Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Management of acute coronary syndrome wikipedia , lookup
Remote ischemic conditioning wikipedia , lookup
Coronary artery disease wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Rheumatic fever wikipedia , lookup
Electrocardiography wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Congenital heart defect wikipedia , lookup
Heart failure wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
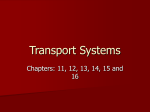
Plasma Urocortin 1 in Human Heart Failure Sue P. Wright, MBChB; Robert N. Doughty, MD, MRCP, FRACP; Chris M. Frampton, PhD; Greg D. Gamble, MSc; Tim G. Yandle, PhD; A. Mark Richards, MD, PhD, DSc, FRACP, FRSNZ Downloaded from http://circheartfailure.ahajournals.org/ by guest on May 2, 2017 Background—The urocortins are emerging as potentially important contributors to neurohumoral regulation of the circulation with recent reports attributing a powerful array of hemodynamic, renal, and neurohumoral effects to the urocortins in cardiac failure. These peptides also seem to have cardioprotective effects in the setting of ischemiareperfusion. Little is known concerning the plasma concentrations of the urocortins in health and disease. We have investigated plasma urocortin 1 as a potential diagnostic marker of heart failure and documented its relationships to symptoms, measures of cardiac function, and concurrent levels of other circulating neurohormones. Methods and Results—In 299 patients with recent onset dyspnea or peripheral edema presenting to primary care, plasma urocortin 1 and other vasoactive hormones were assayed, and echocardiography was performed. Heart failure was present in 74 patients (25%) according to predefined diagnostic criteria. Urocortin 1 levels were increased in patients with heart failure and were related to functional class, clinical signs of heart failure, echocardiographic indicators of left ventricular dimensions and function, plasma creatinine, and concurrent circulating levels of plasma natriuretic peptides, adrenomedullin, and endothelin 1. Conclusions—Plasma urocortin 1 is elevated in heart failure (in proportion to the degree of cardiac dysfunction) in concert with the generalized neurohormonal activation seen in this condition. Urocortin levels predict heart failure independent of age, history of previous myocardial infarction, diabetes, hypertension, fractional shortening, and N-terminal prohormone brain natriuretic peptide levels. (Circ Heart Fail. 2009;2:465-471.) Key Words: urocortin 䡲 heart failure 䡲 cardiac natriuretic peptides 䡲 adrenomedullin 䡲 endothelin T he urocortins are endogenous vasoactive peptides known to exert powerful beneficial neurohormonal, hemodynamic, and renal actions in experimental heart failure.1–5 In stable human heart failure infusions of urocortin 1, at the doses chosen, had little hemodynamic effect, whereas urocortin 2 markedly augmented cardiac output when reducing systemic vascular resistance.6,7 Urocortins have cardioprotective effects in experimental ischemia/reperfusion.8 Members of the corticotrophin releasing factor (CRF) family, the urocortins are ancient, with genetic profiling demonstrating their presence through 550 million years of evolution.9 The cDNA to urocortin 1 was cloned in 199510 and 2 related peptide sequences, named urocortin 2 and urocortin 3, were discovered subsequently.11–13 The gene for urocortin 1 is found in chromosome 2p23-2p21 and encodes a 123 amino acid polypeptide precursor.14,15 Urocortin 1 expression and peptide release are widespread in the body; occurring in the central nervous system, gastrointestinal tract, and heart, among other sites.16 –19 Plasma levels, metabolism, and regulation of the urocortins are still largely undefined. Urocortin expression and peptide release from cultured cardiomyocytes is increased by ischemia.20 Secretion in vitro is also enhanced by cytokines including interleukin-1 , interleukin-6, and tumor necrosis factor-␣21; factors elevated in heart failure and acute coronary syndromes. Urocortin expression is increased in hypertrophied rat hearts and in the cardiac ventricles of patients with both dilated and hypertrophic cardiomyopathy.18,22 Circulating levels in humans have been reported at ⬇8 pmol/L.23 In human heart failure, one report indicates levels are elevated but (perhaps unexpectedly) fall with increasing severity of symptoms as well as with reducing left ventricular ejection fraction (LVEF) and increasing age.24 Bioactivity and detectable immunoreactivity may be modulated by a CRF-binding protein present in humans but not in all mammalian species. This factor may play an inhibitory role in binding to urocortin and preventing receptor activation.25,26 Urocortins act predominantly through 2 receptor subtypes, CRF-1 and CRF-2. Receptors possess 7 transmembrane domains and are G-protein coupled. CRF-2(a) receptors constitute the dominant peripheral CRF-2 receptor form, particularly in the heart and vasculature.15,19 Receptor concentrations are high in the left ventricle and intramyocardial vessels.19 Received December 1, 2008; accepted June 19, 2009. From the Department of Medicine (S.P.W., R.N.D., G.D.G.), Faculty of Medicine and Health Sciences, University of Auckland, Auckland, New Zealand; and Christchurch Cardioendocrine Research Group (C.M.F., T.G.Y., A.M.R.) Department of Medicine, University of Otago, Christchurch, New Zealand. Correspondence to Mark Richards, MD, PhD, DSc, FRACP, FRSNZ, Department of Medicine, University of Otago, Christchurch, PO Box 4345, Christchurch, New Zealand. E-mail [email protected] © 2009 American Heart Association, Inc. Circ Heart Fail is available at http://circheartfailure.ahajournals.org 465 DOI: 10.1161/CIRCHEARTFAILURE.108.840207 466 Circ Heart Fail September 2009 In this study, we set out to establish whether or not plasma urocortin 1 levels were systematically elevated in the presence of symptomatic heart failure, and to establish the relationship of plasma concentrations of this peptide with concurrent symptomatic status, echocardiographic measurements of cardiac dimensions and function and with concurrent circulating concentrations of neurohormones known to be activated in the presence of heart failure. Methods Patients Downloaded from http://circheartfailure.ahajournals.org/ by guest on May 2, 2017 Patients were participants in the Natriuretic Peptides in the Community study, a prospective randomized trial of the diagnostic value of N-terminal prohormone brain natriuretic peptide (NT-proBNP) in diagnosis of suspected new onset heart failure in primary care.27 The protocol was approved by an ethics committee of the New Zealand Ministry of Health. All patients provided written informed consent. Patients presenting with breathlessness and/or peripheral edema were referred to the study by their family doctor. Each patient underwent further cardiological assessment including ECG, chest x-ray, and echocardiography (ATL HDI 5000). Blood samples for neurohormone assays were collected from seated patients without previous resting or other special patient preparation. Blood was collected into EDTA (7.5 mg/mL, Vacutainer; Becton Dickinson, Franklin Lakes, NJ) and centrifuged within 2 hours of venesection (3000 rpm for 10 minutes) with plasma stored at ⫺80°C before radioimmunoassay. The definitive diagnosis of heart failure was provided by a panel of 3 consultants who reviewed each clinical presentation and all test results (excluding neurohormone levels). The panel decided whether individual patients met the European Society of Cardiology diagnostic criteria for a diagnosis of heart failure.28 This required the presence of appropriate symptoms and signs of pulmonary or peripheral congestion and the presence of objective evidence of cardiac dysfunction. In the case of doubt, response to treatment was considered. This standard was based on that used in other recent studies of the diagnosis of heart failure.29,30 Radioimmunoassays Blood samples were collected using standard venipuncture technique into tubes containing EDTA. Samples were centrifuged and frozen at ⫺70°C before immunoassay. Urocortin 1 radioimmunoassay was performed on plasma samples, as described previously.31 Sample preparation included steps previously used to extract total CRF (bound⫹free) from human plasma. One milliliter of plasma was mixed with 2 mL methanol and centrifuged. The supernatant was adjusted to contain 0.003% Triton X-100, dried under an air stream at room temperature, and reconstituted in 0.5 mL assay buffer. For assay, 100 L plasma extract or standard plus 100 l antiserum PBL 5779 diluted 1:165 000 were incubated at 4°C for 24 hours before addition of 100 L radiolabel (I125) Tyr-Ucn-1 (prepared by the chloramine T method and purified by reverse phase high-performance liquid chromatography) containing 10 000 cpm. The assay was incubated for an additional 24 hours at 4°C after which bound and free label was separated by a solid phase second antibody (donkey anti-rabbit; Sac-Cell, IDS, Bolden, United Kingdom). The radioimmunoassay characteristics (mean⫾SD) include zero binding, 35.5⫾6.3% (n⫽25); standard curve 50% effective concentration, 414⫾69 pg/mL (88.1⫾14.6 pmol/L); and a detection limit of 6.6⫾2.7 pg/mL (1.4⫾0.6 pmol/L) in plasma after 2-fold concentration during extraction (n⫽25). Cross reactivity with urocortins 2 and 3 was ⬍0.004% and ⬍0.002% with human CRF, human urotensin 2, or the cardiac natriuretic peptides including atrial natriuretic peptide (ANP), brain natriuretic peptide (BNP), and NT-proBNP. Within assay coefficients of variation calculated from variance between assay duplicates were 13.4% over 0 to 52 pg/mL (0 to 11 pmol/L), 10.3% over 56 to 239 pg/mL (12 to 51 pmol/L), and 3.3% over 239 to 1490 pg/mL (51 to 317 pmol/L). Interassay coefficients of variation were 17.5% at 63 pg/mL (13.5 pmol/L; n⫽23), 16.2% at 111 pg/mL (23.7 pmol/L; n⫽20), and 13.3% at 145 pg/mL (30.9 pmol/L; n⫽23). Recovery of urocortin 1 added to plasma was 61.2% at 141 pg/mL (30 pmol/L), 60.9% at 329 pg/mL (70 pmol/L), and 59.3% at 470 pg/mL (100 pmol/L). Urocortin results are given without correction for recovery. The urocortin 1 reference range encompassing 95% of results for healthy subjects (2 to 16 pmol/L) was determined in 98 subjects drawn at random from the Christchurch, New Zealand, electoral roll and matched to the study population for age and gender. Immunoassays for NT-proBNP, BNP, ANP, NT-proANP, C-type natriuretic peptide, adrenomedullin, and endothelin-1 were measured using our previously validated and published radioimmunoassays.32–37 Statistical Methods Plasma concentrations of neurohormones are expressed as mean and standard deviation (when normally distributed) or median and interquartile range when skewed. Variables with nonnormal distributions were compared using the Wilcoxon rank test. Other continuous variables are compared by Student t tests. Categorical variables were compared with the Fisher exact test. In univariate analyses, Spearman rank coefficient was used to determine correlations between variables, presented as R values. Modeling to investigate independent determinants of urocortin 1 was performed by means of multiple linear regression models. Multiple logistic regression with a forward stepwise selection based on the significance of the Wald Score if a candidate variable were entered into the regression was used to test urocortin 1 and other variables for potential independent association with a diagnosis of heart failure. Urocortin 1 and NT-proBNP were compared for their ability to discriminate presence or absence of heart failure by receiver operating characteristic analysis.38 The authors had full access to the data and take full responsibility for the integrity of the data. All authors have read and agree to the manuscript as written. Results Patient Characteristics Two hundred ninety-nine patients with a median age of 72 years (range 40 to 95 years), 65% women, were included in the study (Table 1). Forty-nine percent of patients presented with dyspnea alone, 12% with edema alone, and 39% with both symptoms. There were 80, 109, 84, and 26 patients in New York Heart Association (NYHA) functional classes I, II, III, and IV, respectively. Seventy-four of 299 (25%) were diagnosed as having heart failure by the panel (8, 22, 27, and 17 in NYHA classes I, II, III, and IV, respectively). Underlying etiologies included ischemic heart disease in 27 (36%) and was multifactorial with contributions from 2 or more of ischemia, diabetes, hypertension, and/or atrial fibrillation in 23 (31%). Valvular heart disease was present in 5 patients (7%), dilated cardiomyopathy in 5 (7%), isolated diastolic heart failure in 11 (15%), and with cause unknown in a further 6 patients (8%). Common non– heart failure conditions leading to presentation among the other 225 patients included respiratory disease (exacerbation of chronic obstructive pulmonary disease and malignancies), myocardial ischemia with exertional dyspnea, and obesity. Other less frequent causes included anxiety with hyperventilation, thoracic deformity, and chronic pulmonary venous thromboembolic disease. Hypertension was similarly frequent in both heart failure (48%) and non– heart failure (53%) groups. However, diabetes (28% versus 10%; P⬍0.001), previous myocardial infarction (34% versus 8%; P⬍0.001) and prescription of both loop diuretics Wright et al A Heart Failure (n⫽74) Age, y 74 (11) 72 (11) 0.16 Gender, female 39 (51) 159 (70) 0.004 Atrial fibrillation 23 (30) 12 (5) ⬍0.0001 Heart rate, bpm 73 (16) 74 (15) 0.75 Systolic BP, mm Hg 140 (24) 148 (22) 0.007 Diastolic BP, mm Hg 76 (17) 80 (14) 0.024 0.114 (0.04) 0.09 (0.03) ⬍0.0001 58.6 (28.1) 69.6 (28.6) 0.02 N-CNP, pmol/L 32.4 (25.4, 39.4) 24.7 (21.0, 29.5) ⬍0.0001 CNP, pmol/L 1.85 (1.35, 2.15) 1.45 (1.13, 1.67) ⬍0.0001 Serum creatinine, mmol/L Creatinine clearance, mL/min Not Heart Failure (n⫽225) 10000 Clinical, Echo, and Hormone Variables P Neurohormones ANP, pmol/L Downloaded from http://circheartfailure.ahajournals.org/ by guest on May 2, 2017 NT-proANP, nmol/L 32 (26, 45) 1.77 (1.36, 2.44) 17 (12, 25) 0.77 (0.49, 1.17) ⬍0.0001 ⬍0.0001 30 (16, 45) 8 (5, 14) ⬍0.0001 NT-proBNP, pmol/L 183 (103, 319) 38 (20, 76) ⬍0.0001 Endothelin-1, pmol/L 1.7 (1.4, 2.1) 1.0 (2.6, 1.2) ⬍0.0001 Adrenomedullin, pmol/L 7.7 (6.5, 9.7) 7.4 (6.0, 8.8) 0.0126 BNP, pmol/L Echocardiographic variables LVEDD, mm 57.5 (10) 50.2 (5.8) ⬍0.0001 LVESD, mm 44.7 (11.5) 33.3 (6.3) ⬍0.0001 LV mass, g 229.7 (90.4) 177.6 (56.7) ⬍0.0001 Fractional shortening, % 23.9 (9.7) 34.3 (7.7) ⬍0.0001 LVEF, % 44.1 (14.7) 60.7 (9.9) ⬍0.0001 LA area, cm 26.2 (5.9) 20.7 (4.8) ⬍0.0001 E-wave velocity, cm/s 63.0 (22.5) 52.0 (17.1) ⬍0.0001 A-wave velocity, cm/s 58.3 (24.7) 69.1 (17.2) ⬍0.0001 E/A ratio 1.29 (0.84) 0.77 (0.30) 0.0003 4.9 (2.1) 6.0 (1.8) 0.0002 E⬘ E/E⬘ ratio 13.6 (6.7) 9.2 (3.9) 0.0014 Deceleration time, ms 175 (75) 215 (170) ⬍0.0001 Data are presented as mean (SD), n (%), or median (25th, 75th percentile). BP indicates blood pressurel LVEDD, left ventricular end diastolic diameter; LVESD, left ventricular end-systolic diameter. (38% versus 18%; P⬍0.001), and angiotensin-converting enzyme inhibitors (47% versus 20%; P⬍0.001) were more frequent in patients with heart failure. Plasma Urocortin 1 Concentrations Mean plasma urocortin 1 in normal control subjects at 7.2⫾2.9 pmol/L (n⫽98) was significantly lower than levels recorded in the 225 non– heart failure symptomatic patients (11.1⫾3.2 pmolL), which in turn were lower than in the 74 patients with a final diagnosis of heart failure (13.6⫾4.1 pmol/L; P⬍0.001 for all intergroup comparisons). Levels of urocortin 1 and NT-proBNP in symptomatic subjects with and without a final diagnosis of heart failure are compared in Figure 1. Urocortin levels fell within a much tighter distribution and heart failure induced lesser absolute and proportional increments in urocortin 1 than in NT-proBNP. The significant intergroup differences in plasma urocortin 1 were independent of age and gender. Levels were significantly higher in men than in women in normal subjects and in the study population, whether the study group was considered B p<0.001 Urocortin I (pmol/L) Patient Characteristics NT-proBNP (pmol/L) Table 1. Plasma Urocortin 1 in Human Heart Failure 1000 100 10 1 467 10000 1000 100 p<0.001 10 1 N n=225 HF n=74 N n=225 HF n=74 Figure 1. Plasma NT-proBNP (A) and urocortin 1 (B) box plots showing median, 25th and 75th percentiles, and smallest and largest values. Identical axes are used to display both skewed NT-proBNP data and normally distributed urocortin 1 data to facilitate direct comparison. For both peptides, levels in heart failure are significantly higher than in patients with symptoms from other causes (P⬍0.001 for both urocortin 1 and NT-proBNP). in totality or separately for those with and without a final diagnosis of heart failure (Table 2). No significant relationship to age was seen in the study group, the normal reference range population, or in any subgroup. We also observed the expected increases in other neurohormones in heart failure (Table 1). Urocortin 1 levels were related to symptoms, exhibiting stepwise increases from 10.6⫾1.3 to 10.8⫾1.3, 11.5⫾1.4, and 13.3⫾1.5 pmol/L in NYHA functional classes I through IV, respectively (P⫽0.007) for the group overall. A similar trend was seen in the 74 patients with a final diagnosis of heart failure (11.5⫾3.5; 12.4⫾2.5; 14.3⫾4.3; and 14.6⫾5.0 pmol/L, respectively). Levels from patients in NYHA classes I and II combined were compared with those in NYHA classes III and IV combined. Severe symptoms (NYHA III/IV, n⫽44) were associated with significantly higher mean plasma urocortin 1 levels than mild (NYHAI/II, n⫽30) symptoms (14.4⫾3.9 pmol/L versus 12.1⫾3.9 pmol/L; P⫽0.017). Table 2. Plasma Urocortin 1 Levels in Normal, Heart Failure, and Non–Heart Failure Groups Plasma Urocortin 1, pmol/L n (Mean⫾SD) Normal Total 98 7.2⫾2.9 M 33 9.1⫾2.7 F 65 6.4⫾2.6 Heart failure Total 74 13.6⫾4.1 M 37 14.6⫾4.5 F 37 12.5⫾2.6 Non–heart failure illness Total 225 11.1⫾3.2 M 68 12.1⫾3.3 F 157 10.7⫾3.1 All 3 groups total values differ (P⬍0.001 for all pair-wise comparisons). Mean values in males (M) are greater than in females (F) in all 3 groups (P⬍0.001 for all). Circ Heart Fail NT-proBNP (pmol/L) 468 September 2009 Table 3. Multivariable Analysis for Independent Predictors of Heart Failure 1000 n=299 r=0.293 (0.19-0.39) p<0.001 10 1 BNP (pmol/L) 1000000 n=294 r=0.311(0.20-0.41) p<0.001 100 1 10 n=286 r=0.384(0.28-0.48) p<0.001 1 0.1 10000 ADM (pmol/L) Downloaded from http://circheartfailure.ahajournals.org/ by guest on May 2, 2017 CNP (pmol/L) 10000 1000 n=298 r=0.331(0.23-0.43) p<0.001 100 10 100 ET (pmol/L) Hazard Ratio 95% CI Urocortin 1, median 2.97 1.39 – 6.38 NTproBNP, median 7.12 2.71–18.70 Age, per 10-y increment 1.28 0.78–2.13 0.328 LVEF, per 1% fall 1.08 1.04–1.11 ⬍0.001 Prior MI 2.27 0.95–5.92 0.063 Diabetes 3.80 1.39–10.42 0.009 Estimated GFR, per 40 mL/min decline 1.58 0.71–3.53 0.261 100 10 n=292 r=0.244(0.13-0.35) p<0.001 1 0.1 0 10 20 30 Urocortin I (pmol/L) Figure 2. Plasma urocortin 1 (in patients presenting with dyspnea and/or edema) plotted against concurrent levels of NT-proBNP, BNP, C-type natriuretic peptide, adrenomedullin, and endothelin 1 levels. R values are given with 95% CIs. Peptide levels were also significantly related to jugular venous pressure (measured by standard clinical technique as the distance of the highest excursion of internal jugular venous waves in centimeters above the sternal angle with torso at 45° and legs horizontal) in those with heart failure (R⫽0.309, n⫽72, P⫽0.008) but not in those without (R⫽0.05, n⫽222, P⫽0.495). Urocortin was related to left ventricular dimensions and function. Correlations with left ventricular end-diastolic dimension, left ventricular end-systolic dimension, fractional shortening, and LVEF were significant (R⫽0.190, 0.228, ⫺0.291, and ⫺0.187, respectively with sample number varying between 212 for calculated left ventricular mass to 259 for left ventricular end-diastolic dimension and corresponding P values varying between 0.002 and ⬍0.0001). R values tended Variable Significance (P ) 0.005 ⬍0.001 MI indicates myocardical infraction; GFR, glomerular filtration rate. to strengthen when analyses was confined to the 74 patients with heart failure (R⫽0.192, 0.266, ⫺0.313 and ⫺0.238, respectively) and lost significance when only the 255 patients without heart failure were considered (P⬎0.05 for all). Significant positive relationships were observed between plasma urocortin 1 levels and levels of the other neurohormones measured, including ANP, NT-proANP, BNP, NTproBNP, C-type natriuretic peptide, adrenomedullin, and endothelin 1 (R values varying between 0.210 for endothelin 1 and 0.398 for C-type natriuretic peptide levels, sample size varying between 286 and 298 with P values ⬍0.0001 for all relationships; Figure 2). An inverse relationship with renal function was observed. Urocortin was directly related to plasma creatinine (R⫽0.249, n⫽294, P⬍0.0001) and inversely related to estimated glomerular filtration rate (R⫽⫺0.107, n⫽286, P⫽0.072). By multiple linear regression analysis, only gender (P⬍0.0001), NT-proBNP levels (P⫽0.002), and a diagnosis of heart failure (P⫽0.034) remained independently predictive of increased plasma urocortin levels (R2⫽0.16). Other variables, which were significantly associated in univariate analysis but not in this multivariate analysis included plasma creatinine, all neurohormones with the exception of NT-proBNP, and the different measures of cardiac function. With respect to predictors of heart failure, univariate relationships were observed for fractional shortening, creatinine clearance, NT-proBNP, and plasma urocortin 1. By multivariate analysis, using stepwise multiple logistic regression, urocortin remained an independent predictor of heart failure (P⫽0.005 Table 3) independent of age, history of previous myocardial infarction, diabetes, LVEF, NTproBNP, and calculated creatinine clearance. The likelihood of a final diagnosis of heart failure rose from 15% to 20% to 39% in first, second, and third tertiles of plasma urocortin 1, respectively. In comparison, for tertiles of plasma NT-proBNP the corresponding figure were 5%, 12%, and 58%. In patients falling within both the lowest tertile of urocortin 1 and the lowest tertile of NT-proBNP, 5% had heart failure. Conversely, in those in the upper tertile plasma concentrations of both peptides, the risk of heart failure was 75% and 49% of all patients with heart failure fell within this subgroup (Figure 3). Wright et al 60 469 1.00 36 .75 Urocortin I (tertiles) 10 11 40 Low Mid High 7 20 3 2 2 Sensitivity Heart Failure Patients (%) 80 Plasma Urocortin 1 in Human Heart Failure Reference Line .25 2 1 0.00 0 0.00 Downloaded from http://circheartfailure.ahajournals.org/ by guest on May 2, 2017 Low n=100 NTproBNP Urocortin 1 .50 Mid n=101 High n=98 NT-proBNP (tertiles) Figure 3. Distribution of patients with heart failure (n⫽74) according to tertiles (low, mid, and high) of plasma NT-proBNP and urocortin 1 levels derived from the total study group (n⫽299). Forty-nine percent (36/74) of patients with a final diagnosis of heart failure exhibit upper tertile levels of both peptides. Urocortin 1 and NT-proBNP were assessed for their ability to predict the presence or absence of heart failure by receiver operating characteristic analysis. Urocortin 1 yielded an area under the curve (AUC) of 0.68 (95% CI, 0.61 to 0.75, P⬍0.001). The best-performing value of urocortin 1 (12.3 pmol/L) was associated with sensitivity, specificity, and positive and negative predictive values of 61%, 67%, 38%, and 84%, respectively. This was clearly a weaker performance than that observed for NT-proBNP with an AUC of 0.85 (95% CI, 0.80 to 0.90, P⬍0.0001), sensitivity of 80%, specificity of 81%, positive predictive value of 58%, and negative predictive value of 93%. Area under the receiver operating characteristic was significantly less for urocortin 1 when compared with NT-proBNP (P⬍0.01; Figure 4). Discussion In patients with a final diagnosis of heart failure, plasma urocortin levels were double those in the normal reference range population. Symptomatic patients without a final diagnosis of heart failure also had elevated urocortin at intermediate levels ⬇50% higher than those observed in the normal range. Plasma urocortin levels were related to symptoms (NYHA class), signs (jugular venous pressure), concurrent levels of other neurohormones known to be activated in heart failure, and echocardiographic measures of cardiac dimensions and function. Urocortin was independently predictive of heart failure. Urocortin 1 is clearly not as powerful a stand-alone indicator of cardiac function or as good a marker of the presence of heart failure as the natriuretic peptides (Figure 4). However, it does add additional and independent information beyond that offered by established predictors as reflected in our multivariable analysis. Intuitively, this is best appreciated from our tertile analysis (Figure 3). When NT- .25 .50 .75 1.00 1 - Specificity Figure 4. Receiver operating characteristic, AUC (95% CI) for discrimination of heart failure by urocortin 1 (AUC, 0.68; [0.61 to 0.75]) and NT-proBNP (AUC, 0.87; [0.82 to 0.92[). AUCs differed significantly (P⬍0.001). proBNP results were considered alone plasma levels in the upper tertile carried a 58% chance of a final diagnosis of heart failure; when both NT-proBNP and urocortin levels fell in the upper tertile the likelihood rose to 75% and half of all patients with heart failure exhibited top tertile levels for both peptides. Even in symptomatic patients without heart failure, urocortin 1 was increased above normal. The reasons for this are uncertain, but it is possible a burden of cardiovascular disease within the non– heart failure study group produced increased urocortin 1 at an intermediate level between truly healthy subjects and those with symptomatic or overt heart failure. Furthermore, urocortin may also be stimulated by noncardiovascular illness. The stimulation of urocortin secretion in vitro by interleukin-1, interleukin-6, and tumor necrosis factor-␣21 raises the possibility that an array of inflammatory states, with attendant cytokine activation, may result in some increase in plasma urocortin 1. Notably, the R2 value (0.16) from the multivariate model assessing independent determinants of plasma urocortin 1 only reflects 16% of the interindividual variation in plasma urocortin 1 levels. This suggests other factors, which influence plasma urocortin1 levels remain to be found. Further studies in health and disease should establish the spectrum of stimuli, which trigger increases in circulating urocortin 1. Ng et al24 have also reported elevated levels of urocortin in heart failure. In contrast to this previous report, we observed an inverse relationship with LVEF rather than the positive correlation reported previously. In addition, we observed a continuous increase in plasma urocortin levels across NYHA functional classes I to IV in contradistinction to the report from Ng et al in which levels seem to peak in NYHA classes I and II and were somewhat less in the NYHA classes III and IV. We observed no relationship with age rather than the inverse relationship reported previously.24 From this data set, it is not possible to determine why our results differ from the previous report in such clear-cut fashion. Answers may lie within the differing characteristics 470 Circ Heart Fail September 2009 Downloaded from http://circheartfailure.ahajournals.org/ by guest on May 2, 2017 of the 2 immunoassays used. They are likely to detect differing epitopes and/or partial degradation products of urocortin. The potential effects of corticotrophin binding protein on assay performance may also differ between assays. The assay used in this report exhibits no significant crossreactivity with relevant alternative peptides and has been fully validated.31 Notably, in this report, plasma urocortin levels follow the common pattern of neurohormones known to be activated in heart failure. That is, they increase with increasing severity of symptoms and cardiac dysfunction and rise in parallel with other neurohormonal markers including the natriuretic peptides, adrenomedullin, and endothelin 1. Clearly, further corroborating data are required. In contrast to the cardiac peptides, plasma urocortin 1 is higher in men than in women. This pattern was apparent in the symptomatic cohort overall and in age and gender matched healthy subjects. The underlying reasons for the gender difference are unknown. Levels of urocortin are also mildly inversely related to renal function by univariate analysis, although in multivariate tests, this relationship to creatinine clearance was not independent of other predictors of elevated urocortin 1. In summary, plasma urocortin 1 levels are elevated in human heart failure with significant positive relationships to other circulating neurohormones known to be activated in this condition. They are also related to symptoms, signs (ie, jugular venous pressure), and echocardiographic measures of cardiac structure and function. In contradistinction to a previous report,24 we found an inverse rather than positive relationship to LVEF. In addition, the relationship between urocortin 1 and symptomatic status was continuous with levels showing a continuous increment between NYHA classes I–IV. Our findings suggest that plasma urocortin levels are unlikely to assume a role as a diagnostic marker in heart failure. However, they do add to our overall understanding of the pathophysiological response to heart failure. In experimental heart failure, deliberate antagonism of endogenous urocortins clearly exacerbates hemodynamic, neurohormonal, and renal impairment.3 Taken together with previous studies defining the bioactivity of the urocortins in experimental heart failure,1–5 it seems likely that elevated plasma urocortin 1 in human heart failure reflects a beneficial compensatory response to this condition. Sources of Funding Support for this work was provided by the Health Research Council of New Zealand and the National Heart Foundation of New Zealand. Marguerite Hunter provided secretarial support. Disclosures Dr Richards holds the National Heart Foundation of New Zealand Chair of Cardiovascular Studies. References 1. Rademaker MT, Charles CJ, Espiner EA, Fisher S, Frampton CM, Kirkpatrick CMJ, Lainchbury JG, Nicholls MG, Richards AM, Vale WW. Beneficial hemodynamic, endocrine, and renal effects of urocortin in experimental heart failure: comparison with normal sheep. J Am Coll Cardiol. 2002;40:1495–1505. 2. Rademaker MT, Cameron VA, Charles CJ, Richards AM. Integrated hemodynamic, hormonal, and renal actions of urocortin 2 in normal and paced sheep: beneficial effects in heart failure. Circulation. 2005;112: 3624 –3632. 3. Rademaker MT, Charles CJ, Espiner EA, Frampton CM, Lainchbury JG, Richards AM. Endogenous urocortins reduce vascular tone and renin-aldosterone/endothelin activity in experimental heart failure. Eur Heart J. 2005;26:2046 –2054. 4. Rademaker MT, Charles CJ, Espiner EA, Frampton CM, Lainchbury JG, Richards AM. Four-day urocortin-I administration has sustained beneficial haemodynamic, hormonal, and renal effects in experimental heart failure. Eur Heart J. 2005;26:2055–2062. 5. Rademaker MT, Charles CJ, Richards AM. Urocortin 1 administration from onset of rapid left ventricular pacing represses progression to overt heart failure. Am J Physiol Heart Circ Physiol. 2007;293:H1536 –H1544. 6. Davis ME, Pemberton CJ, Yandle TG, Lainchbury JG, Rademaker MT, Nicholls MG, Frampton CM, Richards AM. Effect of urocortin-1 infusion in humans with stable congestive cardiac failure. Clin Sci. 2005;109: 381–388. 7. Davis ME, Pemberton CJ, Yandle TG, Fisher SF, Lainchbury JG, Frampton CM, Rademaker MT, Richards M. Urocortin 2 infusion in human heart failure. Eur Heart J. 2007;28:2589 –2597. 8. Brar BK, Jonassen AK, Egorina EM, Chen A, Negro A, Perrin MH, Mjos OD, Latchman DS, Lee K-F, Vale W. Urocortin-II and urocortin-III are cardioprotective against ischemia reperfusion injury: an essential endogenous cardioprotective role for corticotropin releasing factor receptor type 2 in the murine heart. Endocrinology. 2004;145:24 –35. 9. Chang CL, Hsu SYT. Ancient evolution of stress-regulating peptides in vertebrates. Peptides. 2004;25:1681–1688. 10. Vaughan J, Donaldson C, Bittencourt J, Perrin MH, Lewis K, Sutton S, Chan R, Turnbull AV, Lovejoy D, Rivier C, Rivier J, Sawchenko PE, Vale W. Urocortin, a mammalian neuropeptide related to fish urotensin I and to corticotropin-releasing factor. Nature. 1995;378:287–292. 11. Hsu SY, Hsueh AJW. Human stresscopin and stresscopin-related peptide are selective ligands for the type 2 corticotropin-releasing hormone receptor. Nat Med. 2001;7:605– 611. 12. Imaki T, Katsumata H, Miyata M, Naruse M, Imaki J, Minami S. Expression of corticotropin releasing factor (CRF), urocortin and CRF type 1 receptors in hypothalamic-hypophyseal systems under osmotic stimulation. J Neuroendocrinol. 2001;13:328 –338. 13. Lewis K, Li C, Perrin MH, Blount A, Kunitake K, Donaldson C, Vaughan J, Reyes TM, Gulyas J, Fischer W, Bilezikjian L, Rivier J, Sawchenko PE, Vale WW. Identification of urocortin III, an additional member of the corticotropin-releasing factor (CRF) family with high affinity for the CRF2 receptor. Proc Natl Acad Sci USA. 2001;98:7570 –7575. 14. Scarabelli T, Knight R. Urocortins: take them to heart. Curr Med Chem Cardiovasc Hematol Agents. 2004;2:335–342. 15. Eckart K, Radulovic J, Radulovic M, Jahn O, Blank T, Stiedl O, Spiess J. Actions of CRF and its analogs. Curr Med Chem. 1999;6:1035–1053. 16. Iino K, Sasano H, Oki Y, Andoh N, Shin R-W, Kitamoto T, Takahashi K, Suzuki H, Tezuka F, Yoshimi T, Nagura H. Urocortin expression in the human central nervous system. Clin Endocrinol. 1999;50:107–114. 17. Muramatsu Y, Fukushima K, Iino K, Totsune K, Takahashi K, Suzuki T, Hirasawa G, Takeyama J, Ito M, Nose M, Tashiro A, Hongo M, Oki Y, Nagura H, Sasano H. Urocortin and corticotropin-releasing factor receptor expression in the human colonic mucosa. Peptides. 2000;21: 1799 –1809. 18. Nishikimi T, Miyata A, Horio T, Yoshihara F, Nagaya N, Takishita S, Yutani C, Matsuo H, Matsuoka H, Kangawa K. Urocortin, a member of the corticotropin-releasing factor family, in normal and diseased heart. Am J Physiol Heart Circ Physiol. 2000;279:H3031–H3039. 19. Wiley KE, Davenport AP. CRF2 receptors are highly expressed in the human cardiovascular system and their cognate ligands urocortins 2 and 3 are potent vasodilators. Br J Pharmacol. 2004;143:508 –514. 20. Brar BK, Stephanou A, Okosi A, Lawrence KM, Knight RA, Marber MS, Latchman DS. CRH-like peptides protect cardiac myocytes from lethal ischaemic injury. Mol Cell Endocrinol. 1999;158:55– 63. 21. Ikeda K, Tojo K, Tokudome G, Hosoya T, Tajima N, Oki Y, Asaba K, Hashimoto K, Harade M, Nakao K. Urocortin is an endogenous cardioprotective factor against negative effects of cytokines in the heart. Abstract of Paper Presented at the Endocrine Society’s 83rd Annual Meeting, 2001. 22. Ikeda K, Tojo K, Tokudome G, Ohta M, Sugimoto K, Tamura T, Tajima N, Mochizuki S, Kawakami M, Hosoya T. Cardiac expression of urocortin (Ucn) in diseased heart; preliminary results on possible Wright et al 23. 24. 25. 26. 27. 28. Downloaded from http://circheartfailure.ahajournals.org/ by guest on May 2, 2017 29. 30. involvement of Ucn in pathophysiology of cardiac diseases. Mol Cell Biochem. 2003;252:25–32. Watanabe F, Oki Y, Ozawa M, Masuzawa M, Iwabuchi M, Yoshimi T, Nishiguchi T, Iino K, Sasano H. Urocortin in human placenta and maternal plasma. Peptides. 1999;20:205–209. Ng LL, Loke IW, O’Brien RJ, Squire IB, Davies JE. Plasma urocortin in human systolic heart failure. Clin Sci. 2004;106:383–388. Behan DP, De Souza EB, Lowry PJ, Potter E, Sawchenko P, Vale WW. Corticotropin releasing factor (CRF) binding protein: a novel regulator of CRF and related peptides. Front Neuroendocrinol. 1995;16:362–382. Seasholtz AF, Valverde RA, Denver RJ. Corticotropin-releasing hormone-binding protein: biochemistry and function from fishes to mammals. J Endocrinol. 2002;175:89 –97. Wright SP, Doughty RN, Pearl A, Gamble GD, Whalley GA, Walsh HJ, Gordon G, Bagg W, Oxenham H, Yandle T, Richards M, Sharpe N. Plasma amino-terminal pro-brain natriuretic peptide and accuracy of heart-failure diagnosis in primary care: A randomized, controlled trial. J Am Coll Cardiol. 2003;42:1793–1800. Guidelines for the diagnosis of heart failure. The Task Force on Heart Failure of the European Society of Cardiology. Eur Heart J. 1995;16: 741–751. Cowie MR, Struthers AD, Wood DA, Coats AJS, Thompson SG, PooleWilson PA, Sutton GC. Value of natriuretic peptides in assessment of patients with possible new heart failure in primary care. The Lancet. 1997;350:1349 –1353. Maisel AS, Krishnaswamy P, Nowak RM, McCord J, Hollander JE, Duc P, Omland T, Storrow AB, Abraham WT, Wu AHB, Clopton P, Steg PG, Westheim A, Knudsen CW, Perez A, Kazanegra R, Herrmann HC, McCullough PA; the Breathing Not Properly Multinational Study Inves- Plasma Urocortin 1 in Human Heart Failure 31. 32. 33. 34. 35. 36. 37. 38. 471 tigators. Rapid measurement of B-type natriuretic peptide in the emergency diagnosis of heart failure. N Engl J Med. 2002;347:161–167. Davis ME, Pemberton CJ, Yandle TG, Lainchbury JG, Rademaker MT, Nicholls MG, Frampton CM, Richards AM. Urocortin-1 infusion in normal humans. J Clin Endocrinol Metab. 2004;89:1402–1409. Hunt P, Richards A, Nicholls M, Yandle T, Doughty R, Espiner E. Immunoreactive amino-terminal pro-brain natriuretic peptide (NTPROBNP): a new marker of cardiac impairment. Clin Endocrinol. 1997; 47:287–296. Yandle TG, Richards AM, Gilbert A, Fisher S, Holmes S, Espiner EA. Assay of brain natriuretic peptide (BNP) in human plasma: evidence for high molecular weight BNP as a major plasma component in heart failure. J Clin Endocrinol Metab. 1993;76:832– 838. Yandle TG, Espiner EA, Nicholls MG, Duff H. Radioimmunoassay and characterization of atrial natriuretic peptide in human plasma. J Clin Endocrinol Metab. 1986;63:72–79. Prickett TCR, Yandle TG, Nicholls MG, Espiner EA, Richards AM. Identification of amino-terminal pro-c-type natriuretic peptide in human plasma. Biochem Biophys Res Commun. 2001;286:513–517. Lewis LK, Smith MW, Yandle TG, Richards AM, Nicholls MG. Adrenomedullin(1–52) measured in human plasma by radioimmunoassay: plasma concentration, adsorption, and storage. Clin Chem. 1998; 44:571–577. Kitamura K, Tanaka T, Kato J, Eto T, Tanaka K. Regional distribution of immunoreactive endothelin in porcine tissue: Abundance in inner medulla of kidney. Biochem Biophys Res Commun. 1989;161:348 –352. Hanley JA, McNeil BJ. A method of comparing the areas under receiver operating characteristic curves derived from the same cases. Radiology. 1983;148:839 – 843. Plasma Urocortin 1 in Human Heart Failure Sue P. Wright, Robert N. Doughty, Chris M. Frampton, Greg D. Gamble, Tim G. Yandle and A. Mark Richards Downloaded from http://circheartfailure.ahajournals.org/ by guest on May 2, 2017 Circ Heart Fail. 2009;2:465-471; originally published online July 8, 2009; doi: 10.1161/CIRCHEARTFAILURE.108.840207 Circulation: Heart Failure is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 2009 American Heart Association, Inc. All rights reserved. Print ISSN: 1941-3289. Online ISSN: 1941-3297 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circheartfailure.ahajournals.org/content/2/5/465 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation: Heart Failure can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation: Heart Failure is online at: http://circheartfailure.ahajournals.org//subscriptions/