Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Cardiovascular disease wikipedia , lookup
Remote ischemic conditioning wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Electrocardiography wikipedia , lookup
Cardiac surgery wikipedia , lookup
Jatene procedure wikipedia , lookup
Coronary artery disease wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Antihypertensive drug wikipedia , lookup
AF
9th October 2013
Dr Julian Tomkinson
Introduction
NICE Guidance 2006
“Atrial fibrillation (AF) is the most
common sustained cardiac arrhythmia
and if left untreated is a significant risk
factor for stroke and other
morbidities”
Why is AF Important?
• AF prevalence rate in primary care is 1.2%
600,000 in England alone
• Atrial fibrillation predisposes patients to stroke, increasing
stroke risk by 500-700%
• 12,500 strokes per year (of the 150,000 total) attributable
to AF
• – 4,300 deaths in hospital
• – 3,200 discharges to residential care
• – 8,500 deaths within the first year
DH Figures 2007
Consequences
Loss of active ventricular filling :
• Stagnation of blood in the atria leading to
thrombus formation and a risk of embolism,
increasing the risk of stroke.
• Reduction in cardiac output (especially during
exercise) which may lead to heart failure.
Type of AF
• Paroxysmal (subsides within 48 hours)
• Persistent ( >7days)
• Permanent (> 1 year)
Aetiology
• Idiopathic ('lone') atrial fibrillation
(AF): 5-10% of patients (diagnosis
of exclusion with no evidence of
any specific underlying cause).
• Hypertension (especially with
associated left ventricular
hypertrophy).
• Coronary artery disease.
• Valvular heart disease, especially
mitral valve stenosis.
• Cardiac surgery.
• Myocarditis.
• Atrial septal defect.
• Atrial myxoma.
• Sick sinus syndrome.
• Pre-excitation syndromes, eg WPW
• Dilated and hypertrophic
cardiomyopathy.
• Pericardial disease, eg pericardial
effusion, constrictive pericarditis.
• Hyperthyroidism.
• Acute infections (especially
pneumonia in the elderly).
• Acute excess alcohol intake or
chronic excess alcohol intake.
• Respiratory (lung cancer, COPD,
pleural effusion, PE, pulmonary
hypertension).
• Obesity, sleep apnoea,
haemochromatosis, sarcoidosis, and
narcotic abuse
• Genetic: autosomal dominant
Detection
•
•
•
•
•
Breathlessness
Palpitations
Syncope/dizziness
Chest discomfort
Stroke/TIA
manual pulse palpation should be performed to
assess for the presence of an irregular pulse that
may indicate underlying AF
Detection
Opportunistic
20% asymptomatic
Patients Attend for Many Reasons
•
•
•
•
Medication reviews
Chronic Illness monitoring
Flu vaccination
Just for a chat
OPPORTUNITY TO CHECK PULSE
Making the Diagnosis
ECG
Benefits
• Symptom Control
• Reduce Strokes, mortality, morbidity
• Reduce Cost to patients, families,
social care, PCTs, NHS…………..
150,000 strokes per year in the UK
• 410 per day
• 17 per hour
• Within the next four hours, 10 patients with AF will
have suffered a stroke
• 8 would have been known to be high risk of stroke
• 6 should have been on warfarin
• 3 will go home
• 5 will end up in residential care
• 2 will die....
The Stroke Association: www.stroke.org.uk.
Scenario 1
Mrs April Fillingham
75 years old
Attends for Flu Jab
You take her pulse and it is irregularly irregular with
rate 84
WHAT DO YOU DO NEXT?
Scenario 1 (continued)
• Mrs F says she feels well generally
• Past history of COPD
• She gets breathless running upstairs but put
this down to COPD & age
• No chest pain
Scenario 1 (continued)
Mrs F attends for ECG and bloods
•
•
•
•
ECG shows AF rate 92
BP 136/87
FBC U+E’s TFTs glucose all ok
INR 1
Risk factors Mrs AF
•
•
•
•
No murmurs
No recent acute chest infections
Minimal alcohol intake
No signs of heart failure
Scenario 1 (continued)
What do you do now?
Explanation
How do you explain to a
patient they have AF?
Explanation
“Atrial fibrillation (AF for short) is a condition
that affects the heart, causing an irregular
pulse. It occurs when the electrical impulses
controlling the heartbeat become
disorganised, so that the heart beats
irregularly and too fast. When this happens,
the heart cannot efficiently pump blood
around the body”
NICE guide for patients
http://www.youtube.com/watch?v=wqau2_FQq1E
Useful resource
RCGP
Case Cards
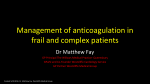
Management
Confirmed diagnosis of AF
Further investigations and clinical assessment including
risk stratification for stroke/thromboembolism
Paroxysmal AF
Persistent AF
Permanent AF
OR
Rhythm-control
Remains symptomatic
Failure of rhythm-control
Rate-control
Admission
• There is a very rapid pulse (greater than 150
beats per minute) and/or low blood pressure
(systolic blood pressure less than 90 mm Hg).
• There is loss of consciousness, severe
dizziness, on-going chest pain, or increasing
breathlessness.
• There is a complication of AF, such as stroke,
TIA, or acute heart failure.
Routine referral to a cardiologist
should be considered when:
• The person is young, eg less than 50 years of age.
• Paroxysmal AF is suspected.
• There is uncertainty regarding whether rate or
rhythm control should be used.
• Drug treatments that can be used in primary care are
contra-indicated or have failed to control symptoms.
• The person is found to have valve disease or left
ventricular systolic dysfunction on echocardiography.
• Wolff-Parkinson-White syndrome or a prolonged QT
interval is suspected on the electrocardiogram.
Rhythm control
• Preferred in:
• Patients with paroxysmal AF
• Patients with persistent AF who are:
– Symptomatic
– younger than 65 years
– presenting for the first time with idiopathic AF or
secondary AF or with congestive heart failure
It should be started after specialist assessment.
Rate Control
Rate control may be started in primary care and
is the preferred treatment when patients have:
• persistent AF
• are more than 65 years old
• have coronary artery disease
• have contra-indications for cardioversion or
anti-arrhythmic drugs.
Rate Control
• Ventricular rate control may be at least as
effective as restoration of sinus rhythm in
terms of survival and symptom control,
especially in elderly patients.[1]
Rate Control
• Measure on an ECG or at the ventricular apex, not the wrist
• Target below 80 beats per minute at rest and 90-115 on
moderate exercise.
• A heart rate-limiting calcium-channel blocker (e.g verapamil
or diltiazem) or a beta-blocker are recommended as firstline therapy for control of the ventricular rate.
• Digoxin may control the resting heart rate, but rarely
adequately controls heart rate during exertion and so
should only be considered as monotherapy in
predominantly sedentary patients. It may be added as a
second-line therapy.
• Often a combination of two drugs may be needed and, in
this case, digoxin can be combined with either a ratelimiting calcium-channel blocker or a beta-blocker.
Management
Rate Control:
You agree to start bisoprolol 2.5mg
daily
Indications for planned
cardioversion
•
•
•
•
•
Persistent AF
Unable to achieve adequate rate control
Symptoms despite rate control
Age < 65
Recent onset and reversible precipitant eg
chest infection
• Atrial Flutter
Management
CVA RISK?
NICE
2006
CHA2DS2-VASc
CHADS2
CHADS2 score
CVA rate per 100 pt years
0
1
2
3
4
5
6
1.9
2.8
4.0
5.9
8.5
12.5
18.2
CHADS2-NICE & QOF
CHADS2 score
0
1
>2
Drug of choice
none or aspirin
aspirin or warfarin
warfarin
European Society of Cardiology
CHAD2 score of 1 = no or possible anticoagulation
and a score > 1 = anticoagulation
Explanation
How would you explain the risks
of AF?
Anticoagulation
You would recommend warfarin
How do you have this
conversation?
Warfarin in lower risk patients
(1% per year)
Warfarin in moderate risk patients
(3.5% per year)
Warfarin in high risk patients
(6% per year)
http://sdm.rightcare.nhs.uk/pda/stroke-prevention-for-atrialfibrillation/introduction/
Shared Decision Making
Warfarin Issues
•
•
•
•
•
Risk of bleeding
Daily medication
Other side effects
Blood monitoring
Other drug interactions
NOAC
• Dabigatran (Pradaxa) 150 mg bd is more effective
than warfarin in reducing the risk of stroke or
systemic embolism, ischaemic stroke and vascular
mortality
• Rivaroxaban (Xarelto) 10 mg daily
Dabigatran
• It does not require monitoring.
• Compared with warfarin, overall risk of life-threatening
bleeds is reduced but there is an increased risk of a GI bleed.
• NICE suggests it can be used in patients with non-valvular AF
with one or more of the following risk factors
– previous stroke, TIA or systemic embolism, left ventricular
ejection fraction below 40%, symptomatic heart failure (NYHA
class 2 or above)
– age 75 years or older or age 65 years or older with diabetes,
coronary artery disease or hypertension.
• It can also be used in those patients with a poorly controlled
INR currently on warfarin.
• Dabigatran 110 mg bd is appropriate for patients aged 80
years and above.
Rivaroxaban
• It does not require monitoring.
• NICE suggests it can be used in patients with
non-valvular AF with one or more risk factors
such as
– congestive heart failure, hypertension, age 75 years
or older, diabetes mellitus, prior stroke or TIA.
• It can also be used in those patients with a
poorly controlled INR currently on warfarin
Mr Chad Skorinski
76
Discharge letter received from hospital saying patient was discharged 2
weeks ago after developing a left sided hemiparesis
On admission he was noted to have
•
•
•
•
left sided hemiparesis
AF rate 72
BP 130/72
CT showed small infarct
Patient made good improvement with OT / physio input and almost fully
recovered function.
Commenced warfarin and bisoprolol 2.5mg od. Rate settle to 76 prior to
discharge. Please arrange echo and AF follow up. Stroke rehab to continue.
Mr Chad Skorinski
76
Phx
Diabetes 2002
Last encounter:
2/2/12
Diabetes review – ‘HBA1C 48 BP 130/80
Bloods ok, still maintaining good glycaemic control
on diet – review 12 months’
Issues
• Pulse checked before?
• Significant event
• Audit
•
•
•
•
•
Coding
Check anti-coagulant team involved?
Refer echo
Review Mr Skorinski
Diabetes check due
QOF Indicators for AF 2013-14
1. Establish and maintain a register of patients with AF
2. Percentage of patients with AF in whom stroke risk has been
assessed using the CHADS2 scoring system in the preceding
12 months (excluding those whose previous CHADS2 score is
greater than 1).
1. In those patients with AF in whom there is a record of a
CHADS2 score of 1 (latest in the preceding 12 months), the
percentage of patients who are currently treated with
anticoagulation drug therapy or antiplatelet therapy.
2. In those patients with AF whose latest record of a CHADS2
score is greater than 1, the percentage of patients who are
currently treated with anticoagulation therapy.
The target resting heart rate in rate
control management of AF is?
1.
2.
3.
4.
5.
6.
<120
<110
<100
<90
<80
<70
Persistent AF
1.
2.
3.
4.
5.
Subsides within 48 hours
Lasts for more than 48 hours
Lasts for more than 7 days
Lasts for more than 28 days
Lasts for more than 1 year
Which of the following statements
about Dabigatran is incorrect?
• It does not require monitoring
• It has a lower incidence of life-threatening bleeds
than warfarin
• It has a lower incidence of GI bleeds than
warfarin
• It should be used at a dose of 110mg bd in
patients over the age of 80
• It is not suitable for patients with valvular disease
AF