Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Remote ischemic conditioning wikipedia , lookup
Coronary artery disease wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Cardiac surgery wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Atrial septal defect wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
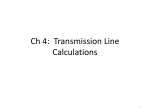
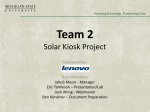
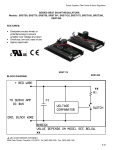
The British Journal of Radiology, 82 (2009), 386–391 Quantification of left-to-right shunting in adult congenital heart disease: phase-contrast cine MRI compared with invasive oximetry 1 K DEBL, MD, 2B DJAVIDANI, MD, 1S BUCHNER, MD, 1N HEINICKE, 2 S FEUERBACH, MD, 1G RIEGGER, MD and 1A LUCHNER, MD MD, 2 F POSCHENRIEDER, MD, 1 Klinik und Poliklinik für Innere Medizin II and 2Institut für Röntgendiagnostik, Universitätsklinikum Regensburg, Germany ABSTRACT. Atrial septum defects (ASDs), ventricular septum defects (VSDs) and patent ductus arteriosus (PDA) are the most common adult congenital heart defects. The degree of left-to-right shunting as assessed by the ratio of flow in the pulmonary (Qp) and systemic circulation (Qs) is crucial in the management of these conditions. This study compared phase-contrast cine magnetic resonance imaging (PC-MRI), a non-invasive imaging technique, with invasive oximetry for the measurement of shunt volumes during cardiac catheterisation in adults with left-to-right shunting. Both invasive oximetry and shunt quantification by PC-MRI (1.5 T scanner; Sonata, Siemens Medical Solutions) were performed on 21 patients with left-to-right shunting (14 ASD, 5 VSD, 2 PDA) and data on Qp/Qs ratios and left-to-right shunt fraction compared. Mean Qp/Qs ratios assessed by PC-MRI and oximetry were 2.10¡0.76 and 1.96¡0.77, respectively (p 5 0.37). Mean shunt fraction was 46.3¡19.6% when calculated by PC-MRI and 42.3¡20.1% when obtained by oximetry (p 5 0.12). There was a strong correlation of Qp/Qs ratios and shunt fraction between both methods (r 5 0.61, p , 0.01 and r 5 0.84, p , 0.0001, respectively). The two methods had a good agreement according to Bland and Altman plots with a small but non-significant overestimation of Qp/Qs-ratios and shunt fraction by PC-MRI. On receiver operating characteristic analysis, the sensitivity and specificity of PC-MRI to detect an oximetry-derived Qp/Qs ratio of >1.5:1 were 93% and 100% at a PC-MRI threshold of a Qp/Qs ratio >1.75:1 (area under curve (AUC) 5 0.99). Quantification of left-to-right shunting can be performed reliably and accurately by PC-MRI and the data obtained by this method correlate closely to those from invasive oximetry. Atrial septum defects (ASDs), ventricular septum defects (VSDs) and patent ductus arteriosus (PDA) are the most common congenital heart defects in both children and adults. Quantification of shunt volumes and of the ratio of flow in the pulmonary (Qp) and systemic circulation (Qs) and assessment of cardiac dilatation as a consequence of volume overload are crucial in the management of patients with left-to-right shunting [1–3]. Transthoracic and transoesophageal echocardiography usually allow exact localisation and sizing of the defect. However, determination of shunt volumes by Doppler echocardiography has limitations [4]. Invasive oximetry using Fick’s principle is the standard of reference for the quantification of left-toright shunting based on measurements of blood oxygenation [5–7]. Interventional closure or corrective surgery is usually indicated in patients with a Qp/Qs ratio >1.5. MRI is a non-invasive method that allows an exact visualisation of cardiac anatomy and an accurate noninvasive sizing of congenital septal defects [8–10]. Additionally, phase-contrast cine MRI (PC-MRI) allows the comparative quantification of cardiac blood flow in the pulmonary artery with that in the ascending aorta. Received 30 August 2007 Revised 24 February 2008 Accepted 6 May 2008 DOI: 10.1259/bjr/18500608 ’ 2009 The British Institute of Radiology Very good agreement of shunt quantifications by PCMRI and invasive oximetry has been shown in children with congenital heart disease [11–16]. Data on shunt quantification by PC-MRI in adults are, however, limited and predictive values in comparison with oximetry are lacking. The aim of our study was therefore to compare shunt volumes assessed by PC-MRI and invasive oximetry in adults with left-to-right shunting. Methods Patients The study included 21 consecutive adult patients with suspected or known left-to-right shunt admitted to our institution for shunt quantification. Invasive oximetry and shunt quantification by PC-MRI were performed in all patients within 1 week. All patients gave written informed consent. PC-MRI and catheterisation studies were well tolerated in all patients. Magnetic resonance imaging studies Address correspondence to: K Debl, Klinik und Poliklinik für Innere Medizin II, Universitätsklinikum, F.J.-Strauss-Allee 11, 93042 Regensburg, Germany. E-mail: [email protected] K Debl and B Djavidani contributed equally as first author. 386 Magnetic resonance imaging studies were performed on a 1.5 T scanner (Sonata, Siemens Medical Solutions). For the assessment of cardiac function and localisation of The British Journal of Radiology, May 2009 Quantification of shunting in adult congenital heart disease by MRI (a) (b) (c) Figure 1. (a) 4-chamber view of a patient with an atrial septum defect II (SSFP sequences); (b) phase-contrast image perpendicular to the ascending aorta; (c) phase-contrast image perpendicular to the main pulmonary artery. the left-to-right shunt, cine images were acquired in multiple short axis and long axis views by fast imaging with steady-state precession (SSFP, slice thickness 8 mm, echo time 1.53 ms, pixel bandwidth 1085 Hz, repetition time 3.14 ms, matrix 256*202). In addition, SSFP sequences were performed to generate scout images of the ascending aorta and pulmonary trunk in three planes. Flow volumes in the ascending aorta and pulmonary trunk were determined in the isocentre of the magnet using through plane phase-contrast MRI (PCMRI) in a retrospective gating technique during normal respiration (flash 2D; slice thickness 5 mm, echo time 3.2 ms, pixel bandwidth 391 Hz, repetition time 41 ms, matrix 256*192), as described previously [17]. Using the SSFP scout images, PC-MRI was performed orthogonally to the ascending aorta and the main pulmonary artery. Slice position in the ascending aorta was approximately 2.0–3.0 cm above the aortic valve distal to the coronary arteries at the level of the right pulmonary artery. Slice position in the pulmonary trunk was approximately 1.5– 2.0 cm above the pulmonary valve but proximal to the bifurcation. Using this approach, the influence of the angle deviation is usually below 15 ˚ and therefore negligible. To optimise the accuracy of PC-MRI, the velocity encoding was set as low as possible while avoiding aliasing artefacts. Usually, the velocity encoding was 150 cm s21 for the measurement of the aortic and pulmonary flow. To achieve flow results as physiological as possible, PC-MRI was performed during normal respiration. Data analyses were performed using ARGUS Flow software (Sonata, Siemens Medical Solutions). For the calculation of pulmonary (Qp) and systemic (Qs) flow volumes, the cross-sectional areas of the pulmonary trunk and ascending aorta were drawn manually for each time frame on the magnitude images and transferred to the corresponding phase image (Figure 1). Shunt volumes for left-to-right shunts in ASD and VSD were calculated by the following formula: Left-to-right shunt ð%Þ~ðQp{QsÞ=Qp ð1Þ and in the case of PDA as: (Qs{Qp)=Qs The British Journal of Radiology, May 2009 ð2Þ Oximetry Calculation of Qp and Qs values was performed as described by Grossman [18]. Blood samples in the upper and lower vena cavae, right atrium and ventricle, pulmonary arteries and a systemic artery were taken to determine the oxygen saturation. The shunt volume was calculated by the difference of mixed venous and pulmonary oxygen saturation. The invasive calculation of the blood flow for the systemic and pulmonary circulation was determined by Fick’s principle: Qp l min{1 ~Oxygen uptake ml min{1 =PVcontent ml l{1 PAcontent ml l{1 ð3Þ Qs l min{1 ~Oxygen uptake ml min{1 =SAcontent ml l{1 MVcontent ml l{1 ð4Þ where PVcontent is the systemic arterial oxygen content, PAcontent is the oxygen content in the pulmonary artery, SAcontent is the systemic arterial oxygen content, MVcontent is the mixed venous oxygen content calculated as (3 6 superior vena cava oxygen saturation + inferior vena cava oxygen saturation)/4. Again, shunt volumes for left-to-right shunts were calculated by the following formula: Left-to-right shunt ð%Þ~ðQp{QsÞ=Qp ð5Þ Statistical analysis The agreement between the methods of shunt quantification was assessed by univariate regression analysis and by the Bland–Altman method. Differences in mean values between two groups were analyzed by Student’s t-test. The x2 test was performed to compare frequencies between groups. Receiver operating characteristic (ROC) analysis was carried out to determine the predictive ability of PC-MRI to detect left-to-right shunting as defined by oximetry. A level of significance of below 0.05 387 K Debl, B Djavidani, S Buchner et al was defined as statistically significant. SPSS version 12.0.1 was used for statistical analysis. 100%, respectively, at a PC-MRI threshold of a Qp/Qs ratio >1.75:1 (AUC 5 0.99) (Table 2). Results Discussion Patient characteristics are depicted in Table 1. Of the 21 patients, 14 had ASD (9 ASD II, 3 ASD I, 2 sinus venosus defect), 5 VSD and 2 PDA. No significant differences in age, gender, rhythm and mean pulmonary artery pressure were observed in patients with Qp/Qs ratios , 1.5 as compared to patients with Qp/Qs ratios >1.5. Our study demonstrates that the quantification of leftto-right shunting in adults by PC-MRI is feasible and reliable. There is a good correlation to the data derived by invasive oximetry, with a small but non-significant overestimation of Qp/Qs ratios and shunt fractions by PC-MRI. Furthermore, PC-MRI obtained excellent predictive values for the detection of significant left-to right shunting requiring shunt closure (Table 2). Comparison of shunt quantification by oximetry and MRI Quantification of left-to-right shunting by PC-MRI compared to oximetry Mean Qp/Qs ratios ¡ 2 SD assessed by PC-MRI and cardiac catheterisation were 2.10¡0.76 and 1.96¡0.77, respectively (p 5 0.37). Mean shunt fraction was 46.3¡19.6% when assessed by PC-MRI and 42.3¡20.1% at cardiac catheterisation (p 5 0.12). Mean differences of Qp/Qs ratios and shunt fraction between the two assessment methods were 0.14% and 4.0%, respectively. Both Qp/Qs ratios and shunt fraction were strongly correlated between the two methods (r 5 0.61, p , 0.01 and r 5 0.84, p , 0.0001, respectively). The Bland–Altman plots also showed good agreement between the two methods with a small but nonsignificant overestimation of Qp/Qs ratios and shunt fraction by PC-MRI. Figures 2 and 4 show that in two patients the Qp/Qs ratios obtained by PC-MRI and cardiac catheterisation fell at opposite sides of the cut-off value for clinical decision making of 1.5. PC-MRI would have suggested defect closure in these two cases, whereas oximetry would have led to a conservative strategy (Figures 2–5). The current study is among the first to compare PCMRI and oximetry by cardiac catheterisation in freebreathing adults who have congenital heart disease. It confirms previous studies that have already shown the feasibility of this technique and a good correlation with invasive oximetry in children. In the management of patients with left-to-right shunting, quantification of the ratio of flow in the pulmonary (Qp) and systemic circulation (Qs) and assessment of cardiac dilatation as a consequence of volume overload are crucial [1–3]. Invasive oximetry is the gold standard for the quantification of left-to right shunting but has several limitations. Oxygenation of venous and arterial blood is especially influenced by several factors such as sedation, agitation and ventilation disorders. Furthermore, the true mixed venous saturation is not measured directly but is calculated by sampling from the superior and inferior vena cavae. Additionally, there is a large intra-individual variability of Qp/Qs ratios assessed by oximetry [6]. Despite these limitations, oximetry remains the standard criterion against which new non-invasive methods must be judged. A potential limitation of PC-MRI-based calculation of the shunt volume calculation may result from the assessment of systemic flow in the ascending aorta distal to the coronary ostia, which would miss coronary blood flow. This technical limitation may result in a small underestimation of Qs values and consequently lead to a slight overestimation of Qp/Qs ratios and left-to-right shunt fraction, respectively. In consequence, underestimation of Qs is probably responsible for a small overestimation of shunt volumes by PC-MRI compared to oximetry. In this respect, our study is in agreement with a recent study [11] that also suggests that quantification of left-to-right shunting by PC-MRI may overestimate shunt volumes as compared to invasive oximetry. Accordingly, ROC analysis determined that detection of Qp/Qs ratios of >1.5:1 by oximetry was best achieved at a PC-MRI threshold of >1.75:1. In our study, PC-MRI derived Qp/Qs ratios pointed to shunt closure in two patients, whereas oximetry-based Qp/Qs ratios would have favoured a conservative strategy. Interestingly, the Qp/Qs ratios assessed by oximetry were only slightly below the cut-off value of 1.5 in these two patients. Qp/Qs ratio is, however, only one criterion in clinical decision making in left-to-right Patients Predictive values of PC-MRI for severity of left-toright shunting As assessed by ROC analysis, the sensitivity and specificity of PC-MRI in detecting Qp/Qs ratios of >1.5:1 (as determined by invasive oximetry) were 93% and Table 1. Patient characteristics Age Gender (% male) SR (%) Mean PAP (mm Hg) Cardiac shunts ASD (n) VSD (n) PDA (n) Qp/Qs ,1.5 (n56) Qp/Qs >1.5 (n515) 47.0¡14.0 66 50 19.0¡7.2 50.9¡16.9 53 80 25.4¡12.7 2 4 0 11 1 2 Qp/Qs, pulmonary-to-systemic flow ratio assessed by oximetry; SR, sinus rhythm; PAP, pulmonary artery pressure, derived at right heart catheterisation; ASD, atrial septum defect; VSD, ventricular septum defect; PDA, patent ductus arteriosus. 388 The British Journal of Radiology, May 2009 Quantification of shunting in adult congenital heart disease by MRI Figure 2. Pulmonary-to-systemic flow ratios (Qp/Qs) determined by phase-contrast cine MRI (PC-MRI) and oximetry in 21 patients with left-to-right shunting. Only two patients are in the right lower quadrant in which a PC-MRI derived Qp/Qs ratio of >1.5 would have suggested shunt closure, whereas data from oximetry would not have. shunting in adults. Although there are limitations in estimating Qp/Qs ratios with any method, high levels of shunting are usually associated with adverse long-term outcomes. Especially in ASD, further signs such as right heart dilatation and an ASD minimum diameter .10 mm must also be considered in the management of these patients [1]. In VSD, left ventricular volume overload or progressive aortic valve disease are usually additional indications for shunt closure [2]. Finally, PDA closure is clearly indicated for symptomatic adults with significant left-to-right shunting and for asymptomatic patients with significant left-to-right shunting and evidence of left heart enlargement [3]. Clinical relevance of MRI in left-to-right shunt quantification With respect to the clinical work-up of patients with left-to-right shunting, transthoracic and transoesopha- Figure 3. The Bland and Altman plot depicts the mean of the pulmonary-to-systemic flow ratios (Qp/ Qs) obtained by phase-contrast cine MRI (PC-MRI) and oximetry and the difference between these Qp/Qs ratios for each of 21 patients with left-to-right shunting. The mean difference (solid line) and ¡ 2 SD from this difference (broken lines) across all patients are shown. The British Journal of Radiology, May 2009 389 K Debl, B Djavidani, S Buchner et al Figure 4. Left-to-right shunt fractions determined by phase-contrast cine MRI (PC-MRI) and oximetry in 21 patients with left-to-right shunting. Only two patients are in the right lower quadrant where a PCMRI-derived shunt fraction suggests shunt closure whereas oximetry does not. geal echocardiography are often adequate to determine the defect size. However, transoesophageal echocardiography is semi-invasive and might have limitations in visualisation of adjacent structures and anomalous venous return. Determination of shunt volumes by Doppler echocardiography also has limitations [4]. Invasive oximetry using Fick’s principle is the standard of reference for the quantification of left-to-right shunting based on measurements of blood oxygenation, but also has several limitations as discussed above. PC-MRI could overcome these problems of defect sizing and quantification of shunt volumes. Interestingly, ASD sizing by MRI correlates well with assessments made by transoesophageal echocardiography and provides additional information on defect shapes, rim distances and pulmonary and venous anomalies that are often associated with left-to-right shunting in congenital defects [8–10]. Furthermore, PC-MRI allows the reliable quantification of left-to-right shunting. MRI can therefore provide anatomical and functional information in a single examination. Figure 5. The Bland and Altman plot depicts the mean left-to-right shunt fraction derived by phasecontrast cine MRI (PC-MRI) and oximetry and the difference of leftto-right shunt fractions by PC-MRI and oximetry for each of 21 patients with left-to-right shunting. The mean difference (solid line) and ¡ 2 SD from this difference (broken lines) across all patients are shown. 390 The British Journal of Radiology, May 2009 Quantification of shunting in adult congenital heart disease by MRI Table 2. Predictive values CATH-Qp/Qs >1.5:1 CATH-shunt >33.3% Cases /Total (n) PC-MRI cut-off ROC area (95% CI) Sensitivity (%)/specificity (%) 15/21 15/21 1.75:1 43% 0.99 (0.97–1.02) 0.99 (0.97–1.02) 93/100 93/100 CI, confidence interval; ROC, receiver operating characteristic; PC-MRI, phase-contrast cine MRI. In summary, quantification of left-to-right shunting can be performed reliably and accurately by PC-MRI and provides results that correlate closely with those obtained by invasive oximetry, although there is a small overestimation of the degree of shunting. In the clinical management of patients with left-to-right shunting, MRI can provide anatomical and functional information in a single examination and is a useful technique for the assessment of adult congenital heart disease. References 1. Webb G, Gatzoulis M. Atrial septal defects in the adult: recent progress and overview. Circulation 2006;114:1645–53. 2. Minette MS, Sahn DJ. Ventricular septal defects. Circulation 2006;114:2190–7. 3. Schneider DJ, Moore JW. Patent ductus arteriosus. Circulation 2006;114:1873–82. 4. Boehrer JD, Lange RA, Willard JE, Grayburn PA, Hillis LD. Advantages and limitations of methods to detect, localize, and quantitate intracardiac left-to-right shunting. Am Heart J 1992;124:448–55. 5. Daniel WC, Lange RA, Willard JE, Landau C, Hillis LD. Oximetric versus indicator dilution techniques for quantitating intracardiac left-to-right shunting in adults. Am J Cardiol 1995;75:199–200. 6. Cigarroa RG, Lange RA, Hillis LD. Oximetric quantitation of intracardiac left-to-right shunting: limitations of the Qp/ Qs ratio. Am J Cardiol 1989;64:246–7. 7. Antman EM, Marsh JD, Green LH, Grossman W. Blood oxygen measurements in the assessment of intracardiac left to right shunts: a critical appraisal of methodology. Am J Cardiol 1980;46:265–71. 8. Sechtem U, Pflugfelder P, Cassidy MC, Holt W, Wolfe C, Higgins CB. Ventricular septal defect: visualization of shunt flow and determination of shunt size by cine MR imaging. Am J Roentgenol 1987;149:689–92. 9. Piaw CS, Kiam OT, Rapaee A, Khoon LC, Bang LH, Ling CW et al. Use of non-invasive phase contrast magnetic resonance imaging for estimation of atrial septal defect size The British Journal of Radiology, May 2009 10. 11. 12. 13. 14. 15. 16. 17. 18. and morphology: a comparison with transesophageal echo. Cardiovasc Intervent Radiol 2006;29:230–4. Beerbaum P, Korperich H, Esdorn H, Blanz U, Barth P, Hartmann J et al. Atrial septal defects in pediatric patients: noninvasive sizing with cardiovascular MR imaging. Radiology 2003;228:361–9. Esmaeili A, Hohn R, Koch A, Vogl TJ, Hofstetter R, Abolmaali N. Assessment of shunt volumes in children with ventricular septal defects: comparative quantification of MR flow measurements and invasive oximetry. Clin Res Cardiol 2006;95:523–30. Beerbaum P, Korperich H, Barth P, Esdorn H, Gieseke J, Meyer H. Noninvasive quantification of left–to-right shunt in pediatric patients: phase–contrast cine magnetic resonance imaging compared with invasive oximetry. Circulation 2001;103:2476–82. Beerbaum P, Korperich H, Gieseke J, Barth P, Peuster M, Meyer H. Rapid left-to-right shunt quantification in children by phase–contrast magnetic resonance imaging combined with sensitivity encoding (SENSE). Circulation 2003;108:1355–61. Hundley WG, Li HF, Lange RA, Pfeifer DP, Meshack BM, Willard JE et al. Assessment of left-to-right intracardiac shunting by velocity-encoded, phase–difference magnetic resonance imaging. A comparison with oximetric and indicator dilution techniques. Circulation 1995;91:2955–60. Kalden P, Kreitner KF, Voigtlander T, Roberts H, Roberts T, Krummenauer F et al. Flow quantification of intracardiac shunt volumes using MR phase contrast technique in the breath holding phase. Rofo 1998;169:378–82. Petersen SE, Voigtlander T, Kreitner KF, Kalden P, Wittlinger T, Scharhag J et al. Quantification of shunt volumes in congenital heart diseases using a breath-hold MR phase contrast technique — comparison with oximetry. Int J Cardiovasc Imaging 2002;18:53–60. Lotz J, Meier C, Leppert A, Galanski M. Cardiovascular flow measurement with phase–contrast MR imaging: basic facts and implementation. Radiographics 2002;22:651–71. Grossman W. Shunt detection and measurement. In: Grossman W, Baim DS, eds. Cardiac catheterization, angiography and intervention. 4th ed. Philadelphia, PA: Lea & Febiger; 1991:166–181. 391