Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Electrocardiography wikipedia , lookup
Heart failure wikipedia , lookup
Coronary artery disease wikipedia , lookup
Remote ischemic conditioning wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Myocardial infarction wikipedia , lookup
Cardiac surgery wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
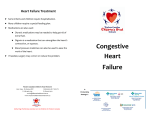
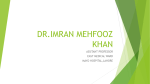
European Heart Journal (2004) 25, 952–962 Clinical research Is central nervous system processing altered in patients with heart failure? Stuart D. Rosena,b,*, Kevin Murphyc, Alexander P. Leffb, Vincent Cunninghamb, Richard J.S. Wiseb, Lewis Adamsc, Andrew J.S. Coatsa, Paolo G. Camicib a Department of Heart Function, National Heart and Lung Institute, Imperial College, Royal Brompton Hospital, London SW3 6NP, UK b MRC Clinical Sciences Centre, Imperial College, Hamersmith Hospital, London W12 OHS, UK c Department of Respiratory Physiology, National Heart and Lung Institute, Imperial College, Charing Cross Hospital, London W68RP, UK Received 13 April 2003; revised 11 March 2004; accepted 31 March 2004 Available online KEYWORDS Aims Breathlessness is a cardinal symptom of heart failure and the altered regulation of breathing is common. The contribution of abnormal central nervous system activity has not previously been investigated directly, although abnormal autonomic responses have been described. Our aim was to assess whether heart failure patients exhibit different patterns of regional brain activation after exercise stress. Methods We used positron emission tomography with H2 15 O, to measure changes in regional cerebral blood flow (rCBF) and absolute global cerebral blood flow (gCBF) in 6 male class II/III heart failure patients and 6 normal controls. Breathlessness (0–5 visual analogue scale) and respiratory parameters were measured at rest, after horizontal bicycle exercise and during isocapnic hyperventilation. CBF was measured in each condition in all subjects. Results Both groups were similarly breathless after exercise and the respiratory parameters were comparable. rCBF differences for the main comparison (exercise vs hyperventilation) were: activation of the right frontal medial gyrus (P < 0:001; Z ¼ 4:90) and left precentral gyrus (P < 0:03; Z ¼ 4:66) in controls but not in patients. Both groups had rCBF increases in the left anterior cingulate (P < 0:05; Z ¼ 4:67) and right dorsal cingulate cortex (P < 0:05; Z ¼ 4:66). The gCBF did not differ between exercise, isocapnic hyperventilation and rest in patients but, in controls, gCBF was greater after exercise compared to either isocapnic hyperventilation or rest. Conclusion Heart failure patients had a distinct pattern of regional cortical activity with exercise-induced breathlessness but unvarying CBF values between conditions. These central neural differences in activity may contribute to some features of heart failure, such as variability in symptoms and autonomic dysregulation. c 2004 The European Society of Cardiology. Published by Elsevier Ltd. All rights reserved. Heart failure; Breathlessness; Cerebral blood flow; Exercise; Brain; Autonomic nervous system; Positron emission tomography Introduction * Corresponding author. Tel.: þ44-208-967-5359; fax: þ44-208-9675007. E-mail address: [email protected] (S. D. Rosen). In health, the regulation of breathing and cardiac output is very closely co-ordinated, maximising the 0195-668X/$ - see front matter c 2004 The European Society of Cardiology. Published by Elsevier Ltd. All rights reserved. doi:10.1016/j.ehj.2004.03.025 Is central nervous system processing altered in patients with heart failure? 953 List of Abbreviations ANOVA ANS CHF CNS ECG fR gCBF PCO2 PET analysis of variance autonomic nervous system chronic heart failure central nervous system electrocardiogram respiratory frequency global cerebral blood flow partial pressure of carbon dioxide positron emission tomography efficiency of oxygen transfer to the body and delivery of oxygen at the tissue level. In cardiac or pulmonary disease, when cardiac output or oxygenation is abnormal, overall cardiopulmonary efficiency declines and the work of breathing is increased for the required oxygen delivery required. Both diseases are associated with breathlessness and fatigue, although the precise mechanisms involved probably differ somewhat between them.1;2 In heart failure, even when objective signs of pulmonary disease are absent, some patients display lower values of PCO2 and higher respiratory frequency (fRÞ .3 An altered ventilatory response to exercise (VE –VCO2 slope) has also been demonstrated and is an independent marker of prognosis.4–6 Dysregulation of breathing in chronic heart failure (CHF) might involve changes of control at several levels, ranging from peripheral ergoreflex activation7 and peripheral chemosensitivity,8 through abnormal autonomic reflexes9–11 to an altered central command.12 Furthermore, the relationship of these variables to the subjective sensation of breathlessness is elusive.2;13;14 The role of the central nervous system (CNS) in the regulation of breathing has been investigated in normal individuals using several technologies,15–24 including positron emission tomography (PET) with H2 15 O, one of the most direct means of exploring neural function in vivo in man.25–27 Regional cerebral blood flow (rCBF) is measured as an index of regional synaptic activity during particular tasks or conditions.28 Although several independent methods (e.g., analysis of heart rate variability10–11 ) have pointed to abnormalities of automatic nervous system (ANS) function in chronic heart failure (CHF), altered activity of the CNS has not been systematically investigated. Because known abnormalities of breathing regulation have been demonstrated by other techniques, we predicted that important functional abnormalities of CNS activity might occur in CHF. We also sought to clarify whether the wide variation in the experience of breathlessness, known to correlate poorly with objective measures of impairment of cardiac function,14 might be explicable in terms of differences in cerebral cortical activation. (We have previously demonstrated this comparing painful and silent myocardial ischaemia.29 ) The specific hypothesis that we tested in this study was that the pattern of CNS activation, during rCBF Sa O2 SPM VCO2 VE VE –VCO2 slope vs VT regional cerebral blood flow arterial oxygen saturation Statistical parametric mapping volume of CO2 exhaled minute ventilation ventilatory equivalent for CO2 versus tidal volume physical stress is different in patients with CHF from that in age-matched normal controls. Methods Study population Selection of heart failure patients Six dextral male patients [age 62 (11) years], mean (SD) were recruited from consecutive out-patients of Hammersmith and Charing Cross Hospitals over a period of 1.5 years. All were patients with symptomatic systolic CHF, New York Health Association (NYHA) class II or III, controlled on medication. The aetiology of the CHF was coronary artery disease with previous myocardial infarction in 5 cases and idiopathic dilated cardiomyopathy in 1 case. During exercise testing, 5/6 patients and all controls had ECGs that were amenable to the detection of ischaemia; one patient was in left bundle branch block. There was no detectable inducible ischaemia during exercise in the study population. Echocardiography was performed according to standard protocols to assess left ventricular function. Lung function tests were also performed to exclude asthma or chronic obstructive pulmonary disease. Diabetes and autonomic neuropathy were also excluded, the latter by standard bedside tests. In addition, subjects with unstable cardiovascular disease, drug or alcohol addiction and those who had already undergone a PET scan or any other study involving ionising radiation within the last two years were excluded. Patients with clinical evidence of cerebrovascular disease were also excluded. The 6 patients who satisfied the above criteria were the result of investigating over 40 patients with CHF during an 18-month period. The characteristics of the patient group are shown in Table 1. Control subjects Six dextral normal sedentary male controls [age 67 (5) years, P ¼ NS vs the patients] were also studied. These were selected on the basis that they were both age- and sex-matched with respect to the patients. They were recruited randomly from hospital staff, visitors and relatives of patients on the basis of reply to a general call for study volunteers. They all had clear past medical histories with no background of cardiac or pulmonary disease, or risk factors for coronary artery disease. They underwent the same detailed cardiopulmonary assessment as the patients and demonstrated normal results, i.e., normal resting and exercise ECGs, normal echocardiography and normal lung function. 954 Table 1 Characteristics of the patients and controls Patient Age Height Weight Cause Medication Echocardiogram 1 67 164 62 AMI 5 years S,A,D,AS 2 68 171 90 AMI 6 years N,D,B,S,AS,F,AL FS 26%; anteroseptal akin; NS inf hypokin FS 27% apical and inf infarcts Ex 20 years 3 54 168 63 AMI 1.5 years AS,A,D, Lithium 4 70 167 61 AMI 8 years AS,D,N,A 5 71 166 111 AMI 4 years A,Warfarin,N,D 6 45 185 84 DCM 4 years Dig,amio,D, Warfarin,S,A FS 15% Ant and inf infarcts; dil LA and LV FS 16%; ant, apical and infpost hypokin, apex akin FS 3%; septum akin; hypo through-out FS 23%; apical hypo Control Age Height Weight Echocardiogram Smoke ECG 1 2 3 4 64 60 66 72 156 167 180 163 65 66 84 70 No No No No Within Within Within Within 5 6 71 72 178 171 59 77 No WMA; FS 30% No WMA; FS 29% NS NS Ex 25 years 20/day for 56 years NS NS WMA; WMA; WMA; WMA; FS FS FS FS 33% 47% 29% 40% normal normal normal normal Smoke NS NS Ex 28 years 10 g/wk ECG Angiogram NYHA LBBB Negative maximal DSE Q V1-5; L-axis # ST I, aVL,V3-6 Poor R V1-3; nonspec # ST V5,6 Incomplete LBBB; " LA; Inferolat ST/T; VE’s Poor R V1-3; q in V4; # T V1-6, I, aVL # T inferolat; Q V1-3; VE’s 90% prox LAD; Cx and RCA II Occ LAD; 70%RCA; unobst Cx; Eff PCI-LAD Small unobst arteries II 80% mid LAD; Occ Cx after OM1; Occ RCA; 3 SVG’s and LIMA 90% LAD; 90% Cx; Occ RCA; LIMA to LAD; SVG’s: OM1 & RCA Not performed (Patient refused) II III III II limits limits limits limits Within normal limits Within normal limits Cause: AMI, acute myocardial infarction, number of years previously; DCM, dilated cardiomyopathy. Medication: S, statin; A, ACE-inhibitor; D, diuretic; AS, aspirin; N, nitrate; B, b-blocker; F, fibrate; AL, ablocker; Dig, digoxin; Amio, amiodarone. Echocardiogram ; FS, fractional shortening; ant, anterior; inf, inferior; infpost, inferoposterior; akin, akinesis; hypokin, hypokinesis; dil, dilated; LA, left atrium; LV, left ventricle; WMA, wall motion abnormality. Smoke: smoker status; Ex, ex-smoker; NS, non-smoker. ECG: LBBB, left bundle branch block; DSE, dobutamine stress echocardiogram; L-axis, left axis deviation; # ST, ST segment depression; " LA, left atrial enlargement; Nonspec, non-specific changes; Poor R, poor R wave development; ST/T, ST and T wave changes; VE’s, ventricular ectopic beats. Angiogram: LAD, left anterior descending coronary artery; Cx, left circumflex artery; RCA, right coronary artery; prox, proximal stenosis; Occ, occluded; Unobst, unobstructed; Ef, effective; PCI, percutaneous coronary intervention; OM1, first oblique marginal branch of circumflex; SVG, saphenous vein graft; LIMA, left internal mammary artery graft. NYHA: New York Heart Association heart failure class. S. D. Rosen et al. Is central nervous system processing altered in patients with heart failure? Monitoring and measurements Time 0 End list mode Exercise at 50W Peak of counts Unloaded exercise End infusion During the PET study, patients were monitored repeatedly using: a 12 lead ECG (Marquette), continuous ECG for rhythm (Siracust), blood pressure (Dinamap), respiratory flow rate (ultrasonic flowmeter), end-tidal PCO2 (Capnograph), arterial oxygen Count rise noted PET scanning protocol On a different day, patients and controls attended the MRC Clinical Sciences Centre/IRSL, Hammersmith Hospital for PET scanning. This was carried out using an ECAT EXACT3D tomograph (model 966, CTI, Knoxville, TN, USA).31;32 The acquisition system of this scanner has a flexible design which can record data in both frame and list mode. List mode acquisition was used in the present study, thus providing efficiency of data storage and high temporal sampling with flexible post-hoc frame re-binning. Emission scanning was performed with an energy window of 350–650 keV. Transmission scanning was performed with a single photon point source (150 MBq of 137 Cs, E ¼ 0:663 MeV, t1=2 ¼ 30:2 years), contained in a small pellet which was driven in a fluid-filled steel tube wound into a helix and positioned just inside the detector ring. A series of measurements of rCBF were carried out, using H2 15 O as the flow tracer. For each CBF measurement, 6 mCi activity of H2 15 O were administered as a bolus over 160 s, (build-up period of 120 s, infusion for 20 s and flush for 20 s).33 After cannulation of the radial artery and an antecubital vein, patients and controls underwent a series of 12 scans. These comprised 3 different conditions of rest, post-exercise breathlessness and isocapnic hyperventilation each repeated 4 times in a randomised sequence. The duration of each scan including the delay between scans was 8 min: For each 8-min cycle, when the run was bicycle exercise, there was unloaded exercise between t0 and 1.00 min, then 50W exercise between 1.00 and 4.00 min of the 8 min cycle. When the run was isocapnic ventilation, each subject breathed in time with a metronome at the same fR and VT as at the end of the bicycle exercise condition, between 3.00 and 7.30 min of the 8 min cycle. In all conditions, the H2 15 O build-up was between t ¼ 1:30 and t ¼ 3:30 min, the infusion between 3.30 and 4.30 min, with the rise noted on the PET camera between 4.20 and 4.25 min, peaking at 4.55 min (Fig. 1). The list mode acquisition was between 2.30 and 7.30 min. Scan acquisition was performed immediately on cessation of cycling because movement artefacts during cycling prevented the acquisition of useful data. During the scanning sequence, 200 mL of blood (5 mL/ min between 3.50 and 7.20 min of each cycle plus a discrete 5 mL sample at 6.50 min) was taken from each subject. During each PET scan, blood was sampled continuously from a radial arterial line for scintillation counting by an on-line bismuth germanium oxide system. This allowed the rCBF measurements to be quantified in absolute units (described below). In total, subjects had a radiation exposure of 3.54 mSv (12 runs, each equivalent to an exposure of 0.27 mSv, plus 0.3 mSv for the transmission scan). H215O infusion Prior to the PET scanning session, all subjects underwent clinical rehearsals at the Respiratory Physiology Laboratory, Charing Cross Hospital to learn how to use the horizontal exercise bicycle. They had a symptom-limited test during which, in addition to continuous ECG, their blood pressure, heart rate, ventilation (ultrasonic respiratory flowmeter), PCO2 (capnograph) and oxygen saturation (finger oximeter) was monitored. They also gave an estimate of their perceived breathlessness upon exertion using a modified Borg scale;30 in this case, a 0–5 scale (0 ¼ no sense of breathlessness, 5 ¼ intolerably severe breathlessness) with increments of 0.5. On a separate occasion, subjects were taught to copy the rate and depth of breathing that they had displayed during the practice horizontal bicycle test. This was to provide a control condition for the physical respiratory efforts associated with post-exercise breathlessness. However, to avoid hyperventilation-induced hypocapnia, we adjusted the amount of CO2 in the inspired gas mixture, to keep the PCO2 in the normal range. The condition was therefore termed ‘isocapnic hyperventilation’. From pilot work, we observed that isocapnic ventilation alone generated very little sensation of breathlessness. The idea was therefore that in the analysis of the scan data (described below), the exercise run, minus isocapnic ventilation, would equate to (physical effort of respiration + sensation of dyspnoea) ) (physical effort of respiration), i.e., as close as possible to a true representation of the sensation of dyspnoea. Start list mode Pre-scanning assessment Run 1 Isocapnic hyperventilation; Run 2 Rest 1; Run 3 Horizontal bicycle exercise; Run 4 Isocapnic hyperventilation; Run 5 Rest 2; Run 6 Horizontal bicycle exercise; [4 min break to download data from PET camera to computer] Run 7 Horizontal bicycle exercise; Run 8 Isocapnic hyperventilation; Run 9 Rest 3; Run 10 Rest 4; Run 11 Horizontal bicycle exercise; Run 12 Isocapnic hyperventilation. H215O build up Population size The sample size (6 patients and 6 controls) was chosen on the basis of several previous brain PET studies of this nature, in which this sample size was adequate to demonstrate significant differences in regional cerebral blood flow. 955 8 minutes Fig. 1 Acquisition schedule – post-exercise breathlessness. 956 S. D. Rosen et al. saturation – Sa O2 (finger oximeter), a modified Borg scale of perceived breathlessness and distress. Analysis of PET images PET images were transformed into a standard stereotactic space. Regional blood flow measurements were corrected for global changes in blood flow and comparisons of rCBF across conditions were performed with the t statistic (more precisely a block design ANCOVA) on a voxel by voxel basis by statistical parametric mapping (SPM96) software (Wellcome Department of Cognitive Neurology, Queen Square).34–37 rCBF changes related to the post-exercise breathlessness runs were compared with isocapnic hyperventilation runs as well as with baseline conditions. These analyses permitted the construction of statistical parametric maps for the description of significant changes in rCBF between the different test conditions. Significant changes were identified by applying a statistical threshold of 0.05, corrected for multiple comparisons. For the computation of global cerebral blood flow (gCBF), arterial blood was sampled throughout the scanning procedure from the radial arterial line. gCBF measurements were obtained (mL blood/min/mL tissue) by means of least squares fits of total tissue radioactivity using the Kety model.38 Statistical evaluation Besides the use of SPM for the analysis of the rCBF data, the intra-group respiratory variables, between different conditions, were analysed with a 2 factor ANOVA (two-sided). However, due to concerns over possible correlations between the post-exercise data and the isocapnic hyperventilation data, we compared the respiratory variables between groups for the different conditions using two-tailed paired t tests. The t test was also used to compare age and echocardiographic fractional shortening between the study groups. The statistical comparisons were performed using Statview SE+ Graphicsâ 4.0 software. Statistical significance was defined as P < 0:05. Ethical considerations This study was approved by the Research Ethics Committee, Hammersmith Hospital and by the UK Administration of Radioactive Substances Advisory Committee (ARSAC). The investigation conformed with the principles outlined in the Declaration of Helsinki (Cardiovascular Research 1997;35:2–4). All subjects gave written informed consent for their participation in the study. Results Patient and control characteristics are presented in Table 1. The only co-morbid illnesses were two previous deep vein thromboses in patient 2 and diverticulosis in patient 5. No control had any intercurrent illness, nor was any taking medication. Lung function tests were within normal limits in all cases. The details of the respiratory parameters are in Tables 2–4. Respiratory parameters NB: Values of Sa O2 were above 96% in all subjects at all stages of testing and will therefore not be presented in greater detail. 1. At rest. There were no significant differences between the patients and controls for inspiratory and expiratory times and volumes, PCO2 , heart rate, fR or Vi at rest. (Table 2) 2. Isocapnic hyperventilation. The differences between isocapnic hyperventilation and rest for the two groups are detailed in the Table 3. As can be seen, there were no significant differences between the patients and controls for the respiratory variables during isocapnic hyperventilation. Table 2 Respiratory parameters under resting conditions Patient Ti Te PCO2 HR fR Vi 1 2 3 4 5 6 5.47 1.73 1.89 2.28 1.91 1.91 2.39 1.44 2.82 2.17 4.87 1.57 27.11 29.72 25.90 29.51 34.91 35.34 75.4 101.0 59.0 85.0 49.0 66.1 7.92 19.07 13.60 13.59 8.91 17.47 9.18 13.27 12.66 7.06 9.52 8.89 Mean P (vs Con) 2.53 ± 1.45 0.769 2.54 ± 1.25 0.781 30.41 ± 3.93 0.622 72.58 ± 18.72 0.25 13.42 ± 4.45 0.887 10.10 ± 2.39 0.988 Control Ti Te PCO2 HR fR Vi 1 2 3 4 5 6 2.47 2.71 1.91 2.74 2.07 2.18 2.34 2.86 1.53 2.58 2.42 2.61 37.38 30.86 29.16 31.58 25.05 35.87 59.25 59.5 50.5 53.5 80.5 68.5 12.57 11.14 17.46 11.28 13.51 12.79 8.26 10.00 8.02 9.69 15.18 9.55 Mean 2.35 ± 0.38 2.39 ± 0.51 31.65 ± 3.93 61.96 ± 10.98 13.13 ± 2.57 10.12 ± 2.73 Ti , inspiratory time (s); Te , expiratory time (s); PCO2 , end tidal partial pressure of CO2 (mmHg); HR (beats min1 ); fR respiratory frequency (min1 ); Vi , ventilation, i.e. expiratory volume fR (L min1 ); Con, Control subjects. Is central nervous system processing altered in patients with heart failure? 957 Table 3 Respiratory parameters during isocapnic hyperventilation Patient Ti Te PCO2 HR fR Vi 1 2 3 4 5 6 1.52 1.65 1.78 1.53 2.12 0.99 1.66 0.94 2.18 1.72 1.91 1.18 32.60 31.35 39.32 41.26 29.51 34.59 87.74 90 62 81 51 73.28 19.02 23.63 15.59 18.43 15.40 27.72 34.71 23.13 21.22 15.56 29.10 30.65 Mean P (vs Rest) P (vs Con) 1.60 ± 0.42 0.198 0.515 1.60 ± 0.37 0.068 0.353 34.77 ± 4.82 0.204 0.190 74.35 ± 15.28 0.657 0.165 19.97 ± 5.01 0.006 0.298 25.73 ± 7.72 0.004 0.939 Control Ti Te PCO2 HR fR Vi 1 2 3 4 5 6 1.62 1.40 1.98 1.60 2.02 1.72 1.53 1.54 1.67 1.50 2.02 3.43 39.41 36.81 38.96 35.73 36.99 37.35 63.25 58.75 48.5 55 77.25 68.25 19.02 21.88 16.47 19.47 15.00 11.71 28.08 29.95 14.85 43.51 14.71 25.73 Mean P (vs Rest) 1.72 ± 0.24 0.044 1.95 ± 0.75 0.237 37.54 ± 1.39 0.019 61.83 ± 10.15 0.910 17.26 ± 3.63 0.010 26.14 ± 10.75 0.021 For legend, see Table 2, plus: IH, isocapnic hyperventilation. Table 4 Respiratory parameters during post-exercise breathlessness Patient Ti Te PCO2 HR fR Vi 1 2 3 4 5 6 2.27 1.22 1.23 1.78 2.63 1.46 2.36 1.30 2.47 1.77 2.28 1.97 32.75 32.56 33.71 41.08 30.24 34.59 98.63 126.75 77.33 135.5 66.25 71.21 13.25 23.87 16.59 17.02 12.30 27.72 25.41 16.84 19.42 13.49 17.30 30.65 Mean P (vs Rest) P (vs IH) P (vs Con) 1.76 ± 0.58 0.257 0.573 0.527 2.02 ± 0.44 0.360 0.133 0.236 33.39 ± 4.05 0.226 0.593 0.114 95.95 ± 29.53 0.194 0.140 0.686 16.99 ± 4.18 0.183 0.280 0.281 17.96 ± 4.15 0.002 0.042 0.719 Control Ti Te PCO2 HR fR Vi 1 2 3 4 5 6 2.19 1.46 1.49 2.51 1.57 2.63 2.06 1.89 1.91 3.55 2.22 3.02 38.46 35.42 33.06 38.76 35.30 39.62 96.75 81.75 91.33 67 104 101.50 14.25 17.91 17.72 9.97 16.18 10.80 14.54 21.19 16.57 12.84 17.74 20.14 Mean P (vs Rest) P (vs IH) 1.97 ± 0.54 0.183 0.314 2.44 ± 0.71 0.872 0.259 36.77 ± 2.01 0.036 0.531 90.39 ± 13.94 0.003 0.002 14.47 ± 3.41 0.445 0.202 17.17 ± 3.57 0.002 0.079 For legend, see Table 2. 3. Post-exercise breathlessness. There was a non-significant trend for PCO2 to be lower after exercise in patients (33.4 ± vs 36.8 ± mmHg; P ¼ 0:114, two-tailed). Otherwise, there were no significant differences between the groups for the respiratory parameters (see Table 4). Breathing is increased during exercise or hyperventilation and, as expected, the comparisons in Tables 2–4 reflect this. Comparing post-exercise breathlessness to isocapnic hyperventilation, no differences between groups for the respiratory variables and heart rate were apparent (2tailed, paired t test), although there were differences in these variables between the conditions (P ¼ 0:042 for patients for Vi , and 0.002 for HR for controls]. No significant differences were found when testing for an interaction between these comparisons (CHF vs Controls 958 S. D. Rosen et al. There were significant rCBF increases in common for the patient and control groups with respect to the right lentiform nucleus (28, 12, 4; Z ¼ 6:01; P ¼ 0:000 and 38, )6, 6; Z ¼ 5:45; P ¼ 0:001) and left cerebellum ()32, )54, )40; Z ¼ 4:92; P ¼ 0:015) (see Table 6). 3. Post-exercise breathlessness vs isocapnic hyperventilation. NB: This equates to {physical effort of respiration + sensation of dyspnoea} compared to the physical effort of respiration alone. This main comparison identified the following areas of brain activation to be common to both patients and controls: the left anterior cingulate gyrus ()28, 32, 10; Z ¼ 4:67; P ¼ 0:043), and the right dorsal cingulate (18, )54, 26; Z ¼ 4:66; P ¼ 0:045). However, when patients and controls were compared directly, the control group exhibited increased rCBF in the right frontal medial gyrus (BA6; 2, )24, 64; Z ¼ 4:9; P ¼ 0:01) and the left pre-central gyrus (BA4; )18, 26, 62; Z ¼ 4:66; P ¼ 0:028), activations which were not found in the patient group. See Fig. 2. 4. Absolute cerebral blood flow in the test conditions. In the patients, there were no significant differences in gCBF among the study conditions (0.51 ± 0.07 mL/min/mL after exercise; 0.51 ± 0.10 mL/min/mL during isocapnic hyperventilation and 0.49 ± 0.09 mL/ min/mL at rest, P ¼ 0:89). In the controls, gCBF was greater after exercise than after isocapnic hyperventilation (0.40 ± 0.24 mL/min/mL vs 0.35 ± 0.03 mL/min/ mL; P < 0:0001) and greater after exercise than at rest (0.40 ± 0.24 mL/min/mL vs 0.35 ± 0.04 mL/min/mL; P < 0:0001). There were no differences between the and Post-exercise breathlessness vs isocapnic hyperventilation). For details, see Table 4. Perception of breathlessness There were no significant differences in the perception of breathlessness between the patients and controls within the test conditions. Both groups felt more breathless during exercise compared to resting conditions (1.99 ± 0.48 vs 0.13 ± 0.16 P ¼ 0:0002, for patients and 1.29 ± 1.14 vs 0.25 ± 0.61, P ¼ 0:03 for controls). Both groups also felt more breathless after exercise compared to during isocapnic hyperventilation (1.99 ± 0.48 vs 0.33 ± 0.35, P ¼ 0:0004, for patients and 1.29 ± 1.14 vs 0.29 ± 0.48, P ¼ 0:039 for controls). For both groups on 2 way ANOVA, post-exercise breathlessness vs isocapnic hyperventilation, P < 0:001. PET findings 1. Post-exercise breathlessness vs rest. NB: This equates to: {physical effort of respiration + sensation of dyspnoea} compared to rest. Areas of the brain activated in this comparison, in both patients and controls, were the right inferior temporal gyrus (BA 20; 60, )28, )22; Z ¼ 5:53; P ¼ 0:001) and the right anterior insula (BA 45; 26, 14, 2; Z ¼ 4:91; P ¼ 0:016). There were no significant areas of activation found in patients that were not found in controls, nor vice versa (see Table 5). 2. Isocapnic hyperventilation vs rest. NB: This equates to the physical effort of respiration compared to rest. Table 5 Areas of increase in rCBF in controls only for the comparison (post exercise breathlessness vs rest) LEFT RIGHT Area x y z Z P Insula/frontal op (BA 38) Cerebellum Cerebellum (vermis) Pre-central gyrus (BA 4) Post-central gyrus Fusiform gyrus )28 )32 )8 )4 14 )64 )56 )26 12 )36 )24 78 5.40 5.33 5.20 4.95 0.001 0.001 0.003 0.008 x Y z Z P 34 )64 )28 4.75 0.019 20 64 34 )24 )20 )64 84 )24 )28 5.13 4.87 4.75 0.004 0.011 0.019 Table 5 reports the co-ordinates in the x, y and z axes of the significant rCBF increases for the controls only, for the Comparison {post-exercise breathlessness ) rest} with reference to the stereotactic space defined by the atlas of Talairach and Tournoux.36 Statistical magnitudes are expressed as Z scores (Z) and P values. BA, Brodmann Area, frontal op, frontal operculum. Table 6 Areas of increase in rCBF, in controls only for the comparison: (isocapnic hyperventilation vs rest) LEFT RIGHT Area x y z Z P x Z P Pre-central gyrus (BA 6) Lentiform nucleus Cerebellum Inf parietal lobule (BA 40) )60 )26 )10 0 )2 )58 18 6 )22 6.30 5.55 6.02 0.000 0.000 0.000 68 y 2 z 12 5.22 0.002 20 66 )70 )42 )24 46 5.56 5.43 0.000 0.001 Table 6 reports the co-ordinates in the x, y and z axes, of the significant rCBF increases for the controls only, for the comparison {isocapnic hyperventilation ) rest} with reference to the stereotactic space defined by the atlas of Talairach and Tournoux.36 Statistical magnitudes are expressed as Z scores (Z) and P values. BA, Brodmann Area; Inf, inferior. Is central nervous system processing altered in patients with heart failure? 959 Abnormalities of respiratory function in heart failure Impaired ventilatory efficiency (altered VE –VCO2 slope)4–6 is an acknowledged feature of CHF patients and may have a number of causes including central factors (e.g., chemoreceptor stimulation by hypoxia, hypercapnia or acidosis)8 and peripheral ones.7 Our CHF patients showed a trend towards greater fR and lower PCO2 than the controls, although there were no statistically significant differences in the respiratory variables compared to controls. Perception of breathlessness in heart failure Fig. 2 Regional cerebral blood flow increases for the comparison {Post exercise breathlessness ) isocapnic hyperventilation} present in the controls but not in the CHF patients. The activation of the medial postcentral gyrus (I) and left superior frontal gyrus (II) in the controls is evident. R, right; L, left; Ant, anterior; Post, posterior. For the stereotactic co-ordinates, see text. isocapnic hyperventilation condition and at rest. Between patients and controls, there were significant differences (P < 0:00001) for each of the 3 conditions. Discussion Principal findings of the study We examined the central neural correlates of control of breathing in CHF and found: 1. The respiratory parameters were mostly comparable between the 2 groups for the different study conditions. However, during isocapnic hyperventilation and after exercise the patients tended to shorter breathing times, greater respiratory frequency and lower PCO2 ; 2. There was little subjective difference between the group of 6 Class II/III CHF patients and 6 age-matched sedentary controls; 3. There were areas of brain activation common to both groups – the right lentiform nucleus and left cerebellum in the isocapnic hyperventilation condition and the right inferior temporal gyrus and right anterior insula after exercise. For the main effect (exercise vs hyperventilation), a comparison which equates to {physical effort of respiration + sensation of dyspnoea} compared to physical effort of respiration alone, the controls showed activations not present in the patients, chiefly the medial post-central gyrus and left superior frontal gyrus; 4. Absolute gCBF did not differ significantly between the study conditions in the patient group but in controls it was significantly greater during post-exercise breathlessness than during either isocapnic hyperventilation or the resting condition. Breathlessness is a normal experience after excessive physical exertion and is more pronounced in the physically deconditioned. It is also a cardinal symptom of CHF, in which several mechanisms probably contribute to its generation.1;2 Although counter-intuitive, there is little or no relationship between symptoms of CHF and objective indices of function1;2;14 The issue is of obvious clinical importance, with a spectrum of symptoms ranging from excessive, causing debility in patients with wellpreserved organ function on the one hand, to lack of an important ‘early warning system’ in patients with significant pathology on the other. However, to date, the role of the CNS in generating such variability of symptom perception has not been studied directly. One of the motives to perform the present study was to address this. We attempted to identify if rCBF, in a particular cerebral area, co-varied with the subjective sensation of breathlessness in the CHF patients. No such area was identified. In fact there was less cerebral activation in the patients than in the controls, although both groups had similar subjective sensations of breathlessness. This subjective similarity may itself be considered rather surprising. Another situation in which reduced cortical activation is observed is in habituation of the response to an aversive stimulus.39;40 It could be conjectured that in CHF, there is habituation to afferent signals at some level within the neuraxis, which may be a factor in the complex relationship between symptoms and cardiac function in CHF. Concerning the sensation of post-exercise breathlessness, the lack of a difference between CHF patients and controls was rather unexpected. It is possible that the patients lacked a stimulus of sufficient intensity to generate additional foci of activation. However, even if this were the case, the subjective rating of breathlessness of the patients was not less than that of the controls and, furthermore, the haemodynamic responses were equivalent. Thus the principle negative finding of the study (the areas of brain activation found in controls but not patients) still appears to be a significant observation and one which requires explanation. Functional imaging of the brain in the study of respiratory control Functional imaging (mainly PET with H2 15 O) has previously been used in studies of breathing regulation in 960 normal subjects during volitional inspiration15 and expiration.16 Subsequently, CO2 -stimulated breathing has also been studied,18 with a control condition in the form of passive isocapnic respiration at equivalent fR and VT . Neuronal activation was identified in the upper brainstem, midbrain, hypothalamus, hippocampus, parahippocampus, fusiform gyrus, cingulate area, insula and frontal, temporo-occipital and parietal cortices. Although the main focus of that study was the motor control of breathing, the finding of substantial limbic system activation, is significant in the context of perception of breathlessness, because the CO2 inhalation produced a conscious urge to breathe that was often severe enough to be described as breathlessness. In a further investigation,17 the increase in breathing during and after right leg bicycle was explored. As well as demonstrating increases in rCBF in the ‘leg’ areas, there were also increases in the superolateral cortical areas bilaterally, previously noted to be activated during volitional breathing. After exercise, only the superolateral areas continued to show increased rCBF; in this study many of the subjects were feeling breathless during the image acquisition because of the high exercise workload. It should be emphasised however that, unlike the controls of our study, the subjects in these studies were mainly young, fit males with an understanding of respiratory physiology. More recently, Critchley et al., also using PET with H2 15 O, identified the central neural correlates of exercise and mental stress,41 demonstrating rCBF increases in the cerebellar vermis, right anterior cingulate and right insula which covaried with mean arterial pressure. rCBF increases were also found in the pons, cerebellum and right insula which co-varied with heart rate. Decreases in rCBF were reported for the pre-frontal and medial temporal regions. The areas identified were considered representative of the regions involved in integrated cardiovascular response patterns associated with volitional and emotional behaviours. With respect to the current study’s normal subjects, our principal findings are compatible with the above. We found left insular activation during post-exercise breathlessness; activation of this cerebral region was also a feature of Banzett et al., study of air hunger,20 it occurred in Corfield et al., study of CO2 -stimulated breathing18 and in Williamson’s study of hypnotic sense of effort.23 The cerebellar activation observed in our study corresponds to similar activations in studies of volitional inspiration by Ramsay et al.,16 and Colebatch et al.,15 the vermis activation also features in the studies of Pfeiffer on breathing against a resistive load21 and that of Isaev24 as well as in the Corfield et al., CO2 stimulated breathing study.18 The latter study and Williamson’s hypnotic sense of effort study also feature right anterior insular activation as found in our patients and controls.23 With respect to the isocapnic hyperventilation condition in our controls, the activations of the cerebellum and right superior frontal gyrus were also found in the studies of Ramsay,16 Corfield,18 Fink17 and colleagues. For our key comparison (post-exercise breathlessness vs S. D. Rosen et al. isocapnic hyperventilation) the left superior frontal activation in our controls corresponds to that found in Corfield’s CO2 study,18 whilst the left anterior cingulate activation, common to our patients and controls features in the studies of Fink,17 Williamson19;23 and Corfield.18 The most fascinating contrast in the present study, however, is the absence of distinguishing activations among the patients. The observation of no subjective difference in the perception of breathlessness between CHF patients and the controls suggests that the sensation of breathlessness may depend upon different brain mechanisms in CHF from those found in health. Alternatively, or additionally, there may be differences in central command in relation to exercise in CHF. Autonomic dysfunction in patients with heart failure Enhanced sympathetic activity is widely recognised as a pathophysiological feature of CHF. Several independent investigative techniques have pointed to abnormal neural regulation in CHF.10;11;42–47 In particular, an assortment of heart rate variability studies have indicated that at different stages of CHF, there are differences in the degree of alteration of neural regulation and the heart’s responsiveness to it. However, the precise neurophysiological substrate of such abnormalities, including any potential contribution of the higher centres of the CNS, remains to be elucidated. The present study is open and observational and its principal value lies in the proposition of hypotheses. It is possible that the apparent absence of cerebral activations in the different conditions in the CHF patients might be related to the reduced heart rate variability and baroreflex sensitivity known to occur in this disease. Unfortunately, we do not have specific data on heart rate variability and baroreflex sensitivity in these particular subjects, so any association remains speculative. It is tempting to hypothesise that one mechanism maintaining the degree of variability of these may be additional intermittent inputs from the cerebral cortex to the brainstem. A further prospective study with detailed autonomic functional assessment is necessary to clarify this. Cerebral vascular reactivity in heart failure Cerebral autoregulation is a fundamental physiological response to changes in systemic haemodynamic conditions and is well preserved in a wide range of conditions. However, a number of studies have demonstrated that cerebrovascular reactivity is attenuated in CHF. Paulson and colleagues, measuring cerebral blood flow (CBF) by the intracarotid xenon-133 (133 Xe) injection technique48 found mean CBF to be lower in patients with CHF. They also found that CBF was not reduced further by administration of captopril, despite a marked reduction in blood pressure. This effect was interpreted as a shift in the limits of cerebral autoregulation, probably mediated by larger cerebral arteries.49 More recently, Kamishirado et al., measuring CBF by analysing the Patlak-Plot curve obtained from radionuclide angiography, reported an Is central nervous system processing altered in patients with heart failure? increase in CBF in patients with CHF treated with enalapril, independent of any effect on cardiac output.50 Consistent with standard therapy for CHF, all but one of our patients in the present study were treated with ACEinhibitors and therefore the relatively greater values of gCBF that they had in all test conditions might be attributable to medical therapy. Other than treating all controls with an ACE-inhibitor, it is difficult to envisage how to remove this potentially confounding factor. However, this does not necessarily account for the lack of variability in gCBF in patients between conditions. With regard to rCBF in CHF, in a recent paper, a swine model of pacing-induced heart failure was described by Caparas et al.51 CBF was found to be reduced compared to controls both at rest and during treadmill exercise, although there was a significant increase in CBF between rest and exercise in the heart failure swine. Specific regions of blunted increase in perfusion were the parietal and occipital cortex and the supra-pyramidal medulla. To date, however, there have been no direct studies of rCBF in vivo in man in cardiac disease. We employed the technique of least squares fits of total tissue radioactivity using the Kety model.38 This was necessary because the SPM analysis treats gCBF as a co-variate of no interest, so only relative increases in rCBF between conditions can be identified. 961 4. It has to be acknowledged that there has been multiplicity of statistical testing, particularly of the respiratory data; in the presence of small sample sizes, there is therefore a disproportionate risk of false positive results. However, the respiratory data are only a secondary focus of the paper and the brain imaging data are more significant and less susceptible to eccentric outcomes. 5. It is possible that certain cerebral regions identified were only tangentially related to the conditions studied. Thus, we cannot exclude effects of mental counting during the isocapnic hyperventilation runs, in which subjects set their respiratory frequency to one initially derived from a metronome beat. The pre-central activations may be associated with this. 6. The lack of a real-time autonomic marker of cardiac dysfunction has caused difficulties in the analysis of data for this study. It is possible that the study was simply too focussed on the respiratory and neuroimaging aspects. No continuous ECG data, from which a useful measure of autonomic activity might have been made, were obtained. The authors hope to rectify this in subsequent work. 7. It must also be acknowledged that, certainly with respect to deductions made from the gCBF results, there is reliance in the present study on intra-group evaluations. Thus, in the absence of statistically significant differences, the implications of the observation must remain speculative. Limitations of the study 1. We did not find a significant difference in subjective breathlessness during exercise. This might be explained, at least in part, by the controls being (consistent with the demographics of heart failure) middleaged, deconditioned males rather than the more commonly studied young and fit individuals. The workload was also not very demanding. From the perspective of the participants however, the workload was considered ‘reasonable’ in terms of their activities of daily life; their indications were that they would not generally exert themselves beyond this level. This relatively low level of physical stress might have a bearing on the lack of significant differences among the respiratory variables. Furthermore, the number of patients studied is small, all were in NYHA classes II and III and all were probably ‘low perceivers’ in terms of their sensation of breathlessness. On the positive side, the eventual population was tightly characterised and matching was close between the controls and the patients. 2. It is certainly possible that widening of the age range and inclusion of female subjects would yield different results (we know, for example, that autonomic responses vary between sexes and age groups). A larger study would be desirable, but the study protocol was exacting. 3. In our quest for a ‘pure’ population of patients with breathlessness due to CHF, those with respiratory disease were excluded. Among these may have been some patients in whom impairment of lung function was a direct consequence of their cardiac disease, e.g., with bronchoconstriction provoked by an exercise-induced increase in end diastolic pressure. Conclusion We have investigated central neural activity in patients with CHF and in matched controls in conditions of postexercise breathlessness, rest and a control condition, isocapnic hyperventilation. Our principle finding is the absence of specific cerebral regional activations in heart failure patients, which are demonstrable in controls. As a consequence of this, it is suggested that, in heart failure, the perception of breathlessness and respiratory control may depend upon different brain mechanisms from those in health. We further noted a lack of significant change in absolute blood flow between conditions in patients and speculate that this might suggest a reduction in reactivity of the cerebral circulation. Such altered reactivity might contribute to the generation of symptoms and/or the autonomic dysfunction found in CHF. Acknowledgements This work was supported, in a large part, by the British Heart Foundation, through Dr. Rosen’s Intermediate Research Fellowship. References 1. Alexander RW. Dyspnea and fatigue. In: Schlant RC, Alexander RW, editors. The heart, arteries and veins. eighth ed. New York: McGrawHill; 1994. p. 469–74. 2. Coats AJS. What causes the symptoms of heart failure? Heart 2001;86:574–8. 962 3. Weber KT, Kinasewitz GT, Janicki JS et al. Oxygen utilisation and ventilation during exercise in patients with chronic heart failure. Circulation 1982;65:1213–23. 4. Buller NP, Poole-Wilson PA. Mechanism of the increased ventilatory response to exercise in patients with chronic heart failure. Br Heart J 1990;63:281–3. 5. Davies SW, Emery TM, Watlng MIL et al. A critical threshold of exercise capacity in the ventilatory response to exercise in heart failure. Br Heart J 1991;65:179–83. 6. Chua TP, Ponikowski P, Harrington D et al. Clinical correlates and prognostic significance of the ventilatory response to exercise in chronic heart failure. J Am Coll Cardiol 1997;29: 1585–90. 7. Clark AL, Poole-Wilson PA, Coats AJS. Exercise limitation in chronic heart failure: central role of the periphery. J Am Coll Cardiol 1996;28:1092–102. 8. Ponikowski P, Chua TP, Piepoli M et al. Augmented peripheral chemosensitivity as a potential input to baroreflex impairment and autonomic imbalance in chronic heart failure. Circulation 1997;96:2586–94. 9. Eckberg DL, Drabinsky M, Braunwald E. Defective cardiac parasympathetic control in patients with heart disease. N Engl J Med 1971;285:877–83. 10. Binkley PF, Nunziata E, Haas GJ et al. Parasympathetic withdrawal is an integral component of autonomic imbalance in congestive heart failure: demonstration in human subjects and verification in a paced canine model. J Am Coll Cardiol 1991;18:464–72. 11. Guzzetti S, Cogliati C, Turiel M et al. Sympathetic predominance followed by functional denervation in the progression of chronic heart failure. Eur Heart J 1995;16:1100–7. 12. Chua TP, Harrington D, Ponikowski P et al. Effects of dihydrocodeine on chemosensitivity and exercise tolerance in patients with chronic heart failure. J Am Coll Cardiol 1997;29:147–52. 13. Wilson JR, Rayos G, Yeoh TK et al. Dissociation between exertional symptoms and circulatory function in patients with heart failure. Circulation 1995;92:47–53. 14. Rihal CS, Nishimura RA, Hatle LK et al. Systolic and diastolic dysfunction in patients with clinical diagnosis of dilated cardiomyopathy. Relation to symptoms and prognosis. Circulation 1994;90:2772–9. 15. Colebatch JG, Adams L, Murphy K et al. Regional cerebral blood flow during volitional breathing in man. J Physiol 1991;443:91–103. 16. Ramsay SC, Adams L, Murphy K et al. Regional cerebral blood flow during volitional expiration in man: a comparison with volitional inspiration. J Physiol 1993;461:85–101. 17. Fink GR, Adams L, Watson JDG et al. Hyperpnoea during and immediately after exercise in man: evidence of motor cortical involvement. J Physiol 1995;489:663–75. 18. Corfield DR, Fink GR, Ramsay SC et al. Evidence for limbic system activation during CO2 -stimulated breathing in man. J Physiol 1995;488:77–84. 19. Williamson JW, McColl R, Mathews D et al. Activation of the insular cortex is affected by the intensity of exercise. J Appl Physiol 1999;87:1213–9. 20. Banzett RB, Mulnier HE, Murphy K et al. Breathlessness in humans activates insular cortex. Neuroreport 2000;11:2117–20. 21. Peiffer C, Poline JP, Thivard L et al. Neural substrates for the perception of acutely induced dyspnea. Am J Respir Crit Care Med 2001;163:951–7. 22. Harper RM. Visualization of neural activity associated with dyspnea. Am J Respir Crit Care Med 2001;163:805–6. 23. Williamson JW, McColl R, Mathews D et al. Hypnotic manipulation of effort sense during dynamic exercise: cardiovascular responses and brain activation. J Appl Physiol 2001;90:1392–9. 24. Isaev G, Murphy K, Guz A et al. Areas of the brain concerned with ventilatory load compensation in awake man. J Physiol 2002;539: 935–45. 25. Fox PT, Raichle ME, Mintun MA et al. Non-oxidative glucose consumption during focal physiologic neural activity. Science 1988;241:462–4. 26. Raichle M. Circulatory and metabolic correlates of brain function in normal humans. In: Mountcastle VB, Plum F, Geiger SR, editors. Handbook of physiology. Bethesda, MD, USA: American Physiological Society; 1987. p. 643–74. S. D. Rosen et al. 27. Mata M, Fink DG, Ganier H et al. Activity-dependent energy metabolism in rat posterior pituitary primarily reflects sodium pump activity. J Neurochem 1980;34:213–5. 28. Friston KJ, Frackowiak RSJ. Imaging functional anatomy. In: Lassen NA, Ingvar DH, Raichle ME, et al., editors. Brain work and mental activity, Vol 31. Copenhagen, Munksgaard: Alfred Benzon symposium; 1991. p. 267–79. 29. Rosen SD, Paulesu E, Nihoyannopoulos P et al. Silent ischaemia as a central problem: regional brain activation compared in silent and painful myocardial ischaemia. Ann Int Med 1996;124:939–49. 30. Borg GAV. Psychophysical bases of perceived exertion. Med Sci Sports Exerc 1982;14:377–81. 31. Jones WE, Vaigneur K, Young J et al. The architectural impact of single photon transmission measurements on full ring 3D positron emission tomography. IEEE Nuclear Science Symposium and Medical Imaging Conference Record 1995;2:1026–30. 32. Bailey DL, Miller MP, Spinks TJ et al. Experience with fully 3D PET and implications for future high resolution 3D tomographs. Phys Med Biol 1998;43:777–86. 33. Spinks TJ, Jones T, Bloomfield PM et al. Physical characteristics of the ECAT EXACT3D positron tomograph. Phys Med Biol 2000;45:2601–18. 34. Friston KJ, Frith CD, Liddle PF et al. The relationship between local and global changes in PET scans. J Cereb Blood Flow Metab 1990;10:458–66. 35. Friston KJ, Frith CD, Liddle PF et al. Comparing functional (PET) images: assessment of significant change. J Cereb Blood Flow Metab 1991;11:690–9. 36. Talairach J, Tournoux P. A co-planar stereotactic atlas of the human brain. Thieme: Stuttgart, FRG; 1988. 37. Friston KJ, Passingham RE, Nutt JG et al. Localisation in PET images: direct fitting of the intercommissural (AC-PC) line. J Cereb Blood Flow Metab 1989;9:690–5. 38. Kety SS. Measurement of local blood flow by the exchange of an inert, diffusible substance. Meth Med Res 1960;8:228–36. 39. Veit R, Flor H, Erb M et al. Brain circuits involved in emotional learning in antisocial behavior and social phobia in humans. Neurosci Lett 2002;328:233–6. 40. Schneider F, Weiss U, Kessler C et al. Subcortical correlates of differential classical conditioning of aversive emotional reactions in social phobia. Biol Psychiatr 1999;45:863–71. 41. Critchley HD, Corfield DR, Chandler MP et al. Cerebral correlates of autonomic cardiovascular arousal: a functional neuroimaging investigation in humans. J Physiol 2001;523:259–70. 42. Merlet P, Delforge J, Syrota A et al. Positron emission tomography with 11 C CGP-12177 to assess beta-adrenergic receptor concentration in idiopathic dilated cardiomyopathy. Circulation 1993;87:1169–78. 43. Kawai C, Yui Y, Hoshino T et al. Myocardial catecholamines in hypertrophic and dilated (congestive) cardiomyopathy: a biopsy study. J Am Coll Cardiol 1983;2:834–40. 44. La Rovere MT, Bigger Jr JT, Marcus FI et al. Baroreflex sensitivity and heart-rate variability in prediction of total cardiac mortality after myocardial infarction. Lancet 1998;351:478–84. 45. Cohn JN, Johnson GR, Shabetai R, et al. Ejection fraction, peak exercise oxygen consumption, cardiothoracic ratio, ventricular arrhythmias, and plasma norepinephrine as determinants of prognosis in heart failure. The V-HeFT VA Cooperative Studies Group. Circulation 1993;87(Suppl 6):VI5–16. 46. Rundqvist B, Eisenhofer G, Elam M et al. Attenuated cardiac sympathetic responsiveness during dynamic exercise in patients with heart failure. Circulation 1997;95:940–5. 47. Guzzetti S, Mezzetti S, Magatelli R et al. Linear and non-linear 24 h heart rate variability in chronic heart failure. Auton Neurosci Bas Clin 2000;86:114–9. 48. Paulson OB, Jarden OJ, Vorstrup S et al. Effect of captopril on the cerebral circulation in chronic heart failure. Eur J Clin Invest 1986;16:124–32. 49. Paulson OB, Waldemar G, Anderson AR et al. Role of angiotensin in autoregulation of cerebral blood flow. Circulation 1988;77:I55–8. 50. Kamishirado H, Inoue T, Fujito T et al. Effect of enalapril maleate on cerebral blood flow in patients with chronic heart failure. Angiology 1997;48:707–13. 51. Caparas SN, Clair MJ, Krombach RS et al. Brain blood flow patterns after the development of congestive heart failure: effects of treadmill exercise. Crit Care Med 2000;28:209–14.