Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
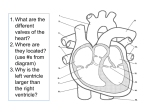
Slide 1 This paper studied the estimation error of aortic pressure by an adaptive observer, which is employed in the control of a permanent left ventricular assist device. Slide 2 This slide show a simplified model of human circulatory system. It has three blocks: left ventricle, arteries, vein and right atrium. The pulmonary circulation is simplified as a power resource P, and muscle pump effect in exercise is simplified as another power resource m. In this model, left ventricle is modeled as a variable capacitance CLV. Diodes D1 and D2 are used to model the one-way valves in the heart. TPR, the resistance of peripheral blood vessels is modeled as a variable resistor, to accommodate its large variation in different activity levels. RV, the resistance of the vein, has a small value. Annotation of the circuit: CLV: Left Ventricle; CA: Aorta; CV: Systemic vein and right atrium; D1: Aortic valve; D2: Mitral Valve; TPF: total peripheral flow; TPR: total peripheral resistance; L: blood inertia in peripheral circulation; RLV: resistance of aortic valve; RV: resistance of vein and left atrium; m: the mean pressure disturbance generated by muscle pump function in exercise, P: pressure disturbance generated by pulmonary circulation. Slide 3 Based on the simplified circuit shown in the last slide, the state space model in systole and diastole are modeled. The states are defined as: x1 = PLV PA, x2 = PV PA, x3 = TPF. Except the four elements in the blue box, and system matrix of the two model are the same. Actually if 1/RV=0, these two system matrices will be equal. The input LV in the systolic state space equation is the disturbance caused by the left ventricular capacitance variation during systole. The value of LV depends upon the heart rate, systole/diastole ratio, and the contractility of the natural left ventricle. It together with CA (the compliance of the aorta), and TPR (total peripheral resistance), may change for a LVAD patient over time, and are studied in this paper. TPR, the resistance of blood vessel, may have a large variation in different activity levels. Slide 4 Based on the two models found in last slide, a single state space equation is proposed to model the response of circulatory system. In this single equation model, there is one non physical parameter RV’ replacing RV, and there is no LV. The influence of LV (from variation of heart rate, contractility, and systole/diastole ratio) covered by RV’ . The value of this artificial parameter can be derived from measurement in initial stage of surgery as described by this equation. It will change when heart rate, contractility, or systole/diastole ratio changed, thus influence the accuracy of the single-equation model. The aortic pressure hat(PA), the signal of interest for physiological controller, is a function of states x1 and x2. The parameters of interest, which may change over time are RV', CA, TPR, Slide 5 Using P that can be obtained from magnetically suspended pump position sensor, not pressure sensor, the state observer equation can be rearranged as this algebraic equation. In this equation, only TPR is assumed varied. All other parameters are fixed. Then the normalized gradient algorithm is used to estimation the large varying parameter TPR, which is then plugged in adaptive observer to estimate states, and in turn to derive the aortic pressure using this equation. Slide 6 Now, we have the estimation algorithm for aortic pressure developed, and let us study its estimation performance. This simulink file is the simulation study environment for the estimation algorithm. The variation of parameters and input of interested that we discussed before can all be simulated in this model. Slide 7 This slide shows the experimental study environment for the estimation algorithm. Slide 8 Several scenarios have been studied in simulation or experiment, such as: (as in the slides) These cases simulate a lot of variation that may happen for a LVAD patient in long term. Slide 9 As shown in this slide, the value of RV’ is not fixed. It will decrease with the increase of heart rate, and be less with longer systole (larger systole/diastole ratio). Slide 10 Then we fix the heart rate at 75 beats per minute and Systole/Diastole ratio at 40:60 to study the relation between RV’ and the ratio between the flow contributed by the natural left ventricle and the total flow to the circulatory system. Q8 is the flow contributed by the natural left ventricle, and Qs is the summation of the left ventricle outflow and the pump flow. “-” here annotate average value. The increase of left ventricular flow ratio is achieved by increasing the contractility of left ventricle, namely the strength of the LV. Obviously, higher Q8/Qs means higher value of RV’. If using a fixed value of RV’ labeled by the yellow star for simulation study, we can also predict that the numerical value of estimation error will decrease when LV is stronger. Slide 11 Now let us study if you the fixed value of RV’ shown by the yellow star in the last slide and this slide, what will happen to the estimation error of TPR and aortic pressure. The horizontal axis of this plot is the ratio between the flow contributed by the left ventricle and the total flow rate. The top two are the trajectories of the estimation error for aortic pressure and total peripheral resistance respectively. The bottom two shows the peak to peak value of the total flow rate and the pump flow rate respectively. The flow rate in this slide is provided by the optimal adaptive controller, thus exhibiting oscillation. The increase of left ventricular flow ratio is achieved by increasing the contractility of left ventricle, which also increase the peak to peak value of total flow. Starting from the red vertical dashed line, the pump flow turns negative in a portion of diastole. Before the red dashed line, the numerical value of estimation error decreases because of the effect that RV’ is increasing. With the appearance of negative pump flow (larger oscillation), the model error besides RV’ of the single-equation model become dominant, which increase the numerical value of estimation error. The absolute value of estimation error of aortic pressure is within 3 mmHg over the whole simulation range. Slide 12 With the increase of arterial elastance (reciprocal of arterial compliance), the peak to peak value of pump flow rate and total flow will increase, decreases the numerical value of estimation error. Using the fixed value of RV’ corresponding to the yellow star on the figure, the numerical value of estimation error will decrease with the increase of the elastance. However, it is worth point out, for a single patient, the variation of arterial elastance is much narrow than the studied range, thus will have much less variation of estimation error (less than about 4.5 mmHg shown in this simulation). Slide 13 In this slide, we study the estimation performance of the adaptive observer at the presence of large TPR variation. This slide shows the experimental study in mock circulatory loop. When TPR is varied, with other parameters unchanged, the estimated TPR and estimated aortic pressure tracks the actual TPR and actual pressure with less oscillation and some delay. The mean value of total peripheral flow (TPF) is equal to the mean value of pump flow in this simulation, with less oscillation because of the damping effect in the circulation system. As shown in the bottom plot, the gain of estimator adapt in the presence of TPR variation. Overall, this study shows that the estimation error is small in the presence of TPR variation, thus suitable for physiological controller of the permanent LVAD. Annotation of this figure: (PA: aortic pressure; PA^: the estimated aortic pressure; TPR: total peripheral resistance; TPREST: estimated TPR by adaptive observer; Q: pump flow; TPF: the total peripheral flow; LO1: the first element of the adaptive observer gain) Slide 14 As we demonstrated in simulation study before, and also shown in this small figure that, the value of RV’ actually change with the variation of heart rate and systole/diastole ratio. If using the fixed value of RV’ (as shown by the yellow star) and run the experimental testing, the estimation error of aortic pressure, as shown in this large figure, will increase with the increase of heart rate; following the opposite trend of variation of RV’ shown before as predicted. The effect of Systole/Diastole ratio is not consistent, partially because the experimental mock loop does not have the same value as the Simulink file. (Dr. Tao, I also want to point out that the range of the heart rate in computer simulation and experiments are different because the experiment set up can not achieve the range of the computer simulation) Slide 15 As show by the experimental study, at the large variation of TPR of LVAD patient, the adaptive observer maintains good estimation performance, making it suitable for controller design of permanent LVAD. Also we can see there is definite relation between systemic parameters (CA, heart rate, contractility, systole/diastole ratio) and the estimation error. Using this relationship, if acquiring pressure estimation error, as may happen when patients have routine check, the systemic parameters of patient may be derived. All the simulation studies cover a very wide range, which usually do not happen for any patient. For any patient, the variation of systemic parameter except TPR and Heart rate are usually very small over short period, with the properly derived constant value for RV’, the estimation error is very small (within a couple of mmHg), thus suitable for physiological control of LVAD.