Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
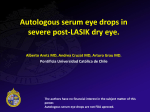
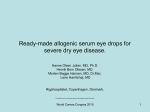
New York State Council on Human Blood and Transfusion Services GUIDELINES FOR AUTOGENEIC SERUM EYE DROPS 2012 New York State Council on Human Blood and Transfusion Services New York State Department of Health Wadsworth Center Empire State Plaza; P.O. Box 509 Albany, New York 12201-0509 2012 New York State Council on Human Blood and Transfusion Services Blood and Tissue Resources Program Wadsworth Center New York State Department of Health Empire State Plaza; P.O. Box 509 Albany, New York 12201-0509 Phone: Fax: E-mail: (518) 485-5341 (518) 485-5342 [email protected] For additional information, this and the Council’s other blood services guidelines are available at: www.wadsworth.org/labcert/blood_tissue ii NEW YORK STATE COUNCIL ON HUMAN BLOOD AND TRANSFUSION SERVICES Members (2012) Donna L. Skerrett, M.D., M.S., Chairperson Chief Medical Officer Mesoblast Ltd New York, NY David Huskie, R.N. Petersburg, NY Philip L. McCarthy, M.D. Clinical Blood and Marrow Transplant Director Roswell Park Cancer Institute Buffalo, NY Joseph Chiofolo, D.O. Medical Director, Transfusion Service Winthrop University Hospital Mineola, NY Lazaro Rosales, M.D. Director, Blood Bank SUNY Health Science Center Syracuse, NY Rachel Elder, M.D. Director of Laboratory Crouse Hospital Syracuse, NY Nirav R. Shah, M.D., M.P.H. (Ex-officio) Commissioner New York State Department of Health Albany, New York Alicia E. Gomensoro, M.D. Director, Blood Bank Maimonides Medical Center Brooklyn, NY Kathleen Grima, M.D. Blood Bank Director The Brooklyn Hospital Center Downtown Campus Brooklyn, NY Jeanne V. Linden, M.D., M.P.H. Executive Secretary Director, Blood and Tissue Resources Wadsworth Center New York State Department of Health Albany, New York iii NEW YORK STATE COUNCIL ON HUMAN BLOOD AND TRANSFUSION SERVICES BLOOD SERVICES COMMITTEE Members (2012) Joseph Chiofolo, D.O., Chairperson * Medical Director, Transfusion Service Winthrop University Hospital Mineola, NY Patricia T. Pisciotto, M.D. Chief Medical Officer American Red Cross Northeast Division Blood Services Farmington, CT Visalam Chandrasekaran, M.D. Associate Professor School of Health Professions and Nursing Long Island University Brookville, NY Timothy Hilbert, M.D., Ph.D., J.D. Medical Director, Blood Bank NYU Langone Medical Center New York, NY Helen Richards, M.D. Blood Bank Director Harlem Hospital New York, NY † Beth Shaz, M.D. Chief Medical Officer New York Blood Center New York, NY Joan Uehlinger, M.D. Director, Blood Bank Montefiore Medical Center Bronx, NY Jeanne V. Linden, M.D., M.P.H. * Director, Blood and Tissue Resources Wadsworth Center New York State Department of Health Albany, NY † Chairperson, Guideline Working Group * Member, Guideline Working Group The Council gratefully acknowledges the assistance of the following Wadsworth Center staff member in preparation of this document: Danuta Olkowska, M.D. Associate Director, Blood and Tissue Resources Program iv NEW YORK STATE COUNCIL ON HUMAN BLOOD AND TRANSFUSION SERVICES GUIDELINES FOR AUTOGENEIC SERUM EYE DROPS Introduction Autogeneic serum eye drops (ASEs) may be used to promote corneal re-epithelialization in cases of severe dry eye or persistent corneal epithelial defects that are unresponsive to conventional therapy.1 The primary source of the corneal epithelium’s nutrition is natural tears, but lacrimation may be insufficient to promote epithelialization in severe epithelial disorders. ASEs without preservatives are non-allergenic, and have biomechanical and biochemical properties similar to those of natural tears. The pH and osmolarity of serum equal those of natural tears, and serum contains growth factors, the adhesion factor fibronectin, immunoglobulins, complement, and vitamins needed for corneal repair. ASEs have been used to relieve symptoms of dry eye and promote healing in ocular surface disorders associated with autoimmune conditions, neurotrophic keratides, and after cornea transplantation or LASIK surgery. Duration of treatment is variable. Most patients show subjective and/or objective improvement in one to four weeks and treatment can be tapered. Some erosions may recur, necessitating resumption of therapy. Patients with severe conditions such as advanced ocular cicatricial pemphigoid and Stevens-Johnson syndrome may need to use the eye drops every 15 minutes during waking hours indefinitely. The number of reported complications is small, but complications are difficult to evaluate because some may be attributed to the patient’s disease or other concurrently applied therapies. Microbial contamination is the biggest concern and may lead to microbial keratitis. Other adverse effects attributed to the use of ASEs include inflammatory response, eczema, and scleral vasculitis in a patient with rheumatoid arthritis. Contraindications include elevated bilirubin or protein, active viral or fungal infection, and certain medications that may injure the cornea. The clinician will order preparation of ASEs following documented patient informed consent. Preparation of ASEs from autogeneic whole blood is considered a reinfusion procedure as defined in 10 NYCRR, Subpart 58-2 (Blood Banks). Hospitals and blood centers holding a Department permit in Blood Services – Collection or Blood Services – Transfusion may perform reinfusion procedures under such a permit. Other sites must be approved by the Department as a Limited Reinfusion Service (LRS). An LRS application packet can be obtained from the Blood and Tissue Resources Program at (518) 485-5341 or [email protected]. There must be written protocols for all procedures pertinent to ASEs. Currently there is no single accepted method of preparation of ASEs and no FDA requirements for establishments producing or distributing these products. Geerling and colleagues sought to develop a standardized manufacturing process and, in 2004, following consideration of many factors, published a detailed protocol.2 1 Blood Collection Microbial contamination is possible during ASE preparation and at point of use. Precautions should be taken to minimize this risk, including disinfection of the phlebotomy site using methods generally accepted for collection of blood for transfusion. Blood should be collected into a sterile blood bag, without anticoagulant, or other container with a sterile interior and sterile entrance port. The person drawing the blood should initial or sign the records pertaining to the collection and attest that the patient identification on the blood and on the pertinent records is correct. Testing for infectious disease markers may be required by the collecting or processing facility. Preparation Blood specimens and ASEs must be stored and transported in an appropriate container, to maintain the required temperature as determined by either the collector or processor. Eye drop preparation should be carried out using aseptic technique. Maintenance of a closed system may not be possible during aliquoting of the final product. Passage through a 0.2µ filter may reduce microbes, but this cannot be relied on to assure sterility. Dilution of serum (1:4) may be appropriate to decrease the concentration of transforming growth factor-beta (TGF-beta), which has an inhibitory effect on the epithelialization process. Diluents may include preservative-free balanced salt solution or saline. Some practitioners advocate use of an antibiotic as a diluent, but this can cause allergic reactions. Labeling Accurate identification must be in place throughout the process. All containers that are used in the collection, processing, and/or final packaging must be properly labeled. Collection and final packaging containers must be labeled with two forms of identification, one of which must be the patient’s name. The final product label or labeling materials must also include a description of the contents and the expiration date, if applicable. Packaging/Dispensing/Storage The final product should be packaged into aliquots in sterile screw cap dropper vials. The ASEs can be stored frozen in a home freezer, then a dropper bottle thawed and stored at 4°C after opening. Thawing a fresh aliquot each day is preferred. Some practitioners have advocated storage at 4°C for up to one week or even 30 days. However, one study demonstrated increasing frequency of microbial contamination after initially sterile bottles with droppers were stored refrigerated in a residential setting.3 If 2 aliquots are to be stored refrigerated for more than one day, the safety of such an extended shelf-life should be validated. The shelf-life for frozen storage, based on stability of growth factors in frozen serum, has been reported to be 3 months. Patient education and detailed instructions for use and storage are important elements to reduce microbial contamination at the point of use. Patients may be advised to use antibiotic eye drops concurrently. Records Complete and accurate records of all steps in the process must be created and maintained. All pertinent records must be retained for a minimum of seven years. Quality Management In hospitals, the collection, processing, and dispensing of ASEs are subject to review by the Transfusion Committee or hospital Quality Committee. ASE procedures must comply with written protocols approved by: o the director of the transfusion service and the transfusion committee; o the director of the hospital department collecting the blood and/or dispensing ASEs; and o the director of the hospital department or facility where processing is performed, if different. In blood centers, the collection, processing, and/or dispensing of ASEs are the responsibility of the director. ASE procedures must comply with written protocols approved by the director. In other settings, the collection, processing, and/or dispensing of ASEs, including record keeping and the reporting of errors and accidents, are the responsibility of the director of the limited reinfusion service. ASE procedures must comply with written protocols approved by the director of the limited reinfusion service. All errors and accidents in collection, testing, preparation, storage or distribution of autogeneic serum eye drops that may affect the safety or purity of the product, or health of the recipient, must be reported to the NYS Department of Health with sufficient detail to facilitate evaluation and investigation, within seven days of occurrence or discovery. 3 REFERENCES 1. Yamada C, King KE, Ness PM. Autologous serum eye drops: Literature review and implications for transfusion medicine specialists. Transfusion 2008;48:1245-55. 2. Geerling G, MacLennan, Hartwig D. Autologous serum eye drops for ocular surface disorders. Br J Ophthalmol 2004;88:1467-74. 3. Sauer R, Blüthner K, Seitz B. Sterility of non-preserved autologous serum eye drops for treatment of persistent corneal epithelial defects. Ophthalmologe 2004;101:705-9. *************************************************************************************************** OTHER PERTINENT LITERATURE American Academy of Ophthalmology Cornea/External Disease Panel. Preferred practice pattern®: Dry eye syndrome – limited revision. San Francisco, CA: American Academy of Ophthalmology, 2011. Available at: www.aao.org/ppp. Jover Botella A, Márquez Peiró JF, Márques K, et al. Effectiveness of 100% autologous serum drops in ocular surface disorders. Farm Hosp 2011;35(1):8-13. Lagnado R, King AJ, Donald F, Dua HS. A protocol for low contamination risk of autologous serum drops in the management of ocular surface disorders. Br J Ophthalmol 2004;88:464-5. Liu L, Hartwig D, Harloff S, et al. An optimised protocol for the production of autologous serum eyedrops. Graefe’s Arch Clin Exp Ophthalmol 2005;243:706-14. Noble BA, Loh RSK, MacLennan S, et al. Comparison of autologous serum eye drops with conventional therapy in a randomized controlled crossover trial for ocular surface disease. Br J Ophthalmol 2004;88:647-52. Ogawa Y, Okamoto S, Mori T, et al. Autologous serum eye drops for the treatment of severe dry eye in patients with chronic graft-versus-host disease. Bone Marrow Transplant 2003;31:579-83. Partal A, Scott E. Low-cost protocol for the production of autologous serum eye drops by blood collection and processing centres for the treatment of ocular surface diseases. Transfus Med 2011;21(4):271-7. Reed-Kane D, Carlson RA, Kupiec TC. Applications and sterility of autologous serum eye drops. Int J Pharm Comp 2009;13:541-3. Research in dry eye: Report of the Research Subcommittee of the International Dry Eye Workshop (2007). Ocul Surf 2007;5(2):179-93. Sanz-Marco E, Lopez-Prats MJ, Garcia-Delpech S, et al. Fulminant bilateral Haemophilus influenza keratitis in a patient with hypovitaminosis A treated with contaminated autologous serum. Clin Ophthalmol 2011;5:71-3. 4 Schulze SD, Sekundo W, Kroll P. Autologous serum for the treatment of corneal epithelial abrasions in diabetic patients undergoing vitrectomy. Am J Ophthalmology 2006;142:207-11. Tananuvat N, Daniell M, Sullivan LJ, et al. Controlled study of the use of autologous serum in dry eye patients. Cornea 2001;20(8):802-6. Tsubota K, Goto E, Fujita H, et al. Treatment of dry eye by autologous serum application in Sjögren’s syndrome. Br J Ophthalmol 1999;83:390-5. Tsubota K, Goto E, Shimmura S, Shimazaki J. Treatment of persistent corneal epithelial defect by autologous serum application. Ophthalmology 1999;106:1984-9. 5