-Americans with decompensated heart failure. Am J Med Sci 332: 112–118, 2006. 27. Lee JH, O’Keefe JH, Bell D, Hensrud DD, Holick MF. Vitamin D deficiency an important, common, and easily treatable cardiovascular risk factor? J Am Coll Cardiol 52: 1949 –1956, 2008. 28. Lee W, Kang PM. Vitamin D deficiency and cardiovascular disease: Is there a role for vitamin D therapy in heart failure? Curr Opin Investig Drugs 11: 309 –314, 2010. 29. Li Y, Spataro BC, Yang J, Dai C, Liu Y. 1,25-dihydroxyvitamin D inhibits renal interstitial myofibroblast activation by inducing hepatocyte growth factor expression. Kidney Int 68: 1500 –1510, 2005. 30. Li YC, Kong J, Wei M, Chen ZF, Liu SQ, Cao LP. 1,25-Dihydroxyvitamin D(3) is a negative endocrine regulator of the renin-angiotensin system. J Clin Invest 110: 229 –238, 2002. 31. Lydia A, Asanuma K, Nonaka K, Takagi M, Jeong KH, Kodama F, Asao R, Asanuma E, Prodjosudjadi W, Tomino Y. Effects of 22-oxacalcitriol on podocyte injury in adriamycin-induced nephrosis. Am J Nephrol 35: 58 –68, 2012. 32. Mizobuchi M, Morrissey J, Finch JL, Martin DR, Liapis H, Akizawa T, Slatopolsky E. Combination therapy with an angiotensin-converting enzyme inhibitor and a vitamin D analog suppresses the progression of renal insufficiency in uremic rats. J Am Soc Nephrol 18: 1796 –1806, 2007. 33. Moller JE, Dahlstrom U, Gotzsche O, Lahiri A, Skagen K, Andersen GS, Egstrup K. Effects of losartan and captopril on left ventricular systolic and diastolic function after acute myocardial infarction: results of the Optimal Trial in Myocardial Infarction with Angiotensin II Antagonist Losartan (OPTIMAAL) echocardiographic substudy. Am Heart J 147: 494 –501, 2004. 34. Nian M, Lee P, Khaper N, Liu P. Inflammatory cytokines and postmyocardial infarction remodeling. Circ Res 94: 1543–1553, 2004. 35. O’Connell TD, Berry JE, Jarvis AK, Somerman MJ, Simpson RU. 1,25-Dihydroxyvitamin D3 regulation of cardiac myocyte proliferation and hypertrophy. Am J Physiol Heart Circ Physiol 272: H1751–H1758, 1997. •