Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Heart failure wikipedia , lookup
Jatene procedure wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Myocardial infarction wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Electrocardiography wikipedia , lookup
Ventricular fibrillation wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
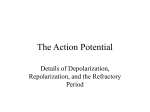
1346 Effect of Altered Activation Sequence on Epicardial QRST Area and Refractory Period in Dogs Kanji Hanashima, MD; Isao Kubota, MD; Taketoshi Ozawa, MD; Takehiko Shibata, MD; Michiyasu Yamaki, MD; Kozue Ikeda, MD; and Shoji Yasui, MD Downloaded from http://circ.ahajournals.org/ by guest on June 15, 2017 Background. We investigated the effects of activation sequence on cardiac surface QRST areas and refractory periods in experiments on dogs. Meth.ods and Results. Right and left ventricular pacings were performed, and the pacing site was altered every 6 minutes. After 4 minutes of a given pacing, 54 unipolar electrograms distributed over the entire cardiac surface were recorded. Next, refractory periods at electrode sites near pacing electrodes were measured. Paired right ventricular/left ventricular (RV/LV) pacing data were obtained six or seven times in each sample. Although the QRST isoarea maps during the two activation orders were qualitatively similar, it was recognized consistently from the right ventricle-left ventricle difference map that leads around the RV free wall had positive values and that leads around the LV free wall and apex had negative values. Compared with the same leads at RV and LV pacing, QRST areas were larger when pacing sites were near the leads. The local QRST areas of individual leads at which we measured local refractory period were consistently larger during drive from proximal pacing sites than during drive from distant pacing sites. Refractory periods were consistently longer during proximal pacing than during distal pacing, and there was a positive correlation between change in local QRST area and change in refractory period (r=0.64) during altered activation sequence, whereas there was an inverse correlation between change in QRST area and change in refractory period (r= -0.91) during localized myocardial warming. Conclusions. Both local QRST areas and local refractory periods were dependent on the activation sequence, and there was a positive correlation between QRST areas and refractory periods during various activation sequences compared with localized myocardial warming. (Circulation 1991;84:1346-1353) R) ecently, the body surface distribution of OQRST area has been reported to be a useful parameter in evaluating cardiac states at high risk of ventricular arrhythmiasl-4 and in diagnosing myocardial infarction in the presence of intraventricular conduction disturbances.5-7 The basis for these findings is that QRST area reflects local recovery properties and is largely independent of ventricular activation sequence. QRST areas have been postulated to depend on differences in the durations of intrinsic ventricular From the First Department of Internal Medicine, Yamagata University School Of Medicine, Yamagata, Japan. Supported in part by grants from the Mochida Memorial Foundation for Medical and Pharmaceutical Research and the Uehara Memorial Foundation. Address for correspondence: Kanji Hanashima, MD, Nora Eccles Harrison Cardiovascular Research and Training Institute (CVRTI), Building 500, University of Utah, Salt Lake City, UT 84112. Received August 29, 1989; revision accepted May 7, 1991. recovery properties.8 Direct evidence for this relation was shown by Abildskov et al.9 By measuring QRST areas in cardiac surface electrograms of dogs and determining their relation to changes of refractory period induced by localized warming, Abildskov et al showed that changes in QRST areas were inversely correlated with changes in refractory periods. In their study, Abildskov et a110"11 also found that the QRST area was largely but not entirely independent of ventricular activation sequence. In addition, small but definite changes in QRST area with differing activation sequences have been reported in some studies.12-'4 Previous studies15-17 have also shown that there are small but significant alterations of recovery properties resulting from different electrotonic interactions during various activations. The purpose of the present study was to investigate the effects of activation sequence on cardiac surface QRST distributions and to define the relation between local QRST area and local refractory period Hanashima et al Effect of Activation Sequence with alterations of activation sequence. These data are essential for understanding the effects of body surface QRST area distributions in the evaluation of heart diseases with intraventricular conduction disturbance. Downloaded from http://circ.ahajournals.org/ by guest on June 15, 2017 Methods Experiments were performed on 15 dogs initially anesthetized with 30 mg/kg i.v. sodium pentobarbital. An intravenous infusion of 500 ml 0.9% NaCl in H20 containing 200 mg pentobarbital was also given slowly over the 3- or 4-hour duration of each experiment. The large anesthetic dose has been shown to reduce spontaneous variation of ventricular repolarization properties, probably by reducing fluctuations of autonomic nerve tone.9 Under artificial ventilation, the thorax was opened in the fifth intercostal space, and the pericardium was incised to form a cradle supporting the heart. The sinus node was crushed. Bipolar stainless-steel hook electrodes with 1.5-mm separation of poles were used to deliver basic driving stimuli. They were attached to the right atrium and the free walls of the right and left ventricles. The heart was paced at a cycle of 400 msec with a 2-msec square-wave stimuli at twice diastolic threshold intensity. An array of 54 fine silver wire (0.005-in.-diameter) unipolar electrodes, insulated except at their point of attachment and mounted on a nylon sock, was stretched over the heart and anchored near the pericardial reflection. The electrode array had six rows (1-6) and nine columns (A through I). Rows 1-6 were located around the heart from the apex to the base (Figure 1). All recording electrodes were referenced to a Wilson central terminal and sampled every 2 msec using a multiplexed data recording system (CD-0055, Chunichi Denshi, Nagoya, Japan). To minimize beat-to-beat variations in the electrograms, all recordings were obtained with the respirator held in full expiration. The thoracic incision was covered with a clear polyethylene sheet, which was attached to the edges of the wound. A surgical lamp was directed over the thorax to maintain the cardiac surface temperature at 35 ±0.5°C. The left ventricular pressure was monitored so that suitable hemodynamic conditions could be maintained. Altered Activation Protocol Right ventricular (RV) and left ventricular (LV) pacings were performed during each experiment. The ventricular pacing site was changed every 6 minutes, and pairs of RV/LV pacing data were obtained six or seven times. The right atrium was paced simultaneously with the right or left ventricle to avoid retrograde atrial activation. After 4 minutes of a given ventricular pacing, all unipolar electrograms were recorded simultaneously in all dogs. Then, in 11 dogs (dogs 5-15), refractory periods at two sites (two epicardial sites, dogs 5 and 6) or at three sites (two epicardial sites and one endocardial site, dogs 7-15) were measured before changing to the other ventricular pacing. A B P QRST Area and RP 1347 D H I H I GH I on C E F G 6 *1~ 4 "\,-\ ell,p %~~~~~~~fl. \ 2 I ' LV / 1 R B 4 B C D E F B C D E F G - J \ ~~~~~~ 4 \ 4-'I '4 \.4~~~~9 1 l- - 2 1 C p B C D E F G H I A B C D E F G H I A B C D E F G H I 6 5 4 4. 1 FIGURE 1. Cardiac surface QRST isoarea maps from dog 7 during right ventricular pacing (panel A) and left ventricular pacing (panel B) and difference map (panel C) constructed from subtracting panel B from panel A. *Site of pacing. Although QRST isoarea maps during two activation orders are qualitatively similar, in the difference map positive and negative areas are located over right and left ventricles (RV and LV), respectively. Electrode array had six rows (1-6) and nine columns (A through I), and rows 1-6 were located around heart from apex to base. Intervals of contour line are 200 mV. msec. LAD, left anterior descending coronary artery; 0, zero line. QRSTArea Calculating The root-mean-square voltages of all 54 epicardial leads plotted against time were used to assist in manually selecting the onset of QRS and the end of the T wave. QRST areas were calculated by integrating each electrogram over the QRST interval. In this calculation, areas below the baseline were treated as negative. The right atrium was paced simultaneously 1348 Circulation Vol 84, No 3 September 1991 Downloaded from http://circ.ahajournals.org/ by guest on June 15, 2017 with either ventricle, and the P waves were a small constant value included in QRST areas during both RV and LV pacing. The activation time at each electrode site was computed from the minimum derivative of the QRS, which was time-referenced to the pacing stimulus. procedure was repeated. A period of 5 minutes of warming at each light intensity was allowed, after which the electrocardiogram was recorded during simultaneous pacing of the atrium and either the right or left ventricle. The refractory period was determined after each electrogram was recorded. Refractory Period Measurement Sites. After recording the electrograms, we measured refractory periods at two epicardial sites (leads RV and LV) in two dogs (dogs 5 and 6) and at two epicardial sites and one left ventricular endocardial site (lead LVE) in nine dogs (dogs 7-15). The lead RV was located 5-10 mm from the RV pacing site. The lead LV was located 5-10 mm from the LV pacing site. When we selected the two electrodes, we did not consider polarity of the QRST area. The electrode of lead LVE used for measurement of refractory periods was constructed from 0.005-in.-diameter stainless-steel, Teflon-coated wire. The insulation was stripped from one end of the wire, which was formed in a hook. This plunge electrode was placed approximately opposite the lead LV by means of a 26-gauge needle. Procedure. Constant-current, 2-msec, cathodal stimuli at 1.5-fold diastolic threshold intensity were delivered to the test site after every 10th basic RV or LV pacing stimulus. Initially, the interval between the 10th driving stimulus and the premature stimulus was shorter than that required for a propagated response. This interval was increased by steps of 1 msec until the earliest propagated response occurred. The difference between this interval and the activation time of the test site was taken as the refractory period. Localized Myocardial Warning Study In six of the 15 dogs (dogs 10-15), we examined the effects of localized myocardial warming on local QRST areas and local refractory period after completion of the former protocol. This examination was performed to confirm the finding of previous reports.912 We used the same protocol they used and examined correlations between actual value of QRST area and actual value of refractory period and between change in QRST area and change in refractory period. The electrodes, which had been placed at RV and LV free walls in the previous part of the experiment, were used to deliver stimuli for ventricular pacing. The electrode for recording electrograms and determining refractory periods was one of the 54 electrodes mounted on the sock. It was on the anterior surface near the septum and was selected because it was easily warmed by directing a light beam on it. Warming (up to 42°C) was produced by a lamp directed through a condenser lens assembly and a circular aperture so that a 20-mm-diameter light spot was centered on the electrode. Electrograms were recorded and refractory periods were measured at seven levels of light intensity. The ventricular pacing site was changed, and this Statistical Analysis Average data of six or seven measurements with paired RV/LV pacing in each dog were analyzed with a paired t test. Data were expressed as mean+SD, and a paired t test was used to assess significance of difference. Probability values of less than 0.05 were considered to indicate a significant difference. The least-squares method of linear regression analysis was used to determine the correlation coefficient between actual values of local QRST area and local refractory period and changes in local QRST area and local refractory period. Results Altered Activation Sequence Study The QRST areas (n=15 dogs) and refractory periods (n = 11 dogs) for different ventricular pacings are summarized in Table 1. The effects of altered activation sequence on QRST areas (in 15 dogs) and refractory periods (in 11 dogs) were similar to each other dog's data pattern. QRST areas were larger at leads RV and LV during proximal pacing than during pacing at a distance. Refractory periods were longer at leads RV, LV, and LVE during proximal pacing than during pacing at a distance. QRSTArea Distribution of Maps Figure 1, which is a representative example from dog 7, shows cardiac surface QRST isoarea maps during RV pacing (Figure 1A) and LV pacing (Figure 1B) and the difference map (Figure 1C) constructed by subtracting the map in Figure 1B from the map in Figure 1A. A star indicates the site of pacing. Although the QRST isoarea maps during the two activation orders were qualitatively similar, in the difference map there were positive and negative areas mainly over the right and left ventricles, respectively. This distribution of positive and negative areas was consistent in all of the difference maps. QRST Areas During RV and L V Pacing Figure 2 (data from dogs 1-15) shows pairs of average values of QRST areas for RV and LV pacing at lead RV (Figure 2A) and lead LV (Figure 2B). The QRST area at lead RV was 665.7±358.9 mV* msec during RV pacing and 69.7±+413.9 mV * msec during LV pacing. When paired data were analyzed, the QRST area increased 596.0±420.8 mV* msec at the lead RV when the drive was moved from the left ventricle to the right ventricle. This was significant for a probability of less than 0.01. The QRST area at lead LV was 52.5±+439.2 mV * msec during RV pacing and 710.9+389.2 Hanashima et al Effect of Activation Sequence on QRST Area and RP 1349 TABLE 1. Summary of Data Dog 1 2 3 4 5 6 7 Downloaded from http://circ.ahajournals.org/ by guest on June 15, 2017 8 9 10 11 12 13 14 15 n 6 6 6 6 7 7 7 7 6 6 6 6 6 6 6 6 6 6 6 6 6 6 6 6 6 6 6 6 6 6 6 6 6 6 6 6 Lead RV LV RV LV RV LV RV LV RV LV RV LV RV LV LVE RV LV LVE RV LV LVE RV LV LVE RV LV LVE RV LV LVE RV LV LVE RV LV LVE 6 6 RV LV 6 LVE QRST area (mV* msec) RV pacing LV pacing 516 115 -19 535 576 234 -183 287 180 -454 -448 192 1,032 792 13 468 1,324 367 803 1,315 393 1,042 723 1,070 916 667 348 610 . 449 188 38 368 . . 331 12 -87 382 189 164 -222 366 . . . . . . 641 297 404 721 . . 181 352 92 959 785 -96 -463 1,440 . . . . 978 -707 -263 964 845 -660 -568 986 ... ... Refractory period (msec) RV pacing LV pacing . . . . . 149.2 133.2 164.3 158.8 182.2 174.7 195.3 175.9 154.8 171.6 158.4 158.3 162.3 160.8 139.4 176.9 158.8 149.1 160.4 168.9 147.1 171.0 170.9 141.3 172.8 151.6 159.3 165.9 135.4 140.0 141.0 162.0 177.0 186.5 200.2 164.5 169.7 176.4 155.0 162.7 166.0 157.6 146.9 179.9 155.4 163.8 164.1 160.0 150.4 173.8 167.7 152.0 178.1 149.2 165.1 168.8 183.4 168.3 191.8 178.3 176.6 199.1 Values are averages from measurements. n, Number of measurements; RV, right ventricle; LV, left ventricle; LVE, left ventricular endocardium; RV pacing, right ventricular epicardial pacing; LV pacing, left ventricular epicardial pacing; lead RV, lead near LV pacing site; lead LV, lead near RV pacing; lead LVE, lead on left ventricular endocardium opposite lead LV. mV * msec during LV pacing. When paired data were analyzed, the QRST area increased 658.4+515.0 mV * msec at the lead LV when the drive was moved from the right ventricle to the left ventricle. This was significant for a probability of less than 0.01. Refractory Periods During RV and LV Pacing Figure 3 (data from dogs 5-15) shows pairs of average values of refractory periods for RV and LV pacings at lead RV (Figure 3A) and lead LV (Figure 3B). The refractory period at lead RV was 165.9+11.5 msec during RV pacing and 158±13.4 msec during LV pacing. When paired data were analyzed, the refractory period increased 7.6±6.4 msec at the lead RV when the drive was moved from the left ventricle to the right ventricle (p<0.01). The refractory period at lead LV was 161.4±+13.5 msec during LV pacing and 153.1±+12.5 msec during RV Circulation Vol 84, No 3 September 1991 1350 A B lead RV lead LV msec 301 1500 1500- r= 0.64 1000- 1000 - 0 20 - n 0 0- E a: 10500 500- - 0 0 co 0 a) -1 0- I0- -10 - La C 0 0 0 0 0 0 o -500 - -1000 - -1000 n=-15 n=15 pacing site RV LV pacing site Downloaded from http://circ.ahajournals.org/ by guest on June 15, 2017 FIGURE 2. Bar graphs of average values in each experiment of QRST areas at leads RV (panel A) and LV (panel B) during right and left ventricular pacings in dogs 1-15. QRST area at lead RV during right ventricular pacing was significantly larger than that during left ventricular pacing, and QRST area at lead LV during left ventricular pacing was significantly larger than that during right ventricular pacing. RV, right ventricle; LV, left ventricle. pacing. When paired data were analyzed, the refractory period increased 8.3+4.2 msec at the lead LV when the drive was moved from the right ventricle to the left ventricle (p<0.01). Correlation Between QRST and Refractory Period Figure 4 shows the relation between change in QRST area (A QRST) and change in refractory period (A RP) (dogs 5-15). The values are averages of six measurements during each drive; there was a positive correlation between them (r=0.64). However, there was no correlation between actual values lead LV B lead RV A 1801 180 170 0 -v 2_ [l -2000 - n= 22 1000 0 1000 2000 mVmsec delta QRST FIGURE 4. Scatterplot of relation between change in QRST area (delta QRST) and change in refractoy period (delta RP) from average values in each experiment (dogs 5-15). There was a positive correlation (r = 0.64). Regression line: y=0.0071x-0.23; y, delta RP; x, delta QRST. of QRST ods using areas and actual values average values from six of refractory perimeasurements. Refractory Period of LV Endocardial Lead The LV endocardial lead (lead LVE) was placed approximately opposite the lead LV, which was on the LV free wall. The refractory period (average values from six measurements in each experiment, dogs 7-15) at lead LVE was 178.5-+±13.1 msec during LV pacing and 174.2±+12.1 msec during RV pacing. When paired data were analyzed, the refractory period at the lead LVE increased 4.3+± 1.5 msec when the drive was moved from the right ventricle to the left ventricle (p<0.01) (Figure 5A). Although the site at lead LVE always had a longer refractory period than the site at lead LV, the difference was always less during LV pacing than during RV pacing. The difference was 19.5±11.1 msec during RV pacing and 14.7±11.9 msec during LV pacing. When paired data were analyzed, the difference decreased 4.7±4.0 msec when the drive was moved from the right ventricle to the left ventricle (p<0.01) (Figure 5B). E Go .c 160 ._ 0) a) >, 150- ci as 140- aD 1 1301 n=l1 RV LV pacing site n=1 1 RV LV pacing site FIGURE 3. Bar graphs of average values in each experiment ofrefractory periods at leads RV (panel A) and LV (panel B) during right and left ventricular pacings in dogs 5-15. Refractory period at lead RV during right ventricular pacing was significantly longer than that during left ventricular pacing, and refractory period at lead LV during left ventricular pacing was significantly longer than that during right ventricular pacing. RV, right ventricle; LV, left ventricle. Correlation Between QRSTArea and Refractory Period During Localized Myocardial Warming We measured refractory period in six dogs (dogs 10-15) during localized myocardial warming. We calculated the correlation coefficient of actual QRST with actual refractory period and the correlation coefficient of A QRST with A RP. Data from both RV and LV pacings with seven light intensity levels were analyzed. There were high negative correlation coefficients between QRST area and refractory period with increasing light intensity during pacing of a given site. However, the correlation between QRST area and refractory period with increasing warming was not as good as if data during pacings of both sites were considered together. Correlation coefficient between actual QRST and actual refractory period varied between -0.40 and -0.98 (average, -0.74). Hanashima et al Effect of Activation Sequence on QRST Area and RP A lead LVE 200 _ _ 190 0 E 0 B _ 50- lead LVE-lead LV ES between A QRST and A RP that we found with altered activation sequence (Figure 4). 0o Discussion Local QRST Area During Altered Activation Sequence The present study demonstrated that cardiac surface QRST was not totally independent of ventricular activation sequence. The QRST area during drive from a near site was consistently larger than that during drive from a distant site. Abildskov et a110 recorded body surface QRST isoarea maps of a dog during ventricular drive from the left and right ventricles via catheter-mounted stimulating electrodes and found that peak areas were displaced slightly toward the stimulating electrodes. Their finding is supported by our cardiac surface QRST area results. 40- 0. 30 0 180- a " 0 0 0 0 10 170- " a2 0 160 150n=9 - LV pacing site RV 1351 RV LV pacing site n=9 Downloaded from http://circ.ahajournals.org/ by guest on June 15, 2017 FIGURE 5. Panel A: Bar graph of refractory periods (average values in each experiment for dogs 5-15) at lead LVE during right and left ventricular pacing. Refractory period was significantly longer during left ventricular pacing than during right ventricular pacing. Panel B: Bar graph of difference in refractory period at leads LVE and LVduring right or left ventricular pacing. Average values in each experiment (dogs 5-15) were plotted. Difference was significantly less during left ventricular pacing than during right ventricular pacing. QRST area is realized as difference in refractory period between endocardium and epicardium. Although difference in refractory period at left ventricular endocardium and epicardium decreased during left ventricular pacing compared with during RV pacing, QRST area on left ventricular epicardium (lead LV) was larger during left ventricular pacing than during right ventricular pacing (Figure 2). QRST area change during altered activation sequence was not explained by the relation between endocardial and epicardial recovery properties. RV, right ventricle; LV, left ventricle; LVE, left ventricular endocardium. Correlation coefficient between A QRST and A RP varied between -0.84 and -0.97 (average, -0.91). There was a high inverse relation between A QRST and A RP. Figure 6 shows an example of the relation between A QRST and A RP (r= -0.96) (dog 15). This is inverse compared with the positive correlation localized myocardial warming Local Refractory Period During Altered Activation Sequence We also found that refractory periods were altered by activation sequence. At any lead (RV, LV, or LVE), the refractory period during drive from a near site was consistently longer than that during drive from a distant site. These changes of refractory periods between RV and LV pacings can be explained by different electrotonic interactions during the various activation sequences.15-17 During repolarization, the ventricular site at which the depolarization wave starts can be expected to receive a depolarization effect from surrounding tissue, and the site at which a depolarization wave terminates can be expected to receive a repolarization effect from surrounding tissue. Therefore, ventricular pacing would be expected to prolong the duration of the action potential in the region near the pacing site and to shorten it in the region far from the pacing site. Such an electrotonic interaction can also explain other observations: the longer refractory periods at both LV epicardium and LV endocardium during LV pacing than during RV pacing and the larger change in refractory periods between RV and LV pacing at LV epicardium compared with LV endocardium. 101 r 0- -0.96 0 ._ -10- 0 to E -20- 0. a_30 D -40s -h;u -%JV l5 -1000 n=14 _ 2000 0 1000 delta QRST (mV msec) 3000 FIGURE 6. Representative scatterplot of relation between x (change in QRST area, delta QRST) and y (change in refractory period, delta RP). There was an inverse correlation. Regression line: y= -0.022x-3.3. Relation Between QRST Area and Refractory Period Localized myocardial warning. In experiments in which myocardium was warmed, Abildskov et a19 found an inverse relation between QRST area and refractory period. They attributed this to the theory that the QRST area is determined by the difference between recovery properties at the electrode site and those in the remainder of the ventricles. A regional decrease (increase) of refractory period follows the proportional increase (decrease) of QRST area at that region. We confirmed this negative correlation between QRST areas and refractory periods using a method similar to that of Abildskov. Altered activation sequence. In contrast to the relation of change in QRST area to change in refractory period with localized myocardial warming, this neg- 1352 Circulation Vol 84, No 3 September 1991 Downloaded from http://circ.ahajournals.org/ by guest on June 15, 2017 ative relation does not hold true between changes of QRST area and refractory period during altered activation sequence. There was a positive correlation (r=0.64) between A QRST and ARP (Figure 4). During localized myocardial warming, recovery property should change only at local myocardium, whereas during altered activation sequence, recovery properties of varied myocardium were expected to have an influence. We must consider the interaction between recovery properties at local sites and those around local sites. Refractory periods at endocardium and epicardium. The relation of QRST area and refractory period to altered activation sequence is not explained by only local recovery property. A decrease in QRST area would be expected if the LV epicardial refractory period was the only factor involved. QRST area increased during proximal pacing despite the fact that the refractory period increased during proximal pacing. Therefore, we examined the relation between LV epicardial and endocardial refractory periods (dogs 7-15). We speculated that the refractory period difference between LV endocardium and LV epicardium would increase during pacing at LV epicardium; however, the result was the opposite (Figure 5B). The resulting QRST area during proximal pacing could not be explained by the relation between LV endocardial and epicardial refractory periods. QRST area on cardiac or body surface has been thought to be the difference between endocardial and epicardial action potential configuration (polarization). QRST area could be the difference between endocardial and epicardial action potential durations when the magnitude of action potential does not change. If amplitude of action potential above baseline changed, this might explain the fact that QRST area increases with proximal pacing. Measurement of action potential at some leads around the pacing site will be necessary. Definition of local site affecting electrocardiogram on an electrode. QRST area on a electrode is theoretically equal to the difference between recovery property at the local site and that in the remainder of the ventricle. We measured refractory period at a lead only 0.5-1.0 cm from the pacing site to assess recovery property at the local site. However, we believe that recovery property at a local site affecting an electrocardiogram on an electrode is a sum of recovery property around the electrode site. It is unknown how widely epicardium around the electrode affects QRST area as local site information. If QRST area was constructed from the difference between the sum of the polarization around an electrode and the remainder of the ventricle, it would be possible for QRST area to be larger during proximal pacing. Further investigation measuring many leads of refractory periods around the pacing site is necessary. Study Limitations In the present study, global QRST area findings were not compared with global recovery property because of the difficulty of measuring refractory periods from many leads in the few critical minutes available. However, a proper investigation of global change in recovery property would use other parameters (e.g., activation recovery time). In the present study, we could not find a direct mechanism to explain the different effects of localized myocardial warming and altered activation sequence on the relation between QRST area and refractory period. Further investigation, which should include observations of the changes of action potential configuration during varied activation sequences, and many measurements of recovery properties at many sites in the free wall of the ventricles around the pacing site are necessary. Clinical Significance The present study does not necessarily deny the clinical usefulness of QRST areas for the assessment of heart diseases; we found the cardiac surface QRST isoarea maps during RV and LV pacings to be qualitatively similar, as reported in previous studies.9,1" However, the relation between QRST areas and refractory periods following altered activation sequence must be taken into account. For example, if there is a local myocardial region with prolonged refractory period and corresponding decreased QRST area during normal activation, the ectopic rhythm occurring within the region may further increase the refractory period yet normalize the QRST area. In conclusion, there was a paradoxical relation between QRST areas and refractory periods during altered activation sequence. When we use body surface QRST areas in the evaluation of ventricular recovery properties, transmural and neighboring epicardial as well as local epicardial refractory periods must be considered. References 1. Urie PM, Burgess MJ, Lux RL, Wyatt RF, Abildskov JA: The electrocardiographic recognition of cardiac states at high risk of ventricular arrhythmias: An experimental study in dogs. Circ Res 1978;42:350-358 2. Garedner MJ, Montague TJ, Armstrong CS, Horacek BM, Smith ER: Vulnerability to ventricular arrhythmia: Assessment by mapping of body surface potentials. Circulation 1986;73:684-692 3. Ambroggi DL, Bertoni T, Locati E, Stramba-Badiale M, Schwarty PJ: Mapping of body surface potentials in patients with the idiopathic long QT syndrome. Circulation 1986;74: 1334-1345 4. Yasumura S, Kubota I, Ikeda K, Tsuiki K, Yasui S: Using body surface mapping to detect vulnerability to ventricular arrhythmias in patients with coronary artery disease. J Electrocardiol 1987;20:114-120 5. Kubota I, Ikeda K, Yamaki M, Watanabe Y, Tsuiki K, Yasui S: Determination of the left ventricular asynergic site by QRST isointegral mapping in patients with myocardial infarction. Jpn Heart J 1984;25:311-324 6. Igarashi A, Kubota I, Ikeda K, Tsuiki K, Yasui S: Determination of the site of myocardial infarction by QRST isointegral mapping in patients with abnormal ventricular activation sequence. Jpn Heart J 1987;28:165-176 Hanashima et al Effect of Activation Sequence 7. Hirai M, Burgess MJ, Haws CW: Effects of coronary occlusion on cardiac and body surface PQRST isoarea maps of dogs with abnormal activation simulating left bundle branch block. Circulation 1988;77:1414-1423 8. Wilson FN, Macreod AG, Barker PS, Johnston FD: The determination and significance of the areas of the ventricular deflections of the electrocardiogram. Am Heart J 1934;10: 46-61 9. Abildskov JA, Evans AK, Lux RL, Burgess MJ: Ventricular recovery properties and QRST deflection area in cardiac electrograms. Am J Physiol 1980;239:H227-H237 10. Abildskov JA, Burgess MJ, Urie PM, Lux RL, Wyatt RF: The unidentified information content of the electrocardiogram. Circ Res 1978;43:899-907 11. Abildskov JA, Burgess MJ, Millar K, Wyatt R: New data and concepts concerning the ventricular gradient. Chest 1970;58: 244-248 12. Burgess MJ, Lux RL, Wyatt RF, Abildskov JA: The relation of localized myocardial warming to changes in cardiac surface electrograms in dogs. Circ Res 1978;43:899-907 on QRST Area and RP 1353 13. Cosma J, Levy B, Pipberger HV: The spatial ventricular gradient during alterations in the ventricular pathway. Am Heart J 1966;71:84-91 14. Simonson E, Schmitt OH, Dahl J, Fry D, Bakken EE: The theoretical and experimental basis of the frontal plane ventricular gradient and its spatial counterpart. Am Heart J 1954;47:122-153 15. Abildskov JA: Effects of activation sequence on the local recovery ventricular excitability in the dog. Circ Res 1976;38: 240-243 16. Toyoshima H, Burgess MJ: Electrotonic interaction during canine ventricular repolarization. Circ Res 1978;43:348-356 17. Osaka T, Kodama I, Tsuboi N, Toyama J, Yamada K: Effects of activation sequence and anisotrophic cellular geometry on the repolarization phase of action potential of dog ventricular muscles. Circulation 1987;76:226-236 KEY WORDS * QRST mapping * ventricular recovery Downloaded from http://circ.ahajournals.org/ by guest on June 15, 2017 Effect of altered activation sequence on epicardial QRST area and refractory period in dogs. K Hanashima, I Kubota, T Ozawa, T Shibata, M Yamaki, K Ikeda and S Yasui Downloaded from http://circ.ahajournals.org/ by guest on June 15, 2017 Circulation. 1991;84:1346-1353 doi: 10.1161/01.CIR.84.3.1346 Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1991 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7322. Online ISSN: 1524-4539 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circ.ahajournals.org/content/84/3/1346 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation is online at: http://circ.ahajournals.org//subscriptions/