Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
257
Renal Functional Reserve and
Microalbuminuria in Offspring of
Hypertensive Parents
Beatriz Grunfeld, Eduardo Perelstein, Rosa Simsolo, Maria Gimenez, and Juan C. Romero
Downloaded from http://hyper.ahajournals.org/ by guest on June 15, 2017
Renal functional reserve, microalbuminuria, and plasma atrial natriuretic factor were measured
in 21 offspring (9.5±0.5 years of age, mean±SEM) of hypertensive parents and in eight children
(10±0.5 years of age) with no family history of hypertension who were used as a control group.
Renal functional reserve was evaluated by measurement of the changes in creatinine clearance
after an oral protein load of 45 g/m2. Atrial natriuretic factor levels were determined before and
60 minutes after the protein load, and microalbuminuria in fractional urine before and 120
minutes after the same stimulus as well as in a 24-hour urine collection. All children in the
control group significantly increased their creatinine clearance after the protein load (preload,
122±12; 60 minutes, 144±9; 120 minutes, 154±11; 180 minutes, 144±9 ml/min/1.73 m2; all values
were significant vs. preload, p< 0.005). In contrast, only 13 of 21 offspring of hypertensive parents
increased their creatinine clearance to values within 2 SD of the increase shown by the control
group (preload, 144±11; 60 minutes, 153 ±7; 120 minutes, 202±13 ml/min/1.73 m2;/?<0.001 vs.
preload; 180 minutes, 214±19 ml/min/1.73 m2, p<0.001 vs. preload). The remaining eight
offspring of hypertensive parents showed no detectable changes (nonresponders) (preload,
189±18; 60 minutes, 146±11; 120 minutes, 170±14; 180 minutes, 168±13 ml/min/1.73 m2; all
values p=NS). No changes in atrial natriuretic factor after the protein load were observed in any
group. Offspring of hypertensive parents presented higher microalbuminuria levels in 24-hour
urine specimens (3.1 /tg/min, tolerance factor [TF]2.2) than controls (2.1 /ig/mln, TF 1.5)
(j?<0.05). Although microalbuminuria increased significantly after the water load in the control
group (/?<0.05) and in the offspring of hypertensive parents (/><0.01), it returned to baseline at
120 minutes in the former but not in the latter (p<0.05 vs. baseline). The lack of renal functional
reserve in nonresponders was significantly related (p<0.05) to the presence of higher levels of
microalbuminuria. We conclude that the absence of renal functional reserve and increased
microalbuminuria in some normotensive children who are offspring of essential hypertensive
parents can indicate that subtle alterations in renal function may precede the onset of clinical
hypertension. {Hypertension 1990;15:257-261)
S
everal lines of evidence suggest that a genetic
factor is involved in the pathogenesis of
essential hypertension in some patients.1-2 A
number of past observations supports the hypothesis that inherited abnormalities in kidney function
may participate in the pathogenesis of essential
hypertension.3-5
From the Hipertension Arterial, Hospital de Niflos "Ricardo
Gutierrez" (B.G., R.S.), the Department of Nephrology, Hospital
de Niflos "Ricardo Gutierrez" (E.P.), Buenos Aires, Argentina,
the Pediatric Clinical Chemistry Laboratory Hospital Italiano
(M.G.), Buenos Aires, Argentina, and the Department of Physiology and Biophysics, Mayo Clinic (J.C.R.), Rochester, Minnesota.
Partially supported by grant HL-16496 from the National Institutes of Health.
Address for reprints: Dr. J.C. Romero, Mayo Clinic, 200 First
Street SW, Rochester, MN 55905.
Received May 25,1989; accepted in revised form November 24,
1989.
We have reported decreased active and inactive
urinary kallikrein excretion after a diuretic stimulus
in a subgroup of normotensive offspring of essential
hypertensive parents as well as in normotensive
children with a single kidney.6 As urinary kallikrein
has been proposed as an indicator of distal tubular
mass or function,7 our findings could be interpreted
as an expression of a diminished functional renal
mass in the normotensive offspring of hypertensive
parents.
To gather additional information on their renal
function, we evaluated the renal functional reserve
(as indicated by the increase in the creatinine clearance after an oral protein load) and the microalbuniin excretion in a group of normotensive children
who are offspring of essential hypertensive parents.
Oral protein load has been shown to increase glomer-
258
Hypertension Vol 15, No 3, March 1990
TABLE 1.
Basal Blood Pressure at the Beginning of the Study
N-EH
Control
Downloaded from http://hyper.ahajournals.org/ by guest on June 15, 2017
Patient no.
Sex
Age (yr)
BP (mm Hg)
Control no.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
F
F
M
F
M
M
M
F
M
F
M
F
M
M
F
M
M
M
F
F
F
6
12
14
7
14
12
7
5
7
10
13
11
9
13
8
9
14
5
9
11
6
100/68
108/70
116/70
104/64
120/80
118/70
1.
2.
3.
4.
5.
6.
7.
8.
Mean±
SEM
110/60
104/50
110/60
110/70
122/70
114/72
112/62
120/70
110/70
112/70
120/80
106/66
110/70
110/70
90/64
111/68
Sex
F
M
M
F
F
M
M
M
Age(yr)
BP (mm Hg)
10
9
11
8
11
10
11
12
90/60
108/60
115/65
100/70
90/60
114/70
114/72
118/70
Mean±
106/66
SEM
4/2
2/1
N-EH, nonnotensive children with a single hypertensive parent; BP, blood pressure.
ular filtration rate in healthy subjects.8 Because atrial
natriuretic factor (ANF) has been reported to increase
the glomerular nitration rate,9 we also measured
plasma fluctuations of ANF after the oral protein load.
Methods
Patient Population
Twenty-one nonnotensive children (N-EH) with
a single essential hypertensive parent (11 boys,
mean age 9.5 ±0.5 years) and eight nonnotensive
children without a family history of essential hypertension (C) (five boys, mean age 10 ±0.5 years) who
were attending the Outpatients Clinic at Children's
Hospital were included in the study. Children were
considered nonnotensive according to the criteria
of the Second Task Force on Blood Pressure Control in Children (Table 1). Creatinine clearances
(Ccr) were within the normal range in all propositi
and none had proteinuria. All subjects were free of
medication at the time of the study. All studies were
carried out on an outpatient basis.
Oral Protein Load
Studies were started at 8:00 AM after an overnight
fast. After emptying their bladders, the children were
given an oral water load of 20 ml/kg body wt, after
which two timed 30-minute urine samples were collected by spontaneous voiding; at a midpoint of each
30-minute period, blood was drawn for the creatinine
determination from an intravenous butterfly needle
introduced into a peripheral arm vein. Baseline Ccr
was calculated from the mean value obtained at the
two 30-minute periods. The children were then fed
an oral protein load (OPL) (lean, cooked hamburger
meat) of 45 g/m2 body surface area ingested during a
20-30-minute period. After the meal was completed,
three 60-minute urine samples were collected and
blood again drawn at the midpoint of each period for
Ccr. At the end of each urine collection, an amount
of water equivalent to the volume voided was
ingested by each child. Blood pressure was taken
hourly from the preload period through the third
hour of the post-protein load period with a mercury
sphygmomanometer.
Plasma and urinary creatinine were measured by a
standard method by means of an automatic analyzer
(Abbott VP Bichromatic Analyzer, Abbott Labs.,
Dallas, Texas), and Ccr was corrected for body
surface and expressed per 1.73 m2. Urinary sodium
was measured in the 24-hour urine collection by
flame spectrophotometry.
Microalbuminuria was measured in three different
urine samples: 1) 24-hour urine specimen collected
the day before the OPL study; 2) in the second
30-minute urine collection after the water load
administered before the protein meal; 3) in the
second 60-minute urine collection after the protein
load. Urinary urea was also measured in the last two
Grunfeld et al
TABLE 2.
Renal Functional Reserve in Children
259
Creatinine Clearance Values After an Oral Protein Load
Postload
Group
Control
N-EH
Responders
Nonresponders
n
8
21
13
8
Basal
143±22
135±8
134±11
136±14
Preload
1 hour
2 hours
122±12
161±11
144±11
189±18||
144±9*
151±6
153±7
146±11
154±llf
156±18
202±13§
170±14
3 hours
144±9*
169±21
214±195
168±13
Values are mean±SEM (ml/min/1.73 m2). N-EH, norraotensive offspring of hypertensive parents; basal, values
obtained from 24-hour urine collected the day before the study.
*p<0.05; :tp<0.01; t.P<0.005; §p<0.001 when compared with respective preload values. ip<0.01 when compared
with N-EH responders.
Downloaded from http://hyper.ahajournals.org/ by guest on June 15, 2017
samples. Microalbuminuria was measured by radioimmunoassay with the method of Miles et al,10 as
modified in our laboratory. The first antibody was
purchased from Serotec (Oxfordshire, UK). Standards for iodination and standard curves were from
Calbiochem (Calbiochem Corp., La Jolla, California)
catalogue No. 126658 and 126654, respectively.
Interassay variation coefficient was 15% and 13%,
respectively, and the sensitivity was 7.8 ng.
ANF was measured by radioimmunoassay in three
different plasma samples: 1) in basal conditions
before the water load, 2) 1 hour after the water load
and before the protein meal, and 3) 1 hour after the
protein load. Plasma levels of ANF were measured
with the method of Gutkowska et al.11 The antibody
against ANF-(99-126) was kindly supplied by Y.
Gutkowska, who also helped us set up the assay in
our laboratory. All the other reactions were obtained
from Peninsula Labs., Inc., Belmont, California.
Parental consent for the present study was obtained
after giving appropriate information in all cases.
Statistical Methods
Statistical analysis of the results was done by
nonparametric methods because changes in Ccr after
the protein load, as well as microalbuminuria, may
not follow a normal distribution, as stated by other
authors. The Wilcoxon signed rank test was used to
evaluate changes in Ccr after the protein load within
each group. The median test was applied to study the
differences among the groups. Fisher's exact test on
two-by-two contingency tables were used to determine a possible relation between the response to the
protein load and microalbuminuria. Results are
expressed as mean±SEM, except for microalbuminuria; which is expressed antilogged with a geometric
mean (GM) equivalent to the arithmetic mean of the
logged data, and a tolerance factor (TF) equivalent to
the standard deviation of the logged data, except that
the GM is multiplied or divided by the TF. Results
were considered statistically significant whenp<0.05.
Results
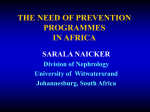
Creatinine clearance values obtained after the oral
protein load are shown in Table 2. Although the Ccr
in the children in the control group increased significantly after the protein load (p<0.005), no significant changes in the mean Ccr were recorded in the
N-EH group children. However, when the results
obtained in the latter group were analyzed in a more
discriminative manner, two subsets of children could
be identified: 13 of 21 children in the N-EH group
(62%) did in fact increase their Ccr significantly
(p<0.001) (responders) to values within 2 SD of the
increase shown by the control group, whereas 8 of 21
children in the N-EH group (38%) did not (nonresponders) (Figure 1).
No significant changes in blood pressure were
recorded throughout the study.
Basal urinary urea excretion was similar in N-EH
responders and nonresponders, and it increased significantly after the protein load (responders: basal
13.4±9 g and post-protein load 16.3±1.2 g,p<0.01;
nonresponders: basal 10.7±1.7 g and post-protein
Ioadl8.2±2.5g, j p<0.01).
Urinary sodium excretion was similar in the N-EH
responder and nonresponder groups, and it was not
different from the control groups (responders, 98 ±17
meq/24 hr; nonresponders, 94 ±20 meq/24 hr; and C,
110±23 meq/24 hr).
Basal plasma ANF levels were similar in control
and N-EH children, and they showed no signficant
changes either after the water load or after the
protein load (C: basal 107±10 pg/ml, after water load
98±18 pg/ml, and after protein load 94±5 pg/ml;
N-EH: basal 111±47 pg/ml, after water load 118±46
pg/ml, and after protein load 124±67 pg/ml).
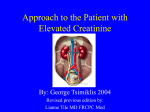
Microalbuminuria in the 24-hour urine collection
was higher in a total population of 33 N-EH than in
CONTROLS
PRE
POST
PRE
POST
FIGURE 1. Graph showing creatinine clearance response to
an oral protein load. N-EH, normotenswe offspring of hypertensive parents; full lines, responders; dotted lines, nonresponders.
260
Hypertension
Vol 15, No 3, March 1990
motensive when transplanted with a kidney donated
from a normotensive rat3-4 lent support for the theory
on the primacy of the kidney in the pathogenesis of
essential hypertension. A dramatic reversal of hypertension has also been reported in some patients with
end-stage renal disease after successful renal
transplantation.12'13 Thus, a number of past observations support the contention that something in the
kidney may be primarily at fault, in at least a subset
of essential hypertensive patients.
Healthy subjects have been shown to increase their
glomerular filtration rate after a meat meal, and this
increase has been considered a measure of the renal
Basal
PruWntaad
functional reserve. Patients with renal disease have a
Oonbo)
lack of renal functional reserve, and the presence of
FIGURE 2. Graph showing microalbuminuria response to an glomerular hyperfiltration in the remnant nephrons
oral protein load. N-EH, normotensive offspring of hyperten- has been postulated as the underlying mechanism.
sive parents. *p<0.05; **p<0.01 vs. respective baseline.
Further support for the latter comes from experimental data demonstrating an increase in single
nephron glomerular nitration rate of the remnant
20 appropriate control subjects (N-EH: 3.1 ^g/min,
nephrons after renal ablation.14
TF 2.2; C: 2.1 jig/min, TF 1.5;/J<0.05). Microalbuminuria increased significantly 1 hour after the water
Our present finding of a lack of renal functional
load in the 21 N-EH (p<0.01) and in the eight
reserve in a subset of normotensive offspring of
control subjects (p<0.05) included in the study (Nessential hypertensive patients, together with our
EH: 12.1, TF 2.6; C: 8.8, TF 1.9 fig/min). Although
past observation of a decreased urinary kallikrein
microalbuminuria decreased 2 hours after the protein
excretion in both the N-EH and normotensive single
load in both groups, the N-EH group had not returned
kidney children,6 lend additional support to our
to baseline whereas the control group did (N-EH: 8.2,
hypothesis that a diminished functional renal mass is
TF 1.6 ng/min, p<0.05 vs. baseline; C: 4.3, TF 1.7
present in a subset of normotensive children who are
jtg/min) (Figure 2). The lack of Ccr response to the
offspring of essential hypertensive parents.
protein load in the N-EH children was significantly
A primary defect in glomerular development leadrelated (p<0.05) to the presence of high levels of
ing to a reduction in single nephron filtration rate
microalbuminuria (>mean 2 TF of control group).
(probably due to a lower glomerular hydraulic conductivity or surface area) was described in Milan
Discussion
hypertensive strain rats, an animal model for essential hypertension.15 Based on these data, it may be
Our results indicate that the creatinine clearance
speculated that hypofiltration rather than hyperfiltraresponse to an oral protein load was significantly
tion could have led to the lack of renal functional
altered in 38% of a cohort of N-EH children, sugreserve found in some of our patients.
gesting that some of these children may have an
abnormal renal functional reserve in spite of having
Vascular structural changes before the developshown normal renal function by standard diagnostic
ment of hypertension have been reported in spontatests. In addition, N-EH children presented signifineously hypertensive rats.16 An inappropriate vascucantly increased mean microalbumin excretion when
lar constrictory state has recently been postulated to
compared with control subjects without a family
be present in offspring of essential hypertensive
history of essential hypertension. Furthermore, a
parents.17 Therefore, structural or functional vascusignificant relation between the lack of renal funclar alterations, or both, may be mediators of the lack
tional reserve and increased microalbuminuria was
of response to the meat meal.
also found in these children.
Differences in dietary protein intake or in the
absorption of the meat meal could be ruled out as
We used the endogenous creatinine clearance as
responsible for our findings as 24-hour urinary urea
an estimation of the glomerular nitration rate, as
was similar in all children studied and urea excretion
other authors have previously shown that creatinine
after the protein load increased comparably in both
clearance and inulin clearance rendered similar
responder and nonresponder N-EH groups.
results in this test.8 Although it has long been known
that both clearances may be discordant because of
A restricted sodium diet cannot be related to the
tubular secretion of creatinine, this discrepancy
lack of creatinine clearance either, as the urinary
becomes important only when the glomerular filtrasodium excretion was again similar in both N-EH
tion rate is decreased. Differences between both
subgroups.18
clearances have previously been reported to be less
Our findings do not support a role for ANF in
than 10% in subjects with normal renal function.
mediating the creatinine clearance response to an
The observation that bilaterally nephrectomized
oral protein load. The increased microalbuminuria
spontaneously hypertensive rats will become norfound in N-EH children could have been the result of
mtarodbumkulii (ug/mln)
Downloaded from http://hyper.ahajournals.org/ by guest on June 15, 2017
Grunfeld et al Renal Functional Reserve in Children
early alterations in the glomerular capillary permeability secondary to glomerular hemodynamic abnormalities, as previously suggested.19 The above speculation is furthered by our observation of a significant
relation between the absence of renal functional
reserve and microalbumin excretion in the N-EH
group.
In synthesis, the absence of renal functional
reserve and increased microalbuminuria in some
normotensive children who are offspring of essential
hypertensive parents, indicate that subtle alterations
in renal function may precede the onset of clinical
hypertension. Long-term follow-up of these children
may contribute to the understanding of the pathophysiological meaning of the findings here reported
and presumably establish their possible usefulness
for the identification of children at risk for developing essential hypertension.
Downloaded from http://hyper.ahajournals.org/ by guest on June 15, 2017
References
1. Bianchi G, Cusi D, Barlassina C, Lupi P, Ferrari P, Picotti G,
Gatti M, Polli E: Renal dysfunction as a possible cause of
essential hypertension in predisposed subjects. Kidney Int
1983;23:870-875
2. Platt R: Heredity in hypertension. Lancet 1963;l:899-904
3. Bianchi G, Fox U, DiFrancesco GF, Giovanetti AM, Pagetti
D: Blood pressure changes produced by kidney crosstransplantation between spontaneously hypertensive rats and
normotensive rats. Clin Sci Mol Med 1974;47:435-448
4. Dahl LK, Heine M: Primary role of renal homografts in setting
chronic blood pressure levels in rats. Ore Res 1975;36:692-696
5. Guyton AC: Arterial Pressure and Hypertension. Philadelphia,
WB Saunders Co, 1980, pp 457-569
6. Grunfeld B, Gimenez M, Simsolo R, Becu L: Kalikrina
urinaria total y activa en ninos hipertensos y en ninos con
rinon unico (abstract). Mcdicina 1987;47:571
7. Spragg J, Denney DL, Tilney NL, Austen KF: Kallikrein
excretion in renal transplant recipients and in uninephrectomized donors. Kidney Int 1985;28:75-81
261
8. Bosch JP, Sacaggi A, Lauer A, Ronco C, Belledonne M,
Glabman S: Renal functional reserve in humans. Effect of
protein intake on glomerular filtration rate. Am J Med 1983;
75:943-950
9. Ortola FV, Ballermann BJ, Anderson S, Mendez RE, Brenner
BM: Elevated plasma atrial natriuretic peptide levels in diabetic rats. Potential mediator of hyperfiltration. / Clin Invest
1984;80:670, 674
10. Miles D, Mogensen C, Gundersen H: Radioimmunoassay for
urinary albumin using a single antibody. Scand J Clin Lab
Invest 1970;26:511-514
11. Gutkowska J, Bourassa M, Roy D, Thibault G, Garcia R,
Contin N, Genest J: Immunoreactive atrial natriuretic factor
(ir-ANF) in human plasma. Btochem Biophys Res Commun
1985;128:1350-1356
12. Rao TKS, Gupta SK, Butt KMH, Kauntz SL, Friedman EA:
Relationship of renal transplantation to hypertension in end
stage renal failure. Arch Intern Med 1978;138:1236-1241
13. Curtis JJ, Luke RG, Dustan HP, Kashgarian M, Whelchel JD,
Jones P, Diethelm AG: Remission of essential hypertension
after renal transplantation. NEnglJMed 1983^09:1009-1015
14. Ayslett JP: Functional adaptation to reduction in renal mass.
Physiol Rev 1979^59:137-164
15. Baer PG, Bianchi G: Renal micropuncrure study of normotensive and Milan hypertensive rats before and after development
of hypertension. Kidney Int 1978;13:452-466
16. Eccleston-Joyner CA, Gray SD: Arterial hypertrophy in the
fetal and neonatal spontaneously hypertensive rat. Hypertension 1988;12:513-518
17. Blackshear JL, Garnic D, Williams GH, Harrington DP,
Hollenberg NK: Exaggerated renal vasodilator response to
calcium entry blockade in first-degree relatives of essential
hypertensive subjects. Hypertension 1987;9:384-389
18. Ruilope L, Rodicio J, Garcia Robles R, Sancho J, Miranda B,
Granger J, Romero JC: Influence of a low sodium diet on the
renal response to aminoacid infusions in humans. Kidney Int
1987;31:992-999
19. Hostetter TH, Olson JL, Rennke HG, Venkachatalam MA,
Brenner BM: Hyperfiltration in remnant nephrons: A potentially adverse response to renal ablation. Am J Physiol 1981;
241-.F85-F93
KEY WORDS •
family history
microalbuminuria
renal function
atrial natriuretic factor
Renal functional reserve and microalbuminuria in offspring of hypertensive parents.
B Grunfeld, E Perelstein, R Simsolo, M Gimenez and J C Romero
Hypertension. 1990;15:257-261
doi: 10.1161/01.HYP.15.3.257
Downloaded from http://hyper.ahajournals.org/ by guest on June 15, 2017
Hypertension is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231
Copyright © 1990 American Heart Association, Inc. All rights reserved.
Print ISSN: 0194-911X. Online ISSN: 1524-4563
The online version of this article, along with updated information and services, is located on the
World Wide Web at:
http://hyper.ahajournals.org/content/15/3/257
Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in
Hypertension can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial
Office. Once the online version of the published article for which permission is being requested is located, click
Request Permissions in the middle column of the Web page under Services. Further information about this
process is available in the Permissions and Rights Question and Answer document.
Reprints: Information about reprints can be found online at:
http://www.lww.com/reprints
Subscriptions: Information about subscribing to Hypertension is online at:
http://hyper.ahajournals.org//subscriptions/