Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
12-Hydroxyeicosatetraenoic acid wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
Innate immune system wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Immunosuppressive drug wikipedia , lookup
Inflammation wikipedia , lookup
Psychoneuroimmunology wikipedia , lookup
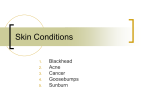
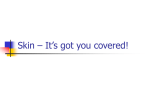
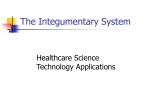
Inflammation & Cell Signaling 2015; 2: e737.doi: 10.14800/ics.737; © 2015 by G. Fabbrocini, et al. http://www.smartscitech.com/index.php/ics REVIEW Fragile Skin: Benefit of Cosmeceuticals based on Rhealba® Oat plantlet in acne vulgaris G. Fabbrocini1, M. Saint Aroman2, F. Schmitt3 1 Department of Dermatology and Venereology, University of Naples Federico II, 80100 Naples, Italy A-DERMA, Pierre Fabre Dermo-Cosmétique, 81500 Lavaur, France 3 A-DERMA, Pierre Fabre Dermo-Cosmétique, 81500 Lavaur, France 2 Correspondence: M. Saint Aroman E-mail: [email protected] Received: March 19, 2015 Published online: May 07, 2015 Fragile skin is the state of unbalanced skin characterized by lower resistance to aggressions linked with impaired barrier function of skin. Acneic skin becomes fragile due to its own pathophysiological mechanism. Indeed, acneic skin differs from normal skin as it is subject to higher transepidermal water loss and lower stratum corneum hydration. Moreover, acne vulgaris is also characterized by alterations in the lipid content of sebum and an inflammation in the sebaceous gland. These alterations lead to hyperproliferation and to an increased desquamation of keratinocytes within sebaceous follicles. Thus, the accumulation of keratinocytes can block the pilosebaceous unit, preventing sebum drainage. This results in the formation of microcomedones, and further acne lesions. Changes of the pilo-sebaceous environment favour the proliferation of Propionibacterium acnes (P. Acnes). P. acnes exerts several pro-inflammatory activities which trigger the innate immune system by activating toll-like receptor 2 and NLRP3-inflammasome, resulting in IL-1β secretion in human monocytes. Rhealba® Oat Plantlets extract (Pierre Fabre Dermo-Cosmetique) has been reported to restore fragile skin, inhibit bacterial adhesion of P. Acnes, and to be capable of reducing inflammation and irritation in acne. Moreover, cosmeceuticals including Rhealba® Oat Plantlets extract and hydro-compensating actives, which can be associated with anti-comedogenic agents (hydroxyl acids), may be usually used stand-alone or in addition to acne treatments in order to treat acne vulgaris. Keywords: Fragile skin; Acne vulgaris; Inflammasome; Toll Like Receptor; Rhealba® Oat To cite this article: G. Fabbrocini, et al. Fragile Skin: Benefit of Cosmeceuticals based on Rhealba® Oat plantlet in acne vulgaris.Inflamm Cell Signal 2015; 2: e737. doi: 10.14800/ics.737. disruption of the immune system, including innate immunity and adaptive immunity[1]. Introduction The most important function of the skin is to provide a protective barrier against external threats such as microorganisms, mechanical impacts, physical insults and chemicals. Fragile skin is the state of unbalanced skin characterized by lower resistance to aggressions linked with impaired barrier function of skin[1]. This impairment is characterized by an excessive water loss and a reduced capacitance. In addition, the ability to fend off potentially invasive microorganisms is also reduced in fragile skin by a Fragile skin can be categorized differently depending on its origin. Four categories were established: Firstly, the physiological fragile skin (age, location). Secondly, fragile skin can be the results of external and internal factors, like climate and stress. This type of fragile skin is therefore classified as circumstantial fragile skin. Then, the fragile skin caused by peeling or isotretinoin is referred to as iatrogenic Page 1 of 7 Inflammation&Cell Signaling 2015; 2: e737.doi: 10.14800/ics.737; © 2015 by G. Fabbrocini, et al. http://www.smartscitech.com/index.php/ics fragile skin. Finally, the pathological fragile skin is represented by atopic dermatitis and acne vulgaris[1]. Acne vulgaris is a chronic inflammatory skin disease of the pilosebaceous unit[2, 3]. The acne pathophysiology is multifactorial, with microbiological, immunological and hormonal mechanisms. Propionibacterium acnes (P. acnes), the predominant organism in the microbiome of facial skin, has been identified in acne lesions and induces inflammatory response and causes keratinocytes damage[4, 5]. These different mechanisms lead to inflammasome activation, and to an alteration of the epidermal barrier, and thus the acneic skin becomes fragile. Acne and epidermal barrier The epidermal barrier is represented by multiple physiologic activities occurring within the stratum corneum (SC). These activities include maintaining skin water content, protection against microbial organisms, protection from effects of ultraviolet radiations, neutralization of reactive oxygen species (ROS) and an immunologic role against exogenous allergens and haptens[6]. Changes in the epidermal barrier may participate or exacerbate the development of acne[1]. Acneic skin differs from normal skin because of higher transepidermal water loss (TEWL) and lower stratum corneum hydration (decreased conductance), responsible of skin dehydration[7]. The severity of acne appears to be correlated with the increase in transepidermal water loss and the decreased conductance[7, 8]. These impairments of the integrity of the skin barrier can cause an accumulation of corneocytes leading to skin thickening. This build-up of corneocytes may block the release of sebum from the pilosebaceous unit[1]. The hyperkeratosis of the follicular epithelium may result in the formation of comedone[8]. Furthermore, total ceramides (lipid rich matrix) and free sphingosine are significantly reduced. By causing hyperkeratosis, the deficiency of intercellular lipid may also contribute to the comedone formation[8]. Moreover, inflammation in the pilosebaceous unit can lead to the follicular wall rupture with subsequent leakage of sebum, bacteria and keratin into the dermis. This event is characterized by the occurrence of nodulocystic or nodular acne lesions[1]. Filaggrin is a fundamental protein in the differentiation of the epidermis and is involved in the functional and structural integrity of the stratum corneum[9]. Filaggrin support cytoskeletal aggregation and formation of the cornified cell envelope, providing additional strength and structure to epidermal barrier. Some skin diseases, and especially atopic dermatitis, are associated with the alteration of filaggrin expression, responsible for skin barrier impairment. However, in cultured keratinocytes and human skin explants, P. acnes causes an increase of filaggrin expression. Thereby, in acne lesions, the expression of filaggrins in keratinocytes lining the follicle wall is increased[10, 11]. Moreover, inflammatory cytokines have been reported to contribute to the overexpression of filaggrin in sebaceous gland explants[12]. These findings suggest that filaggrin expression would play a significant role in acne lesions formation. Another study on the filaggrin mutation in patients with xerosis comes consolidate these findings[13]. This study suggested that some patients may be protected against acne vulgaris whether they present one copy of a null mutation in the filaggrin gene. Nevertheless, a larger study specifically examining the presence of filaggrin null mutations in acne sufferers did not confirm these conclusions[14]. Actually, the filaggrin expression is linked with the differentiation of keratinocytes and alterations in the stratum corneum associated with acne lesion. Although in acne filaggrin expression seems to be augmented, in acne affected skin we curiously find different parameters typically associated with filaggrin function impairment: Yamamato et al. observed that patients with acne vulgaris exhibited markedly greater TEWL and lower skin hydration with an evident permeability barrier impairment. The decrease of skin hydration and increase of TEWL were higher in patients with acne vulgaris of moderate severity as compared to those with mild acne severity and as compared to normal control subjects. This suggests that the degree of the impairment of stratum corneum permeability barrier is correlated directly with the acne vulgaris severity. Another consideration: if filaggrin, that is a protein with an important activity against bacterial colonization, is augmented in acne, why do we observe in acne affected skin an abnormal bacterial colonization? All this apparent contradictions can be probably explained by considering not only quantitative, but also qualitative representation of filaggrin. It’s probable, in fact, that in acne lesions augmented levels of filaggrin coexist with a functional impairment of this protein, that could be unable or less able to complete its natural maturation from profilaggrine, trough filaggrin, to natural moisturizing factors (NMFs), the final filaggrin products, essential to maintain skin hydratation, normal TEWL and skin permeability, and to contrast bacterial colonization. For these reasons, the use of topical products containing functional filaggrin could be an effective and innovative therapeutic option. It is also important to consider that some medications, usually used in the acne treatment, can be responsible for additional alterations of the skin function and its integrity. The origin of these additional alterations may be the active substance or the vehicle, or both, but in any case specific skin care recommendations are very important in the management of Page 2 of 7 Inflammation&Cell Signaling 2015; 2: e737.doi: 10.14800/ics.737; © 2015 by G. Fabbrocini, et al. http://www.smartscitech.com/index.php/ics Figure 1. Pathophysiology of acne vulgaris. Keratinocyte hyperproliferation, increased desquamation, sebum accumulation, altered sebum lipid composition and P. acnes growth into the pilo-sebaceous unit, lead to fragile skin, involving barrier impairment and dehydration, and follicular rupture. TEWL, TransEpidermal Water Loss. acne vulgaris in order to potentiate the efficacy of drugs in the reduction of acne lesions[7]. severe cases, nodules and cysts. Acne lesions are distributed essentially on face, chest, and back. Indeed, systemic medications, topical medications, and surgical and physical procedures used to treat acne and acne scaring can cause impairment in stratum corneum barrier function. Benzoyl peroxide and retinoids are particularly responsible for fragile skin, as characterized by irritated skin (burning and stinging), erythema, scaling, and xerosis[6]. The mechanism of action of retinoids involves the increase of epithelial cells turnover and the shedding of corneocytes[15]. Moreover, topical retinoids cause hypergranulosis, acanthosis, desquamation, and a decrease in stratum corneum thickness. “Retinoid dermatitis” is usually transitory, arising after 2-4 weeks and vanishing afterwards. As for the mechanism of action of benzoyl peroxide, reactive oxygen species are produced and the cohesion of keratinocytes are disrupted in the stratum corneum (keratolysis)[16]. Generally, the first lesions appear around 12 years old. In fact, acne is often linked with puberty and less prevalent in adulthood. Nevertheless, juvenile acne can still be found in people between the ages of 20 and 30. It happens to 64% of individuals for the former, and to 43% for the latter and lead to a considerable psychological and social impact[3]. Although this skin disorder is most frequently not severe, people with acne are often subject to anxiety in social situations, and embarrassed with their appearance leading to reduce their quality of life[17]. Formation of acne lesions is well known to be associated with genetic and environmental factors, and especially emotional stress[2, 3]. Pathology of acne: inflammatory role of P. acnes Acne vulgaris is a chronic inflammatory disease of the pilosebaceous unit. Acne is a common condition, with a lifetime prevalence of 80% but it occurs more frequently during the adolescence between 15 and 17 years old[17]. Features of acne include hyperseborrhoea (excessive sebum production), non-inflammatory lesions (comedones), inflammatory lesions characterized by papules, and pustules associated with diverse degrees of scarring, and in the most P. acnes has been identified as a contributing factor in acne lesions by playing an important role in the pathogenesis because of colonization of the pilosebaceous unit and inflammation caused[3, 12, 18]. Acne lesions first develop in the pilosebaceous unit as subclinical microcomedones and may evolve into inflammatory (papules, pustules) and non-inflammatory lesions[2, 19]. The overproduction of sebum and increased follicular hyperkeratosis were thought to be first events leading to establish an environment favourable for the proliferation of P. acnes, and therefore responsible for the appearance of the initial eruptions (microcomedones). However, most recent evidence points that the inflammation begins before the primary eruptions[18]. Indeed, inflammation Page 3 of 7 Inflammation&Cell Signaling 2015; 2: e737.doi: 10.14800/ics.737; © 2015 by G. Fabbrocini, et al. http://www.smartscitech.com/index.php/ics Figure 2. Activation of the NLRP3-inflammasome by P. acnes. Infiltration by inflammatory cells within the pilo-sebaceous unit allows contact between P. acnes and myeloid cells. The phagocytosis of P. acnes by macrophage and the activation of the TLR result in the activation of the NLRP3-inflammasome, and therefore, the release of active IL-1 β. IL-1 β, Interleukin-1β; PAMPs, Pathogen-associated molecular pattern; ROS, reactive oxygen species; TLR, Toll Like Receptor. and the infiltration of perivascular lymphoid can precede lymphoproliferation. Under normal circumstances, the keratinocytes differentiate into corneocytes, which will then desquamate and lost from the stratum corneum surface.[20] In acne vulgaris, changes in the lipid content of sebum associated with the inflammation in and around the sebaceous gland result in keratinocytes hyperproliferation and increased desquamation within sebaceous follicles[18, 9]. Inflammation of the pilosebaceous unit and the build-up of keratinocytes prevent sebum drainage, and thus microcomedones formation[6]. (figure1) P. acnes is responsible for several pro-inflammatory activities. This microorganism triggers the innate immune system by activating toll-like receptor 2 (TLR2) and the inflammasome pathway[21, 22]. The Toll Like Receptors (TLRs) are transmembrane proteins activated by pathogen-associated molecular patterns. The activation of TLRs by exposure to microbial agent leads to the activation of the NF-κB pathway which modulate expression of many immune response genes[23, 24]. P. acnes induces the production of monocyte cytokines, via a TLR2-dependent pathway. Indeed, TLR2 activation leads to stimulate the release of pro-inflammatory cytokines by the monocytes, such as IL-12 and IL-8. It allows to recruit neutrophils to the active lesion site. Through the release of lysosomal enzymes, these neutrophils cause the rupture of follicular epithelium triggering the inflammation[25]. TLR2 expression in acne suggests that the activation of TLR2 by P. acnes can be involved in the inflammatory lesion development[26]. Furthermore, P. acnes can also be phagocyted by myeloid cells resulting in IL-1β release, responsible for the inflammatory response by the neutrophils[22]. Indeed, in human monocytes, P. acnes activates NLRP3-inflammasome leading to maturation of pro-IL-1β to active IL-1β by means of caspase 1[27]. The inflammasome is an intracellular and molecular complex that has the function of initiate inflammation. The danger- and pathogen-associated molecular patterns (DAMPs/PAMPSs) activate the inflammasome which will regulate the release of several caspase-1 activation-dependent cytokines, and especially IL-1β[28]. Overall, NLRP3-inflammasome activation requires thephagocytosis of P. acnes, the release of cathepsin B by the lysosomal rupture, K+ efflux and formation of reactive oxygen species (ROS)[29]. (figure 2) Rhealba® Oat plantlet extract Page 4 of 7 Inflammation&Cell Signaling 2015; 2: e737.doi: 10.14800/ics.737; © 2015 by G. Fabbrocini, et al. http://www.smartscitech.com/index.php/ics The healing properties of oat have been known for thousands of years. Since 400 BC, traditional medicine has Figure 3. Chemical structure of isoorientin-2’’-O-arabinoside (1) and isovitexin-2’’-O-arabinoside (2). been using oat in the form of flour or gruel, for its emollient and anti-inflammatory benefits. The healing virtues of oat are frequently employed for several skin disorders, such as pruritus, burns, ulcers as well as erythema[30]. Today, Rhealba® Oat plantlet extract (Pierre Fabre DermoCosmetique) is usually used for treating fragile skin due to its varied biochemical properties. Indeed, the non-dietary aerial parts of Rhealba® Oat contain essentially flavonoids and saponins, two molecular species which would have interesting anti-inflammatory and immunomodulatory activities. The active components of Rhealba® Oat Plantlets extract were separated by reverse phase liquid chromatography followed by semi-preparative reverse phase HPLC. Two C-glycosylated flavonoids were isolated, one of the apigenin type, isoorientin-2”-O-arabinoside, and the other of the luteolin type, isovitexin-2”-O-arabinoside[1, 31]. (figure 3) The immunomudulatory and anti-inflammatory activity of Rhealba® Oat Plantlets extract and its purified active substances were therefore studied in vitro in several cell models mimicking the different pathways of activation of inflammation[31]. The results suggest that Rhealba® Oat Plantlets extract exerts interesting immunomodulatory activity. In fact, Plantlets extract causes dose-dependent inhibition in the secretion of pro-inflammatory Th1 and Th2 cytokines and particularly on IL-13 and IL-2 production, cytokines that play a central role in controlling the immune response. Moreover, Rhealba® Oat Plantlets extract has an inhibitory effect on the capacity of dendritic cells to stimulate T lymphocyte proliferation. This reduced efficacy of dendritic cells might be due to the weaker expression of the MHC I and II costimulatory molecules on their surface, negatively regulated by the extract[31]. In addition, Rhealba® Oat Plantlets extract presents an anti-inflammatory activity. Indeed, the extract inhibits significantly the production of the prostacycline PG6KF1α, a prostaglandin which is a major metabolite of arachidonic acid resulting from the cyclo-oxygenase pathway in keratinocytes. This effect appears to be exerted by directly inhibiting the activity of the COX-2 enzyme and not by reducing quantity of arachidonic acid[31]. Rhealba® Oat Plantlets extract has also been identified to inhibit bacterial adhesion, especially Staphylococcus aureus, enhance the production of ceramides, cerebrosides and free acide both involved in cutaneous barrier homeostasis. Moreover, the extract stimulates the proliferation of keratinocytes and enhances the production of collagen IV, hyaluronic acid, and sphingomyelin[1]. All of these findings suggest that Rhealba® Oat Plantlets extract is capable of reducing inflammation and irritation in acne. Cosmeceuticals based on Rhealba® Oat plantlet extract FDA identified colloidal oatmeal in 1989 as a skin protectant drug available over the counter and offered to classify it as a category I ingredient which means safe and effective, while waiting for the standardization of its formula[32]. Rhealba® Oat plantlet extract (Pierre Fabre Dermo-Cosmetique) is an oat plantlet extract without protein used to heal fragile skin and is an exclusive ingredient of A-DERMA. This extract is also part of the Phys-AC range, the product line of A-DERMA to treat acne. A-DERMA products contain also hydro-compensating actives to restore fragile skin and reduce irritation and inflammation[33, 34]. Indeed, acne is often associated with irritation and dry skin and the symptoms can be aggravated by anti-acneic treatment such as topical tretinoin or isotretinoin[32]. The Phys-AC range encompasses four products. The first, Phys-AC Global, is employed as a stand-alone cream which associates Rhealba® Oat plantlet extract, anti-comedogenic agents and hydro-compensating actives. In Phys-AC Global, the anti-comedogenic agents are represented by the hydroxy acids. The main hydroxy acid used, is the glycolic acid, a natural product from sugar cane, known to reduce the cohesion of corneocytes, and favor desquamation[35, 36]. Lactic acid, another hydroxyl acid, is used to inhibit the growth of P. acnes and promote keratinocyte desquamation[11, 37]. The last anti-comedogenic agent is the salicylic acid which has keratolytic activity[38]. Another product of Phys-AC is the Hydra cream, which is composed of Rhealba® Oat plantlet extract and hydro-compensating actives. This cream is to be used in addition to anti-acneic Page 5 of 7 Inflammation&Cell Signaling 2015; 2: e737.doi: 10.14800/ics.737; © 2015 by G. Fabbrocini, et al. http://www.smartscitech.com/index.php/ics treatments in order to lessen the irritation and restore fragile skin. The last two Phys-AC products are the purifying foaming gel and the purifying micellar water. They also contain Rhealba® Oat plantlet extract as well as hydro-compensating actives and can be used as daily cleansers. 6. Del Rosso JQ. Clinical relevance of skin barrier changes associated with the use of oral isotretinoin: the importance of barrier repair therapy in patient management. J Drugs Dermatol 2013; 12:626-631. 7. Thiboulot D, Del Rosso JQ. Acne Vulgaris and the Epidermal Barrier: Is acne Vulgaris Associated with Inherent Epidermal Abnormalities that Cause Impairment of Barrier Functions? Do any Topical Acne Therapies Alter the Structural and/or Functional Integrity of the Epidermal Barrier? J ClinAesthetDermatol 2013; 6:18-24. 8. Yamamoto A, Takenouchi K, Ito M. Impaired water barrier function in acne vulgaris. Arch Dermatol Res 1995; 287:214-218. 9. Harding CR, Aho S, Bosko CA. Filaggrin - revisited. Int J CosmetSci 2013; 35:412-423. Conclusions In acne, fragile skin has two origins; the impairment of the skin barrier and the inflammatory nature of this skin disease. These events are mainly attributed to the proliferation of P. acnes. Thanks to its anti-inflammatory, immunomodulatory and barrier restoration properties, Rhealba® Oat plantlet extract is able to reduce inflammation, inhibit adhesion of P. acnes, and thus, restore the fragile skin. Therefore, cosmeceuticals based on Rhealba® Oat plantlet extract associated with hydro-compensating actives, which can be associated with anti-comedogenic agents (hydroxyl acids), may be usually used stand-alone or in addition to anti-acneic treatment for acne vulgaris treatment. 10. Kurokawa I, Mayer-da-Silva A, Gollnick H, Orfanos CE. Monoclonal antibody labeling for cytokeratins and filaggrin in the human pilosebaceous unit of normal, seborrhoeic and acne skin. J Invest Dermatol 1988; 91:566-571. 11. Jarrousse V, Castex-Rizzi N, Khammari A, Charveron M, Dreno B. Modulation of integrins and filaggrin expression by Propionibacterium acnes extracts on keratinocytes. Arch Dermatol Res 2007; 299:441-447. Conflict of interest 12. Guy R, Kealey T. The effects of inflammatory cytokines on the isolated human sebaceous infundibulum. J Invest Dermatol 1998; 110:410-415. GF declares no conflicts of interest. MSA is an employee of Pierre Fabre and FS is a trainee of Medical Direction of A-DERMA 13. Sergeant A, Campbell LE, Hull PR, Porter M, Palmer CN, Smith FJ, et al. Heterozygous null alleles in filaggrin contribute to clinical dry skin in young adults and the elderly. J Invest Dermatol 2009; 129:1042-1045. Abbreviations 14. Common JE, Brown SJ, Haines RL, Goh CS, Chen H, Balakrishnan A, et al. Filaggrin null mutations are not a protective factor for acne vulgaris. J Invest Dermatol 2011; 131:1378-1380. COX: Cyclooxygenase; IL: Interleukin; NMF: Natural Moisturizing Factors; MHC: Major Histocompatibility Complex; P. acnes: Propionibacterium acnes; PG6KF1α: ProstaGlandin 6KF1α; ROS: Reactive Oxygen Species; SC: stratum corneum; TEWL: TransEpidermal Water Loss; Th: Lymphocyte T helper; TLR: Toll Like Receptor. References 1. Stadler JF, Tennsted D, Deleuran M, Fabbrocini G, de Lucas R, Haftek M, et al. Fragility of epidermis and its consequence in dermatology. J EurAcadDermatolVenereol 2014; 28 (Suppl 4):1-18. 2. Williams HC, Dellavalle RP, Garner S. Acne vulgaris. Lancet 2012; 379:361-372. 3. Bhate K, Williams HC. Epidemiology of acne vulgaris. Br J Dermatol 2013; 168:474-485. 4. Grice EA, Kong HH, Conlan S, Deming C, Davis J, Young A, et al. Topographical and temporal diversity of the human skin microbiome. Science 2009; 324:1190-1192. 5. Beylot C, Auffret N, Poli F, Claudel JP, Leccia MT, Del Giudice P, et al. Proponibacterium acnes: an update on its role in the pathogenesis of acne. J EurAcadDermatolVenereol 2014; 28:271-278. 15. Thielitz A, Gollnick H. Topical retinoids in acne vulgaris: update on efficacy and safety. Am J ClinDermatol 2008; 9:369-381. 16. Sagransky M, Yentzer BA, Feldman SR. Benzoyl peroxide: a review of its current use in the treatment of acne vulgaris. Expert OpinPharmacother 2009; 10:2555-2562. 17. Friedlander SF, Baldwin HE, Mancini AJ, Yan AC, Eichenfield LF. The acne continuum: an age-based approach to therapy. SeminCutan Med Surg 2011; 30(Suppl 3):S6-S11. 18. Tanghetti EA. The role of inflammation in the pathology of acne. J ClinAesthetDermatol 2013; 6:27-35. 19. Lai JJ, Chang P, Lai KP, Chen L, Chang C. The role of androgen and androgen receptor in skin-related disorders. Arch Dermatol Res 2012; 304:499-510. 20. Rawlings AV, Scott IR, Harding CR, Bowser PA. Stratum corneummoisturization at the molecular level. J Invest Dermatol 1994; 103:731-741. 21. Kim J, Ochoa M-T, Krutzik S, Takeuchi O, Uematsu S, Legaspi A, et al. Activation of Toll-like receptor 2 in acne triggers inflammatory cytokine responses. J Immunol 2002; 169:1535-1541. 22. Kistowska M, Gehrke S, Jankovic D, Kerl K, Fettelschoss A, FeldmeyerL,et al. IL-1β Drives Inflammatory Responses to Propionibacterium acnes In Vitro and In Vivo. J Invest Dermatol 2014; 134:677-685. Page 6 of 7 Inflammation&Cell Signaling 2015; 2: e737.doi: 10.14800/ics.737; © 2015 by G. Fabbrocini, et al. http://www.smartscitech.com/index.php/ics 23. Suzuki N, Suzuki S, Duncan GS, Millar DF, Wada T, Mirtsos C, et al. Severe impairment of interleukin-1 and Toll-like receptor signaling in mice lacking IRAK-4. Nature 2002; 416:750-756. 24. Takeda K, Kaisho T, Akira S. Toll-like receptors. Annu Rev Immunol 2003; 21:335-376. 25. Webster GF, Leyden JJ, Tsai CC, Baehni P, McArthur WP. Polymorphonuclear leukocyte lysosomal release in response to Propionibacterium acnes in vitro and its enhancement by sera from inflammatory acne patients. J Invest Dermatol 1980; 74:398-401. 26. Kim J. Review of the Innate Immune Response in Acne vulgaris: Activation of Toll-Like Receptor 2 in Acne Triggers Inflammatory Cytokine Responses. Dermatology 2005; 211:193-198. 27. Thiboutot DM. Inflammasome Activation by Propionibacterium acnes: The story of IL-1 in Acne Continous to Unfold. J Invest Dermatol 2014; 134:595-597. 28. Strowing T, Henao-Mejia J, Elinav E, Flavell R. Inflammasomes in health and disease. Nature 2012; 481:278-286. 29. Contassot E, French LE. New insights into inflammatory acne pathogenesis: Propionibacterium acnes activates the inflammasome. J Invest Dermatol 2014; 134:310-313. 30. Fournier P. Le livre des plantesmédicinalesetvénéneuses de France. Edited by Lechevalluer. EncyclopédieBiologique Tome I. Paris, 1948 ; 178. protein-free content and assessment of regulatory activity on immune inflammatory mediators. Planta Med 2011; 77:900-906. 32. Kurtz ES, Wallo W. Colloidal Oatmeal: History, Chemistry and Clinical Properties. J Drugs Dermatol 2007; 6:167-170. 33. Bartenjev I, Oremovic L, RoglButina M, SjerobabskiMasnec I, Bouloc A, Voda K, et al. Topical effectiveness of a cosmetic skincare treatment for acne-prone skin: a clinical study. ActaDermatovenerol Alp PanonicaAdriat 2011; 20:55-62. 34. Goodman G. Cleansing and moisturizing in acne patients. Am J ClinDermatol 2009; 10(Suppl 1):1-6. 35. Van Scott EJ, Yu RJ. Hyperkeratinization, corneocyte cohesion, and alphahydroxy acids. J Am AcadDermatol 1984; 11:867-879. 36. Van Scott EJ, Yu RJ. Alpha hydroxy acids: procedures for use in clinical practice. Cutis 1989; 43:222-228. 37. Kim TH, Choi EH, Kang YC, Lee SH, Ahn SK. The effects of topical alpha-hydroxyacids on the normal skin barrier of hairless mice. Br J Dermatol 2001; 144: 267-273. 38. Waller JM, Dreher F, Behnam S, Ford C, Lee C, Tiet T, et al. ‘Keratolytic’ properties of benzoyl peroxide and retinoic acid resemble salicylic acid in man. Skin PharmacolPhysiol 2006; 19:283-289. 31. Mandeau A, Aries MF, Boé JF, Brenk M, Crebassa-Triqueros V, Vaissière C, et al. Rhealba® oat plantlet extract: evidence of Page 7 of 7