Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Saturated fat and cardiovascular disease wikipedia , lookup
Cardiovascular disease wikipedia , lookup
Heart failure wikipedia , lookup
Electrocardiography wikipedia , lookup
History of invasive and interventional cardiology wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Remote ischemic conditioning wikipedia , lookup
Jatene procedure wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
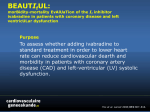
European Heart Journal Supplements (2015) 17 (Supplement G), G24–G29 The Heart of the Matter doi:10.1093/eurheartj/suv056 Ivabradine in the management of coronary artery disease with or without left ventricular dysfunction or heart failure Roberto Ferrari1,2* 1 Department of Cardiology and LTTA Centre, University Hospital of Ferrara and Maria Cecilia Hospital, GVM Care & Research, E.S. Health Science Foundation, Cotignola, Italy 2 Azienda Ospedaliero-Universitaria di Ferrara, Ospedale di Cona, Via Aldo Moro 8, 44124 (Cona) Ferrara, Italy KEYWORDS Left ventricular dysfunction; Heart failure; Coronary artery disease; Ivabradine Heart rate reduction is an integral part of antianginal therapy. In this article, we examine currently available data related to the use of ivabradine in patients with angina pectoris with and without left ventricular dysfunction (LVD) or heart failure (HF). We explore results from large morbidity–mortality trials of ivabradine in stable coronary artery disease (CAD) without HF (SIGNIfY), stable CAD with LVD (BEAUTIfUL), and systolic HF (SHIfT). While ivabradine did not improve outcomes in the main population in SIGNIfY, analyses of the antianginal effect of ivabradine in a pre-specified angina subgroup (n ¼ 12 049) were in line with knowledge of the antianginal properties of ivabradine, with improvements in angina class vs. placebo (P ¼ 0.01) and a trend towards less elective coronary revascularization (P ¼ 0.058). A post hoc analysis in a subgroup of 1507 BEAUTIfUL patients with limiting angina at baseline showed that risk reduction in favour of ivabradine, which was nominally statistically significant for hospitalization for myocardial infarction; the results were even better in patients with heart rate ≥70 b.p.m. Similarly, a post hoc analysis in 2220 SHIfT patients with angina at baseline indicated that the beneficial prognostic effects of ivabradine were maintained. The main differences between the three studies are LVD and ivabradine dosage (which was higher in SIGNIfY than in the other two trials). We conclude that heart rate reduction has a different role according to LVD. Provided that it is used at the recommended dose, ivabradine has been proved to be an effective, useful antianginal agent in patients with and without LVD. Introduction Heart rate reduction is an integral part of optimal antianginal therapy. The efficacy of heart rate reduction with the If inhibitor ivabradine in reducing the symptoms of angina pectoris in patients with stable coronary artery disease (CAD) with normal left ventricular (LV) function either alone or on top of beta-blockers is well documented1–3 and recognized by the European Guidelines.4,5 The recent * Corresponding author. Tel: +39 0532 239882, Fax: +39 0532 237841, Email: [email protected] Study assessInG the morbidity-mortality beNefits of the If inhibitor ivabradine in patients with coronarY artery disease (SIGNIfY) reported that the use of ivabradine in patients with normal LV function appeared to be associated with an increase in the incidence for primary composite endpoint in a pre-specified subgroup of 12 049 patients with Canadian Cardiovascular Society (CCS) class II or higher angina at baseline.6 Whatever the explanation for the results of SIGNIfY in terms of outcomes, analyses of the antianginal effect of ivabradine in the same angina subgroup were in line with the symptomatic use of ivabradine Published on behalf of the European Society of Cardiology. All rights reserved. & The Author 2015. For permissions please email: [email protected] Ivabradine in the management of CAD with or without LVD or HF in patients with stable angina pectoris. There were improvements in CCS angina vs. placebo (P ¼ 0.01) and a trend towards lower incidence of elective coronary revascularization (P ¼ 0.058).6 A substudy of SIGNifY evaluated the effects of ivabradine on angina-related quality of life in 4187 patients. The results indicate that ivabradine produces consistent improvements of self-reported quality of life parameters related to angina pectoris, notably in terms of angina frequency and disease perception.7 Thus, the antianginal effect of ivabradine in CAD patients with normal LV function is unquestionable. The scope of the present article is to examine currently available data related to the use of ivabradine in patients with angina and LV dysfunction or heart failure (HF), because, in these patients, ivabradine could provide symptomatic and prognostic benefits. To achieve this, we also need to examine data from the MorBidity-mortality EvAlUaTion of the If inhibitor ivabradine in patients with coronary disease and left ventricULar dysfunction (BEAUTIfUL) and Systolic Heart failure treatment with the If inhibitor ivabradine (SHIfT) trials.8,9 Patients with angina in BEAUTIfUL BEAUTifUL was an international, multicentre, randomized, double-blind, placebo-controlled, phase 3 study designed to evaluate cardiovascular (CV) outcomes in subjects with CAD and LV systolic dysfunction [LV ejection fraction (EF) ,40%] and heart rate ≥60 b.p.m.8 Subjects received ivabradine in combination with optimal, stable conventional CV medication, deemed appropriate for CAD or specific aspects of their presentations, as background therapy, e.g. beta-blockers (86.9%), aspirin (84.8%), angiotensinconverting enzyme (ACE) inhibitors (79.9%), statins (74.2%), diuretics (mineralocorticoid receptor antagonists, 27.1%; other agents, 58.9%), organic nitrates (43.4%), dihydropyridine (10.2%), and diltiazem or verapamil (2.3%). The study was designed to accrue 950 events of the primary composite endpoint, which was defined as the first event among G25 CV death, hospitalization of acute myocardial infarction (MI), or hospitalization for new or worsening HF. The main results of the BEAUTIfUL trial were neutral. There was no impact of ivabradine on outcomes: in the primary analysis in the randomized set of 10 917 subjects, ivabradine had no effect on the primary composite endpoint. However, in a pre-specified subgroup of subjects with baseline resting heart rate ≥70 b.p.m., there was a trend in the primary composite endpoint in favour of ivabradine. The opposite trend was observed in the subgroup or subjects with heart rate ,70 b.p.m. at baseline. In the subgroup with heart rate ≥70 b.p.m., ivabradine’s main impact was on coronary endpoints with the observation of a 36% relative risk reduction for hospitalization for fatal or nonfatal MI and a 30% relative risk reduction for coronary revascularization. These findings were attributed to differential effects of increased heart rate of CV outcomes with a direct effect on coronary outcomes, i.e. ischaemia or MI.8 Considering the value of ivabradine in the management of angina, a post hoc analysis was performed in a subgroup of BEAUTIfUL subjects with anginal pain as the limiting factor for physical activity at baseline (n ¼ 1507).10 The presence of angina at baseline was determined by New York Heart Association (NYHA) class II or III, whether they reported symptoms limiting activity, and whether those symptoms were noted as angina-related. This definition of limited angina was considered to be equivalent to CCS classes II and III angina. In this subgroup, the hazard ratios of the primary composite endpoint, all component endpoints, and all-cause mortality all favoured ivabradine, and the reduction in risk for hospitalization for acute MI was nominally statistically significant (Table 1, Figure 1A). Compared with placebo, the ivabradine group also had a lower incidence of all-cause mortality than placebo (8.7 vs. 10.0%, respectively), CV death (7.4 vs. 8.3%), and death due to acute MI (0.3 vs. 1.2%). In patients with limiting angina and heart rate ≥70 b.p.m., there was an even greater effect on coronary outcomes and treatment was associated with substantial reductions in hospitalization for fatal and non-fatal MI and coronary revascularization (Figure 1B). Table 1 Incidence of primary composite endpoint [cardiovascular death, hospitalization for acute myocardial infarction (MI), or hospitalization for new or worsening heart failure (HF)] and selected secondary endpoint in BEAUTIfUL subjects with angina pain at baseline Endpoint Primary composite endpoint Secondary endpoints Cardiovascular death Hospitalization for acute MI Hospitalization for new or worsening HF All-cause mortality Event rate, n(%) Hazard ratio E (95% CI)a P valueb Ivabradine N ¼ 734 Placebo N ¼ 773 88 (12.0%) 120 (15.5%) 0.76 (0.58–1.00) 0.05 54 (7.4%) 33 (3.8%) 33 (4.5%) 64 (8.7%) 64 (8.3%) 50 (6.5%) 41 (5.3%) 77 (10.0%) 0.88 (0.62–1.27) 0.58 (0.37–0.92) 0.84 (0.53–1.33) 0.87 (0.62–1.21) 0.51 0.021 0.45 0.41 CI, confidence interval (two-sided). a Estimate (E) of hazard ratio using an adjusted Cox proportional hazards model with beta-blocker intake at baseline as a covariate. b Log-rank test stratified on beta-blocker intake at randomization. G26 R. Ferrari Figure 1 Event curves for the primary composite endpoint of cardiovascular death, hospitalization for acute myocardial infarction, or hospitalization for new or worsening heart failure in patients with limiting angina (A) and in those with limiting angina and heart rate ≥70 b.p.m. (B) at baseline in the BEAUTIfUL study. HR, hazard ratio; CI, confidence interval. Reproduced from reference (10) with permission. We should consider these data in the light of the main results of the BEAUTIfUL study,8 in which there was no impact of ivabradine on the primary composite endpoint. This unexpected result was attributed to the domination of HF events in the primary composite endpoint. Patients with angina would be expected to have proportionately more coronary events—especially MI—and that would affect the primary composite endpoint. The BEAUTIfUL placebo group is informative on this point. Placebo patients with angina had higher rates of hospitalization for fatal and nonfatal MI than placebo patients in the whole study (6.5 vs. 4.2%, respectively; 6.3 vs. 4.9% in patients with heart rate ≥70 b.p.m.) and lower rates of hospitalization for HF (5.3 vs. 7.9%; and 5.5 vs. 10.1%). BEAUTIfUL was not designed to detect the symptomatic effects of ivabradine, and so it was not possible to establish whether treatment reduced the burden of angina pain, which could have explained the reduction of CV risk. This would have been in agreement with the literature reports that patients with angina symptoms are at higher risk for MI, whether they have stable angina, stable CAD, and independently of the presence of LV dysfunction.11–15 It remains unclear by which mechanism limiting angina predicts coronary events. The most probable explanation is related to the obstructive nature of coronary atherosclerosis. Indeed, the pain associated with ischaemia usually indicates a fixed obstructive lesion,14 whereas the progression of disease and acute coronary events are generally related to overall plaque burden, as well as the vulnerability and instability of plaque. Ivabradine’s beneficial effect on endothelial function has been demonstrated in animal models, which support the notion that it should attenuate the progression of atherosclerosis.16,17 While these mechanisms are attractive, they now appear unlikely to be relevant in humans since the SIGNIfY trial clearly demonstrated that ivabradine has no effect on CV death or MI in CAD patients with normal ventricular function, which implies no beneficial effect on atherosclerosis progression or plaque rupture.6 There are a number of differences between BEAUTIfUL and SIGNIfY. The most relevant to our discussion here is probably LV function, which was reduced in BEAUTIfUL and normal in SIGNIfY. This may explain—at least in part— the beneficial prognostic effect found in the angina subgroup of BEAUTIfUL.10 To this end, it is interesting to examine the patients enrolled in SHIfT with angina, since they also had LV dysfunction as well as HF.9 Patients with angina in SHIfT SHIfT included 6558 patients with chronic HF, resting heart rate ≥70 b.p.m. and baseline EF 29.0 + 5.1%, who were also receiving guideline-based background therapy.9 Treatment with ivabradine was associated with a highly significant effect on the primary composite outcome of CV death and hospitalization for HF. The effect was found to be mainly driven by HF hospitalization, the risk of which was reduced by 26% (P , 0.0001). There was no difference in the effect of ivabradine between ischaemic and nonischaemic HF, with a similar magnitude of risk reduction whatever the origin of HF. About a third of the SHIfT population (n ¼ 2220) had angina at entry to the study.18 Preliminary data reported at this year’s American College of Cardiology meeting demonstrated that effect of ivabradine was similar in patients in the whole SHIfT population and in the subgroup of 2220 patients with angina: ivabradine reduced CV death or hospitalization for worsening HF by 18% compared with placebo in the whole population [hazard ratio (HR), 0.82; 95% confidence interval (CI), 0.75–0.90; P , 0.0001] and by 15% in the patients with angina (HR, 0.85; 95% CI, 0.73– 1.00; P ¼ 0.0553). Ivabradine reduced CV death or non-fatal MI by 11% vs. placebo in the whole population (HR, 0.89; 95% CI, 0.79–1.01; P ¼ 0.0660) and by 8% (HR, 0.92; 95% CI, 0.75–1.12; P ¼ 0.3797) in the angina subgroup. Both groups showed directionally consistent results for non-fatal MI. Thus, it appears that SHIfT patients with angina and HF receiving ivabradine had the same benefit in terms of the primary composite endpoint as the overall SHIfT population. How to interpret the data The first point that needs to be made is that both of the evaluations in BEAUTIfUL and SHIfTon patients with angina are Ivabradine in the management of CAD with or without LVD or HF both post hoc, non-prespecified analyses. There is, however, a difference: BEAUTIfUL was a neutral study and so, from a purely statistical and procedural point of view, any sub-analyses have no validity and, actually, should not even be considered. This approach, although correct, is a bit drastic and, in every large trial, there is the temptation (and even a duty) to further dissect the data in the hope of finding interesting hypotheses or explanations for the results. This was the case for the post hoc exploratory analyses performed in BEAUTIfUL, which was subsequently tested in the SIGNIfY trial. The SIGNIfY trial, however, was not a pure replica of BEAUTIfUL in patients with heart rate ≥70 b.p.m., and ended up exploring the effect of a different regimen in quite a different population. The main differences between the two trials were the level of LV function (normal in SIGNIfY, reduced in BEAUTIfUL) and the higher initiation and maintenance dosage employed in SIGNIfY.6,8 It follows that the only argument that could be put forward for BEAUTIfUL angina10 is that the sample size was relevant (1507 patients with angina) and the results are plausible and in line with previous data for ivabradine in a pure angina population,2,3 but not with those of SIGNIfY.6 On closer inspection, the BEAUTIfUL patients with angina resemble more those enrolled in SHIfT, with a 32% EF in BEAUTIfUL and 29% EF in SHIfT, and the two trials share the same dose regimen. The results are also concordant since there was a reduction in primary composite endpoints with less hospitalization for HF in SHIfT vs. less hospitalization for MI in BEAUTIfUL. It would be interesting to make a meta-analysis of the two angina subgroups. Therefore, it seems that ivabradine improves prognosis in patient with LV dysfunction, suggesting an important role of heart rate reduction in relation to LV function.19 When ventricular function is reduced, the elevation of heart rate is closely associated with stroke volume, and its early increase could be considered as a compensatory mechanism. However, this is true only in the initial stages; prolonged neuroendocrine activation has deleterious effects on the myocytes resulting in ventricular changes for the worse and remodelling of the ventricle, a complex phenomenon whereby the ventricles progressively enlarge and EF reduces. Under these conditions, heart rate per se impacts on LV dysfunction with an increase in volumes and reduction in EF at higher rates, as shown in paced patients.20,21 As HF progresses, the force–frequency relationship by which the normal heart regulates cardiac function becomes negative and the compensatory mechanism of increased heart rate is lost; myocardial contractility no longer improves with increasing heart rate. On the contrary, it further deteriorates.22 The situation is further aggravated by a heart rate-associated increase in energy deprivation, inducing hypoxia, which stimulates local production of a range of cytokines, free radicals, and vasoconstrictors implicated in the development of LV remodelling. Of course, all of the processes are further exaggerated by the presence of angina causing short periods of ischaemia with further negative consequences on the myocytes. In stable CAD with maintained LV function, heart rate is a well-established determinant of ischaemia. In line with experimental data, clinical results indicate that elevations of G27 heart rate during physical or emotional stress induce ischaemia and angina.23 Consistent with this, heart rate reduction is a recognized strategy for the prevention of ischaemia and therefore of angina symptoms in patients with maintained24 or depressed LV function.25 Heart rate reduction with ivabradine has been demonstrated to improve angina symptoms since it reduces heart rate both at rest and on exercise, which is when ischaemia is most likely to occur. In line with this, a heart rate of 55 to 60 b.p.m. is currently recommended for optimal antianginal efficacy of beta-blockers and ivabradine in stable CAD.4 Furthermore, experimental and clinical data suggest that heart rate may be involved in the progression of atherosclerosis and plaque rupture leading to MI.26,27 This was the underlying rationale for the SIGNIfY study. The results of SIGNIfY6 confirm the symptomatic benefit of ivabradine, as shown by an improvement in angina class, but do not show a prognostic benefit. Conclusion Provided that it is used at the recommended dose, ivabradine has been proved to be an effective, useful antianginal agent in patients with preserved or reduced EF. The angina substudy of BEAUTIfUL and an analysis of SHIfT patients with angina at entry seem to support a prognostic benefit, but these data should be considered with caution as they are results of sub-studies, albeit in a relevant number of patients. The improvement of outcomes have never been shown to improve with an antianginal treatment in patients with stable angina pectoris. The effects of calcium channel blockade on CV mortality and morbidity were tested in CAMELOT (Comparison of AMlodipine vs. Enalapril to Limit the Occurrence of Thrombosis) and ACTION (A Coronary disease Trial Investigating Outcome with Nifedipine),26,27 but neither trial demonstrated a significant reduction in major CV events independently of LV dysfunction. The IONA (Impact Of Nicorandil in Angina) trial showed a trend,28 but was not powered to show a benefit on CAD mortality or non-fatal MI, and all-cause mortality and therefore we are unable to draw conclusions regarding effects on these endpoints. On the other hand, the benefits of beta-blockade in terms of reduction of mortality are well known, but are limited to post-MI and HF patients.29–32 Moreover, most of these post-MI trials with beta-blockers were performed before the era of thrombolysis or primary angioplasty with extensive use of ACE inhibitors and statins,4 which leaves uncertainty regarding their efficacy on top of more recent management strategies. From these studies, it has been extrapolated that beta-blockade may have an effect on prognosis in angina pectoris, but this has never been evaluated in randomized controlled trials.4 Actually, recent registry data demonstrate the opposite.33 In any case, in angina patients from both BEAUTIfUL and SHIfT, ivabradine was given on top of beta-blockers. Certainly, it did not worsen the prognosis but most likely improved it. Thus, it seems to be a logical to use ivabradine when elevated heart rate remains high. G28 Acknowledgements We thank Sarah Novack, PhD, who provided editorial assistance on behalf of Servier, France. Funding This work was supported by a grant from Fondazione Anna Maria Sechi per il Cuore (FASC), Italy. The funders had no role in the study design, data collection and analysis, decision to publish or the preparation of the manuscript. Conflict of interest: R.F. reported that he received honorarium from Servier for steering committee membership consulting and speaking, and support for travel to study meetings from Servier. In addition, he received personal fees from Boehringer-Ingelheim, Novartis, Merck Serono, and Irbtech. References 1. Borbely A, van der Velden J, Papp Z, Bronzwaer JG, Edes I, Stienen GJ, Paulus WJ. Cardiomyocyte stiffness in diastolic heart failure. Circulation 2005;111:774–781. 2. Tardif JC, Ford I, Tendera M, Bourassa MG, Fox K. Efficacy of ivabradine, a new selective I(f) inhibitor, compared with atenolol in patients with chronic stable angina. Eur Heart J 2005;26:2529–2536. 3. Tardif JC, Ponikowski P, Kahan T. Efficacy of the If current inhibitor ivabradine in patients with chronic stable angina receiving beta-blocker therapy: a 4 month, randomized, placebo-controlled trial. Eur Heart J 2009;30:540–548. 4. Fox K, Garcia MA, Ardissino D, Buszman P, Camici PG, Crea F, Daly C, De BG, Hjemdahl P, Lopez-Sendon J, Marco J, Morais J, Pepper J, Sechtem U, Simoons M, Thygesen K, Priori SG, Blanc JJ, Budaj A, Camm J, Dean V, Deckers J, Dickstein K, Lekakis J, McGregor K, Metra M, Morais J, Osterspey A, Tamargo J, Zamorano JL. Guidelines on the management of stable angina pectoris: executive summary: The Task Force on the Management of Stable Angina Pectoris of the European Society of Cardiology. Eur Heart J 2006;27:1341–1381. 5. Montalescot G, Sechtem U, Achenbach S, Andreotti F, Arden C, Budaj A, Bugiardini R, Crea F, Cuisset T, Di MC, Ferreira JR, Gersh BJ, Gitt AK, Hulot JS, Marx N, Opie LH, Pfisterer M, Prescott E, Ruschitzka F, Sabate M, Senior R, Taggart DP, van der Wall EE, Vrints CJ, Zamorano JL, Achenbach S, Baumgartner H, Bax JJ, Bueno H, Dean V, Deaton C, Erol C, Fagard R, Ferrari R, Hasdai D, Hoes AW, Kirchhof P, Knuuti J, Kolh P, Lancellotti P, Linhart A, Nihoyannopoulos P, Piepoli MF, Ponikowski P, Sirnes PA, Tamargo JL, Tendera M, Torbicki A, Wijns W, Windecker S, Knuuti J, Valgimigli M, Bueno H, Claeys MJ, Donner-Banzhoff N, Erol C, Frank H, Funck-Brentano C, Gaemperli O, Gonzalez-Juanatey JR, Hamilos M, Hasdai D, Husted S, James SK, Kervinen K, Kolh P, Kristensen SD, Lancellotti P, Maggioni AP, Piepoli MF, Pries AR, Romeo F, Ryden L, Simoons ML, Sirnes PA, Steg PG, Timmis A, Wijns W, Windecker S, Yildirir A, Zamorano JL. 2013 ESC guidelines on the management of stable coronary artery disease: The Task Force on the management of stable coronary artery disease of the European Society of Cardiology. Eur Heart J 2013;34: 2949–3003. 6. Fox K, Ford I, Steg PG, Tardif JC, Tendera M, Ferrari R. Ivabradine in stable coronary artery disease without clinical heart failure. N Engl J Med 2014;371:1091–1099. 7. Tendera M, Chassany O, Ferrari R, Ford I, Steg PG, Tardif JC, Fox K. Quality of life with ivabradine in patients with angina pectoris: The SIGNIFY Quality of Life Substudy. Circ Cardiovasc Qual Outcomes 2015; (submitted). 8. Fox K, Ford I, Steg PG, Tendera M, Ferrari R. Ivabradine for patients with stable coronary artery disease and left-ventricular systolic dysfunction (BEAUTIFUL): a randomised, double-blind, placebo-controlled trial. Lancet 2008;372:807–816. R. Ferrari 9. Swedberg K, Komajda M, Böhm M, Borer J, Ford I, Dubost-Brama A, Lerebours G, Tavazzi L. Ivabradine and outcomes in chronic heart failure (SHIFT): a randomised placebo-controlled trial. Lancet 2010; 376:875–885. 10. Fox K, Ford I, Steg PG, Tendera M, Robertson M, Ferrari R. Relationship between ivabradine treatment and cardiovascular outcomes in patients with stable coronary artery disease and left ventricular systolic dysfunction with limiting angina: a subgroup analysis of the randomized, controlled BEAUTIFUL trial. Eur Heart J 2009;30:2337–2345. 11. Califf RM, Mark DB, Harrell FE Jr, Hlatky MA, Lee KL, Rosati RA, Pryor DB. Importance of clinical measures of ischemia in the prognosis of patients with documented coronary artery disease. J Am Coll Cardiol 1988;11: 20–26. 12. Daly CA, De Stavola B, Sendon JL, Tavazzi L, Boersma E, Clemens F, Danchin N, Delahaye F, Gitt A, Julian D, Mulcahy D, Ruzyllo W, Thygesen K, Verheugt F, Fox KM. Predicting prognosis in stable angina--results from the Euro heart survey of stable angina: prospective observational study. BMJ 2006;332:262–267. 13. Gehi AK, Ali S, Na B, Schiller NB, Whooley MA. Inducible ischemia and the risk of recurrent cardiovascular events in outpatients with stable coronary heart disease: the heart and soul study. Arch Intern Med 2008;168:1423–1428. 14. Hultgren HN, Peduzzi P. Relation of severity of symptoms to prognosis in stable angina pectoris. Am J Cardiol 1984;54:988–993. 15. Mozaffarian D, Bryson CL, Spertus JA, McDonell MB, Fihn SD. Anginal symptoms consistently predict total mortality among outpatients with coronary artery disease. Am Heart J 2003;146:1015–1022. 16. Custodis F, Baumhakel M, Schlimmer N, List F, Gensch C, Bohm M, Laufs U. Heart rate reduction by ivabradine reduces oxidative stress, improves endothelial function, and prevents atherosclerosis in apolipoprotein E-deficient mice. Circulation 2008;117:2377–2387. 17. Triggle CR. Defying the economists: a decrease in heart rate improves not only cardiac but also endothelial function. Br J Pharmacol 2008; 154:727–728. 18. Borer JS, Swedberg K, Komajda M, Ford I, Tavazzi L, Boehm M, Depre C, Chen CY, Kim J, Dominjon F. Efficay profile of ivabradine in patients with heart failure plus angina pectoris. Abstract A791. J Am Coll Cardiol 2015;65:A791. 19. Ferrari R, Fox KM. The role of heart rate may differ according to pathophysiological setting: from SHIFT to SIGNIFY. Eur Heart J 2015;36: 2042–2046. 20. Logeart D, Gueffet JP, Rouzet F, Pousset F, Chavelas C, Solal AC, Jondeau G. Heart rate per se impacts cardiac function in patients with systolic heart failure and pacing: a pilot study. Eur J Heart Fail 2009;11:53–57. 21. Thackray SD, Ghosh JM, Wright GA, Witte KK, Nikitin NP, Kaye GC, Clark AL, Tweddel A, Cleland JG. The effect of altering heart rate on ventricular function in patients with heart failure treated with betablockers. Am Heart J 2006;152:713–713. 22. Heusch G. Heart rate and heart failure. Not a simple relationship. Circ J 2011;75:229–236. 23. Panza JA, Diodati JG, Callahan TS, Epstein SE, Quyyumi AA. Role of increases in heart rate in determining the occurrence and frequency of myocardial ischemia during daily life in patients with stable coronary artery disease. J Am Coll Cardiol 1992;20:1092–1098. 24. Fox K, Borer JS, Camm AJ, Danchin N, Ferrari R, Lopez Sendon JL, Steg PG, Tardif JC, Tavazzi L, Tendera M. Resting heart rate in cardiovascular disease. J Am Coll Cardiol 2007;50:823–830. 25. Fox KM, Ferrari R. Heart rate: a forgotten link in coronary artery disease? Nat Rev Cardiol 2011;8:369–379. 26. Nissen SE, Tuzcu EM, Libby P, Thompson PD, Ghali M, Garza D, Berman L, Shi H, Buebendorf E, Topol EJ. Effect of antihypertensive agents on cardiovascular events in patients with coronary disease and normal blood pressure: the CAMELOT study: a randomized controlled trial. JAMA 2004;292:2217–2225. 27. Poole Wilson PA, Lubsen J, Kirwan BA, Van Dalen FJ, Wagener G, Danchin N, Just H, Fox KA, Pocock SJ, Clayton TC, Motro M, Parker JD, Bourassa MG, Dart AM, Hildebrandt P, Hjalmarson A, Kragten JA, Molhoek GP, Otterstad JE, Seabra Gomes R, Soler Soler J, Weber S. Effect of long-acting nifedipine on mortality and cardiovascular morbidity in patients with stable angina requiring treatment (ACTION trial): randomised controlled trial. Lancet 2004;364:849–857. Ivabradine in the management of CAD with or without LVD or HF 28. Dargie HJ. Effect of nicorandil on coronary events in patients with stable angina: the Impact Of Nicorandil in Angina (IONA) randomised trial. Lancet 2002;359:1269–1275. 29. Dargie HJ, Lechat P, Erdmann E, Follath F, Hoglund C, Lopez Sendon JL, Mareyev V, Remme WJ, Sadowski Z, Seabra Gomes RJ, Zannas F, Wehrlen Grandjean M, Funck Brentano C, Hansen S, Hohnloser S, Vanoli E, Jaillon P, De Baker G, Dahlstr’M U, Hill C, Leizorovicz A, Bugnard F, Rolland C, Wiemann H, Verkenne P, Arab T, Cussac N, Dussous V, Haise S, Funck Brentano C. The Cardiac Insufficiency Bisoprolol Study II (CIBIS-II): a randomised trial. Lancet 1999;353:9–13. 30. Freemantle N, Cleland J, Young P, Mason J, Harrison J. beta Blockade after myocardial infarction: systematic review and meta regression analysis. BMJ 1999;318:1730–1737. G29 31. Hjalmarson A, Goldstein S, Fagerberg B, Wedel H, Waagstrein F, Kjekshus J, Wikstrand J, Westergren G, Thimell M. Effect of metoprolol CR/XL in chronic heart failure: Metoprolol CR/XL Randomised Intervention Trial in Congestive Heart Failure (MERIT-HF). Lancet 1999;353: 2001–2007. 32. Packer M, Coats AJ, Fowler MB, Katus HA, Krum H, Mohacsi P, Rouleau JL, Tendera M, Castaigne A, Roecker EB, Schultz MK, De Mets DL. Effect of carvedilol on survival in severe chronic heart failure. N Engl J Med 2001; 344:1651–1658. 33. Bangalore S, Steg G, Deedwania P, Crowley K, Eagle KA, Goto S, Ohman EM, Cannon CP, Smith SC, Zeymer U, Hoffman EB, Messerli FH, Bhatt DL. Beta-blocker use and clinical outcomes in stable outpatients with and without coronary artery disease. JAMA 2012;308:1340–1349.