Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
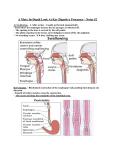
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2013;11:354 –358 ADVANCES IN TRANSLATIONAL SCIENCE Joseph H. Sellin, Section Editor Tissue Engineering the Small Intestine RYAN G. SPURRIER and TRACY C. GRIKSCHEIT Division of Pediatric Surgery, Children’s Hospital Los Angeles, Keck School of Medicine of the University of Southern California, Los Angeles, California Short bowel syndrome (SBS) results from the loss of a highly specialized organ, the small intestine. SBS and its current treatments are associated with high morbidity and mortality. Production of tissue-engineered small intestine (TESI) from the patient’s own cells could restore normal intestinal function via autologous transplantation. Improved understanding of intestinal stem cells and their niche have been coupled with advances in tissue engineering techniques. Originally described by Vacanti et al of Massachusetts General Hospital, TESI has been produced by in vivo implantation of organoid units. Organoid units are multicellular clusters of epithelium and mesenchyme that may be harvested from native intestine. These clusters are loaded onto a scaffold and implanted into the host omentum. The scaffold provides physical support that permits angiogenesis and vasculogenesis of the developing tissue. After a period of 4 weeks, histologic analyses confirm the similarity of TESI to native intestine. TESI contains a differentiated epithelium, mesenchyme, blood vessels, muscle, and nerve components. To date, similar experiments have proved successful in rat, mouse, and pig models. Additional experiments have shown clinical improvement and rescue of SBS rats after implantation of TESI. In comparison with the group that underwent massive enterectomy alone, rats that had surgical anastomosis of TESI to their shortened intestine showed improvement in postoperative weight gain and serum B12 values. Recently, organoid units have been harvested from human intestinal samples and successfully grown into TESI by using an immunodeficient mouse host. Current TESI production yields approximately 3 times the number of cells initially implanted, but improvements in the scaffold and blood supply are being developed in efforts to increase TESI size. Exciting new techniques in stem cell biology and directed cellular differentiation may generate additional sources of autologous intestinal tissue for direct translation to human therapy. Keywords: Tissue Engineering; Small Intestine; Short Bowel Syndrome; Organoid Unit; Stem Cell; Regeneration. Technological Primer S hort bowel syndrome (SBS) describes the constellation of metabolic, nutritional, and physiological derangements resultant from the loss of 70%–75% of small bowel length. It is a highly morbid condition, often resulting in failure to thrive and multiorgan system dysfunction.1,2 Disease processes in the adult population resulting in SBS include ischemia, inflamma- tory bowel disease, and trauma, whereas intestinal atresias, necrotizing enterocolitis, Hirschsprung’s disease, volvulus, and gastroschisis predominate among pediatric patients.3 To date, no reliable, curative therapy has been developed, and most patients are initially managed with lifestyle modification and total parenteral nutrition (TPN). Long-term TPN carries a high risk of central line sepsis and parenteral nutrition–associated liver disease.4 Although evolving understanding of parenteral nutrition–associated liver disease and the use of fish oil– based lipid emulsions composed of omega-3 fatty acids show promise in reducing such complications, morbidity remains high.5,6 Novel therapies such as teduglutide, a glucagon-like peptide 2 analogue, may restore intestinal structural and functional integrity by promoting repair and growth of the mucosa. Multiple randomized placebo-controlled trials among SBS patients have shown intestinotrophic and proabsorptive effects, with resultant reduction in need for parenteral support.7–9 Despite these advances in medical therapy, many SBS patients will require surgical intervention such as a bowel lengthening procedure or intestinal transplant. Surgical procedures for bowel lengthening have been refined during the past few decades and include longitudinal intestinal lengthening and tailoring and serial transverse enteroplasty among others.10 A recent review of autologous intestinal reconstruction surgery showed successful transition to enteral feeding among TPNdependent patients at a rate of 67% after longitudinal intestinal lengthening and tailoring and 34% after serial transverse enteroplasty.11 Other patients, such as those with near-total loss of small bowel length, require intestinal transplant if they fail more conservative treatments. As the largest immune organ in the body, the intestine is highly immunogenic and fails engraftment at much higher rates than other transplanted organs despite lifelong immunosuppression, which itself is fraught with numerous consequences.12–14 Other limitations also exist including the low numbers of available donor organs, particularly in the pediatric population.15 Despite all of the above interventions, the overall 5-year mortality for patients with SBS is 30% and as high as 45% among pediatric patients requiring small bowel transplant.1,16,17 Therefore, alternative solutions to this complex problem are being investigated. Tissue engineering could provide syngeneic intestinal tissue for autologous transplantation via in vitro manipulation of Abbreviations used in this paper: SBS, short bowel syndrome; TESI, tissue-engineered small intestine; TPN, total parenteral nutrition. © 2013 by the AGA Institute 1542-3565/$36.00 http://dx.doi.org/10.1016/j.cgh.2013.01.028 April 2013 stem cells. This field uses a combination of principles from engineering and developmental biology. The goal of current intestinal engineering efforts is to treat patients with SBS by providing replacement tissue with structure and function indistinguishable from native intestine. Findings The microstructure of the intestinal epithelium is composed of crypts and villi. There is a division of labor among the differentiated cell types of the villi to provide efficient transport across this large surface area. Goblet cells secrete mucus that contains important peptides such as Muc2. Enteroendocrine cells regulate multiple hormone-dependent processes.18 Enterocytes are responsible for the critical role of nutrient absorption. Within the crypts are Paneth cells interspersed between the rapidly cycling Lgr5⫹ intestinal stem cells. Paneth cells have long been known to contribute to the gut barrier via production of defensins and antimicrobial peptides, whereas their role in maintaining the microcellular stem cell niche through signaling via WNT and Notch continues to be studied.19 –22 The intestinal stem cell has 2 roles that facilitate the rapid turnover of the epithelium: self-replication into identical daughter cells and differentiation into the various differentiated epithelial cell types.18 The specific location of the intestinal stem cell has long been debated but was initially described by Bjerknes and Cheng.23 They defined crypt-based columnar cells that populate the base of the crypts between Paneth cells. Through lineage tracing, these crypt-based columnar cells were confirmed as the origin of all 4 differentiated cell types of the small intestine.24,25 Although characterized as within the crypt base, the intestinal stem cell is not readily identifiable by microscopy, so investigators sought a definitive cell marker. The first such marker, Lgr5, was found to be expressed by crypt base cells adjacent to Paneth cells. Hans Clevers of the Hubrecht Institute showed these Lgr5 cells to be multipotent, thus confirming the identity of intestinal epithelial stem cells.26 Another marker, Bmi1, was found in cells located predominantly 4 cells above the crypt base (or ⫹4). These Bmi1 cells are also multipotent and required for crypt maintenance.27 These 2 groups of intestinal stem cells are now understood to serve complementary functions, with a quiescent Bmi1 population at ⫹4 and Lgr5 for rapid turnover at the crypt base.28 Numerous additional markers of putative intestinal stem cells have also been proposed including Mushashi-1 (Msi-1), doublecortin-like kinase 1 (DCLK1), mouse telomerase reverse transcriptase (mTert), and prominin 1 (Prom1).29 –33 These advances in stem cell biology occurred in parallel with the development of the field of tissue engineering. In 1988, Vacanti et al of Massachusetts General Hospital initiated in vivo implantation of organoid units, multicellular clusters of epithelium and mesenchyme harvested from rat intestine, in a variation from an original protocol by Evans et al.34,35 These clusters were loaded onto a scaffold that provided physical support and allowed for angiogenesis and vasculogenesis of the developing tissue. After a period of weeks, the tissue-engineered intestine was harvested and examined.34,35 Subsequent investigations have resulted in the growth of every region of the gastrointestinal tract including tissue-engineered esophagus, stomach, small intestine, and colon in rodent models.36 –39 Tissue-engineered colon, esophagus, and small intestine have had their rudimentary function confirmed TISSUE ENGINEERING THE SMALL INTESTINE 355 in replacement models.38,40,41 In the case of tissue-engineered small intestine (TESI), histologic analyses demonstrated the presence of all 4 differentiated intestinal cell types, which confirmed the similarity of TESI to native intestine (Figure 1).37,42 Beyond the epithelium, TESI contains the same key components as native tissue necessary for function: blood vessels, muscle, and nerve components. TESI mesenchyme contains intestinal subepithelial myofibroblasts to contribute to wound healing and immunity. All of these tissues have been confirmed to originate from the TESI donor rather than the host.37 The many transgenic tools of the murine model may facilitate further investigation into the mechanism of tissue formation. Importance of Findings Beginning in the late 1980s with intestinal cell cultures in vitro, Evans et al34 demonstrated the ability to grow rat intestinal epithelial cells in culture by modifying conditions such as culture medium and growth factors. Further modifications to in vitro conditions of cell culture, including creation of a microgravity environment with a rotating bioreactor, have facilitated the growth of villus-like structures from a monolayer of fibroblasts and endothelial cells.43 Recently, single Lgr5⫹ stem cells have been cultured in vitro without mesenchymal cells and successfully developed into crypt and villus structures. However, these single cells yielded organoids in only 6% of cultures and required the support of basement membrane preparation (Matrigel; BD Biosciences, San Jose, CA) and supplementation of multiple exogenous signals usually produced by supporting niche cells.44 Although cell culture methods are capable of producing differentiated intestinal epithelium, such in vitro techniques have been unable to produce vasculature or supporting mesenchyme, which has proved crucial for maintaining the stem cell niche.22 In this regard and others, the in vivo tissue engineering model is unique and more suited to human therapy. Translation of Findings Into Routine Clinical Diagnosis and Treatment Beyond replicating the structure of native intestine and defining the underlying molecular mechanisms, the ultimate goal of tissue engineering is treatment of SBS. To that end, a number of experiments have been undertaken in animals that demonstrate feasibility for translation of TESI therapy to humans. Grikscheit et al were able to demonstrate clinical improvement after rescue with TESI by using a Lewis rat model of SBS. As compared with the group that underwent massive enterectomy alone, the TESI group showed improvement in postoperative weight gain and serum B12 levels.40 With evidence that TESI therapy experimentally improves SBS outcomes, the next logical step was to engineer small intestine in a large animal model that was representative of human scale. Therefore, Sala et al42 harvested small intestine for organoid unit preparation from Yorkshire swine. With the donor animal still under anesthesia, autologous organoid units were loaded onto a biodegradable scaffold and implanted into the omentum of the animal during the same operation. The results demonstrated that successful growth of TESI was a promising pilot for future investigational new drug—enabling large animal studies. 356 SPURRIER AND GRIKSCHEIT CLINICAL GASTROENTEROLOGY AND HEPATOLOGY Vol. 11, No. 4 Figure 1. TESI in the mouse model demonstrates normal epithelial differentiation. (A) Alcian blue staining of the goblet cells in the native and the tissue-engineered small intestine, respectively. (B) Lysozyme staining demonstrates presence of Paneth cells in their crypt location in tissueengineered intestine and native intestine. (C) Chromogranin A⫹B staining identifies enteroendocrine cells in both native and tissue-engineered intestine. (D) The brush border of the enterocytes is stained by using villin specific antibody in both tissues. Scale bar, 40.0 m. From Sala FG, Matthews JA, Speer AL, et al. A multicellular approach forms a significant amount of tissue-engineered small intestine in the mouse. Tissue Eng Part A 2011;17:1841–1850. Reprinted with permission from AAAS. The ability to engineer small intestine is not a phenomenon limited to animal tissues. Human organoid units have been implanted in immunodeficient mouse hosts and successfully grown into tissue-engineered small intestine and colon.45,46 On transition to human therapy, the patient will serve as his or her own bioreactor for autologous TESI growth, thus avoiding the need for immunosuppression. The TESI could then be moved on the vascular pedicle into position for surgical anastomosis. The blood supply of neovascularized omentum that supported its growth would remain intact. Although immediate processing and implantation of organoid units would be ideal, some patients may come to intestinal resection with clinical conditions that are temporarily unfavorable for immediate tissue engineering in the SBS patient’s omentum. In cases such as sepsis due to necrotizing enterocolitis, storage or in vitro expansion protocols may be required. mm in diameter constructed of polyglycolic acid and poly (l-lactic acid) coated with type I collagen (Figure 2). This material demonstrates 95% porosity to allow initial imbibition of nutrients. The type I collagen promotes initial cellular adhesion, and subsequently the scaffold slowly hydrolyzes to allow the TESI to continue growing without excessive concurrent foreign body reaction.37 Although TESI has demonstrated nerve cell growth, specific studies of peristalsis have not been performed. In interposition anastomosis, obstruction did not ensue. Motility will need to be directly measured as the size and length of TESI increase.37 Roadblocks and/or Limitations Some simple hollow viscus organs, such as the trachea, have been engineered on scaffolds without a dedicated blood supply and grown to scale for whole organ replacement.47 TESI has been found to contain approximately 3 times the number of cells initially implanted.37 Current research seeks to improve this yield and further amplify the implanted stem cell population, with the goal of producing enough tissue for whole organ replacement. Larger constructs would be more likely to grow with the support of a definitive blood supply rather than simple imbibition and neovascularization. However, simple anastomosis of a construct to host vasculature is not sufficient to support TESI growth, because attempts to implement larger acellular dermal matrices have failed.48 Although decellularized matrices have been investigated for their potential biocompatibility with native tissue and maintenance of architecture, inadequate porosity to allow imbibition of nutrients has limited their application.49 –53 Current TESI scaffolds are a highly porous tube ⬍5 Figure 2. Morphology of TESI in the mouse model. Four weeks after implantation, the tissue-engineered intestine formed a sphere about twice the size of the initial implanted polymer (arrow). From Sala FG, Matthews JA, Speer AL, et al. A multicellular approach forms a significant amount of tissue-engineered small intestine in the mouse. Tissue Eng Part A 2011; 17:1841–1850. Reprinted with permission from AAAS. April 2013 Differentiation of intestinal stem cells into each of the mature cell types results from an elegant and high-fidelity cellular traffic within the crypt that is not entirely defined. As understanding of the intestinal stem cell niche improves, an improved donor cell population may be substituted for the organoid units currently implanted. Alternatively, the Spence lab has demonstrated the novel approach to induce differentiation of human pluripotent stem cells into intestinal epithelium. In this in vitro model the addition of Wnt3a, Activin A, and fibroblast growth factor to human induced pluripotent stem cells was adequate for hindgut patterning, specification, and morphogenesis, with NEUROG3 transcription factor required for enteroendocrine cell development.54 The factors that contributed to this novel differentiation in vitro are among dozens of molecules within those families with unknown effects in vivo. Further effects of any growth factor must be defined before regulatory approval for transition to human therapy. Conclusions SBS results from the loss of a highly specialized organ, the small intestine. High morbidity and mortality are associated with both SBS and its current treatments. Tissue engineering is an emerging field with tremendous potential for novel therapies to treat these patients. Ideally, restoration of normal intestinal function would occur via autologous transplantation of TESI. In vitro and in vivo techniques have evolved such that modest amounts of small intestine can be reproducibly engineered from donor stem cells. Continued development of materials science may provide more efficient scaffolds or integrate composite biomaterials to support larger constructs. New techniques in stem cell biology and directed cellular differentiation may generate new sources of autologous intestinal tissue. With continued advancements in each of its disciplines, the future is promising for the field of tissue engineering in the small intestine. References 1. Wales PW, de Silva N, Kim J, et al. Neonatal short bowel syndrome: population-based estimates of incidence and mortality rates. J Pediatr Surg 2004;39:690 – 695. 2. Grikscheit TC, Vacanti JP. The history and current status of tissue engineering: the future of pediatric surgery. J Pediatr Surg 2002; 37:277–288. 3. Ueno T, Fukuzawa M. Current status of intestinal transplantation. Surg Today 2010;40:1112–1122. 4. Peyret B, Collardeau S, Touzet S, et al. Prevalence of liver complications in children receiving long-term parenteral nutrition. Eur J Clin Nutr 2011;65:743–749. 5. Fallon EM, Le HD, Puder M. Prevention of parenteral nutritionassociated liver disease: role of omega-3 fish oil. Curr Opin Organ Transplant 2010;15:334 –340. 6. Meisel JA, Le HD, de Meijer VE, et al. Comparison of 5 intravenous lipid emulsions and their effects on hepatic steatosis in a murine model. J Pediatr Surg 2011;46:666 – 673. 7. Jeppesen PB, Gilroy R, Pertkiewicz M, et al. Randomised placebocontrolled trial of teduglutide in reducing parenteral nutrition and/or intravenous fluid requirements in patients with short bowel syndrome. Gut 2011;60:902–914. 8. Jeppesen PB, Pertkiewicz M, Messing B, et al. Teduglutide reduces need for parenteral support among patients with short bowel syndrome with intestinal failure. Gastroenterology 2012; 143:1473–1481. TISSUE ENGINEERING THE SMALL INTESTINE 357 9. Jeppesen PB. Teduglutide, a novel glucagon-like peptide 2 analog, in the treatment of patients with short bowel syndrome. Therap Adv Gastroenterol 2012;5:159 –171. 10. Rege AS, Sudan DL. Autologous gastrointestinal reconstruction: review of the optimal nontransplant surgical options for adults and children with short bowel syndrome. Nutr Clin Pract 2012; 28:65–74. 11. Jones BA, Hull MA, Kim HB. Autologous intestinal reconstruction surgery for intestinal failure management. Curr Opin Organ Transplant 2010;15:341–345. 12. LaRosa C, Baluarte HJ, Meyers KE. Outcomes in pediatric solidorgan transplantation. Pediatr Transplant 2011;15:128 –141. 13. LaRosa C, Glah C, Baluarte HJ, et al. Solid-organ transplantation in childhood: transitioning to adult health care. Pediatrics 2011; 127:742–753. 14. Garg M, Jones RM, Vaughan RB, et al. Intestinal transplantation: current status and future directions. J Gastroenterol Hepatol 2011;26:1221–1228. 15. Lao OB, Healey PJ, Perkins JD, et al. Outcomes in children with intestinal failure following listing for intestinal transplant. J Pediatr Surg 2010;45:100 –107. 16. Wales PW, Christison-Lagay ER. Short bowel syndrome: epidemiology and etiology. Semin Pediatr Surg 2010;19:3–9. 17. Lao OB, Healey PJ, Perkins JD, et al. Outcomes in children after intestinal transplant. Pediatrics 2010;125:e550 – e558. 18. Potten CS, Gandara R, Mahida YR, et al. The stem cells of small intestinal crypts: where are they? Cell Prolif 2009;42:731–750. 19. Moore KA, Lemischka IR. Stem cells and their niches. Science 2006;311:1880 –1885. 20. Garcia MI, Ghiani M, Lefort A, et al. LGR5 deficiency deregulates Wnt signaling and leads to precocious Paneth cell differentiation in the fetal intestine. Dev Biol 2009;331:58 – 67. 21. Gregorieff A, Stange DE, Kujala P, et al. The ets-domain transcription factor Spdef promotes maturation of goblet and Paneth cells in the intestinal epithelium. Gastroenterology 2009;137:1333– 1345. 22. Farin HF, Van Es JH, Clevers H. Redundant sources of Wnt regulate intestinal stem cells and promote formation of Paneth cells. Gastroenterology 2012;143:1518 –1529. 23. Bjerknes M, Cheng H. The stem-cell zone of the small intestinal epithelium: IV— effects of resecting 30% of the small intestine. Am J Anat 1981;160:93–103. 24. Cheng H, Leblond CP. Origin, differentiation and renewal of the four main epithelial cell types in the mouse small intestine: I— columnar cell. Am J Anat 1974;141:461– 479. 25. Cheng H, Leblond CP. Origin, differentiation and renewal of the four main epithelial cell types in the mouse small intestine: V— unitarian theory of the origin of the four epithelial cell types. Am J Anat 1974;141:537–561. 26. Barker N, van Es JH, Kuipers J, et al. Identification of stem cells in small intestine and colon by marker gene Lgr5. Nature 2007; 449:1003–1007. 27. Sangiorgi E, Capecchi MR. Bmi1 is expressed in vivo in intestinal stem cells. Nat Genet 2008;40:915–920. 28. Li L, Clevers H. Coexistence of quiescent and active adult stem cells in mammals. Science 2010;327:542–545. 29. Dijkmans TF, van Hooijdonk LW, Fitzsimons CP, et al. The doublecortin gene family and disorders of neuronal structure. Cent Nerv Syst Agents Med Chem 2010;10:32– 46. 30. May R, Sureban SM, Hoang N, et al. Doublecortin and CaM kinase-like-1 and leucine-rich-repeat-containing G-protein-coupled receptor mark quiescent and cycling intestinal stem cells, respectively. Stem Cells 2009;27:2571–2579. 31. Zhu L, Gibson P, Currle DS, et al. Prominin 1 marks intestinal stem cells that are susceptible to neoplastic transformation. Nature 2009;457:603– 607. 32. Asai R, Okano H, Yasugi S. Correlation between Musashi-1 and 358 33. 34. 35. 36. 37. 38. 39. 40. 41. 42. 43. 44. 45. SPURRIER AND GRIKSCHEIT c-hairy-1 expression and cell proliferation activity in the developing intestine and stomach of both chicken and mouse. Dev Growth Differ 2005;47:501–510. Montgomery RK, Carlone DL, Richmond CA, et al. Mouse telomerase reverse transcriptase (mTert) expression marks slowly cycling intestinal stem cells. Proc Natl Acad Sci U S A 2011;108: 179 –184. Evans GS, Flint N, Somers AS, et al. The development of a method for the preparation of rat intestinal epithelial cell primary cultures. J Cell Sci 1992;101:219 –231. Vacanti JP, Morse MA, Saltzman WM, et al. Selective cell transplantation using bioabsorbable artificial polymers as matrices. J Pediatr Surg 1988;23:3–9. Speer AL, Sala FG, Matthews JA, et al. Murine tissue-engineered stomach demonstrates epithelial differentiation. J Surg Res 2011;171:6 –14. Sala FG, Matthews JA, Speer AL, et al. A multicellular approach forms a significant amount of tissue-engineered small intestine in the mouse. Tissue Eng Part A 2011;17:1841–1850. Grikscheit T, Ochoa ER, Srinivasan A, et al. Tissue-engineered esophagus: experimental substitution by onlay patch or interposition. J Thorac Cardiovasc Surg 2003;126:537–544. Grikscheit TC, Ochoa ER, Ramsanahie A, et al. Tissue-engineered large intestine resembles native colon with appropriate in vitro physiology and architecture. Ann Surg 2003;238:35– 41. Grikscheit TC, Siddique A, Ochoa ER, et al. Tissue-engineered small intestine improves recovery after massive small bowel resection. Ann Surg 2004;240:748 –754. Grikscheit TC, Ogilvie JB, Ochoa ER, et al. Tissue-engineered colon exhibits function in vivo. Surgery 2002;132:200 –204. Sala FG, Kunisaki SM, Ochoa ER, et al. Tissue-engineered small intestine and stomach form from autologous tissue in a preclinical large animal model. J Surg Res 2009;156:205–212. Salerno-Goncalves R, Fasano A, Sztein MB. Engineering of a multicellular organotypic model of the human intestinal mucosa. Gastroenterology 2011;141:e18 – e20. Sato T, Vries RG, Snippert HJ, et al. Single Lgr5 stem cells build crypt-villus structures in vitro without a mesenchymal niche. Nature 2009;459:262–265. Barthel ER, Levin DE, Speer AL, et al. Human tissue-engineered CLINICAL GASTROENTEROLOGY AND HEPATOLOGY Vol. 11, No. 4 46. 47. 48. 49. 50. 51. 52. 53. 54. colon forms from postnatal progenitor cells: an in vivo murine model. Regen Med 2012;7:807– 818. Levin DE, Barthel ER, Speer AL, et al. Human tissue-engineered small intestine forms from postnatal progenitor cells. J Pediatr Surg 2013;48:129 –137. Ott HC. Engineering tissues for children: building grafts that grow. Lancet 2012;380:957–958. Xu HM, Wang ZJ, Han JG, et al. Application of acellular dermal matrix for intestinal elongation in animal models. World J Gastroenterol 2010;16:2023–2027. Orlando G, Baptista P, Birchall M, et al. Regenerative medicine as applied to solid organ transplantation: current status and future challenges. Transpl Int 2011;24:223–232. Bhrany AD, Beckstead BL, Lang TC, et al. Development of an esophagus acellular matrix tissue scaffold. Tissue Eng 2006;12: 319 –330. Voytik-Harbin SL, Brightman AO, Kraine MR, et al. Identification of extractable growth factors from small intestinal submucosa. J Cell Biochem 1997;67:478 – 491. Hodde JP, Record RD, Liang HA, et al. Vascular endothelial growth factor in porcine-derived extracellular matrix. Endothelium 2001;8:11–24. McDevitt CA, Wildey GM, Cutrone RM. Transforming growth factor-beta1 in a sterilized tissue derived from the pig small intestine submucosa. J Biomed Mater Res A 2003;67:637– 640. Spence JR, Mayhew CN, Rankin SA, et al. Directed differentiation of human pluripotent stem cells into intestinal tissue in vitro. Nature 2011;470:105–109. Reprint requests Address requests for reprints to: Tracy C. Grikscheit, MD, 4650 Sunset Boulevard, Mailstop 35, Los Angeles, California 9002. e-mail: [email protected]; fax: (323) 361-3534. Conflicts of interest The authors disclose no conflicts. Funding Supported by California Institute for Regenerative Medicine RN2 00946-1 grant.