Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Myocardial infarction wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Coronary artery disease wikipedia , lookup
Heart arrhythmia wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
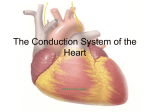
Objective 8 Coronary Circulation The function of coronary circulation is to supply the myocardium with blood. Arterial Supply: The right coronary artery (RCA) and the left coronary artery (LCA) originate from the aorta at the sinuses of Valsalva Branching of the RCA and LCA Aorta Right Coronary Artery Marginal Artery Posterior Interventicular Artery serves the right lateral wall of the heart serves the posterior wall of both ventricles Left Coronary Artery Anterior Interventricular Artery serves the anterior walls of both ventricles and the interventricular septum Circumflex Artery serves the lateral left atrium and and posterior wall of the left ventricle Venous Drainage: Deoxygenated blood is collected by cardiac vein and emptied into the right atrium Right Atrium Anterior Cardiac Veins drains the anterior surface Great Cardiac Vein drains the anterior surface Coronary Sinus Middle Cardiac Vein drains the posterior surface Small Cardiac Vein drains the inferior right margin C. Terms: anastomosis: union or joining of two blood vessels (nerves or lymphatics) collateral alternative route of circulation to an area provided by an circulation: anastomosis ischemia: infarction: insufficient blood supply to an organ or a tissue, usually due to a blocked artery localized necrosis resulting from an obstruction of the blood supply Schematic drawing of the coronary artery circulation without (A) and with interarterial anastomoses (B) between the right coronary artery and the occluded left anterior descending artery (occluded downstream of the third diagonal branch). Traupe T et al. Circulation 2010;122:1210-1220 Copyright © American Heart Association Changes in Infarcted Tissue: 1. Bruised, cyanotic tissue 2. Edema, inflammation and leukocytosis with 24 hours 3. Cardiac enzymes (creatine kinase, lactate dehydrogenase) released within 2-3 days 4. Tissue degradation and replacement by scar tissue Scar tissue Angina Pectoris: thoracic pain resulting from ischemia Objective 9 Cardiac Muscle A. Structure Myocytes (cells) - small, branching, lightly striated fibers One -two centrally located nuclei Poorly developed sarcoplasmic reticulum; no triads Large and abundant mitochondria Myogobin present Intercalated discs, made of gap junctions/desmosomes join cells allow small molecules and ions to pass between cells electrically couple the myocytes (functional syncytium, note: no gap junctions between atrial and ventricular cells) desmosomes prevent cell separation during contraction High capillary density B. Metabolism • utilize aerobic respiration for ATP generation • can use fatty acids for ATP production In summary, what structural adaptations maximize the cardiac myocytes capacity for aerobic respiration? 1. 2. 3. 4. Many large mitochondria Myoglobin High capillary density Can use fatty acids for fuel C. Contraction Properties slower speed of contraction than skeletal muscle are autorhythmic (myogenic) and can contract in the absence of a stimulus receives dual innervation from the autonomic nervous system (SNS HR and force of contraction; PNS HR and force of contraction ) What is the neurotransmitter and receptor type for SNS? Norepinephrine binds to adrenergic receptors What is the neurotransmitter and receptor type for PNS ? Acetylcholine binds to cholinergic receptors cells respond to stretching with a more vigorous contraction, remember the length-tension curve??? cells have a long absolute refractory period What is the importance of this? Objective 10 Autorhythmic and Contractile Cells There are two populations of myocytes in the heart: autorhythmic cells and contractile cells Location Function Autorhythmic Cells Contractile Cells Intrinsic conduction system: SA node, AV node, AV bundle, bundle branches, purkinje fibers All other myocytes Initiate the action potentials that stimulate contractile cells; set heart rate Contract and relax during systole and diastole; they serve as pumping cells A Typical Action Potential for Neurons, Skeletal Muscle Cells Action potential of autorhythmic cells…. 1. Pacemaker potential: gradual decrease in K+ efflux and increased Na+ influx through slow Na+ channels causes gradual depolarization 3 2 2. Threshold (-40mV); Ca2+ channels open and Ca2+ enters the cell from the ECF; this causes depolarization 1 3. Repolarization occurs when Ca2+ channels close and voltage regulated K+ open; K+ leaves the cell Action Potential For Contractile Cardiac Cells (99% of cardiac myocytes) 0. Depolarization Voltage regulated fast Na+ channels open and Na+ enters from the ECF causing depolarization 1. and 2. Plateau: Ca2+ enters the sarcoplasm from the SR and from the ECF through slow Ca2+ ; channels; at the same time there is a decrease in K+ permeability; this causes a prolonged depolarization 3. Repolarization Occurs as the Ca2+ channels close the voltage regulated K+ channels open; K+ leaves the cell 4. Back to resting membrane potential From AP to Contraction AP travels down T-Tubules of the myocyte Calcium enters cell Calcium binds to troponin Troponin tropomyosin complex exposes myosin binding sites on actin Thin filament slide toward toward center of the sarcomere thick filaments Contraction Refractory Period of Contractile Cardiac Myocytes: The long refractory period of contractile cardiac myocytes prevents sustained contraction (tetany) in cardiac muscle and ensures that filling time (diastole) occurs. mV time absolute refractory period atrial cells: 0.15 sec ventricular cells 0.30 sec Objective 11 The Intrinsic Conduction System SA node ↓ AV node ↓ AV bundle ↓ Bundle branches ↓ Purkinje fibers Element Sinoatrial (SA) node Location right atrial wall, just below the SVC entrance Comments inherent depolarization rate is 100/minute normally slowed by extrinsic factors is the normal pacemaker for the heart SA node ↓ AV node ↓ AV bundle ↓ Bundle branches ↓ Purkinje fibers Element Location Comments Interatrial Pathways within the atrial myocardium Bachman’s Bundle delivers the impulse to left atrium; internodal pathways deliver the impulse through the right atrium and to the AV node and Internodal Pathways SA node ↓ AV node ↓ AV bundle ↓ Bundle branches ↓ Purkinje fibers Element Atrioventricular (AV) node Location interatrial septum above tricuspid valve Comments impulse delayed .01 sec inherent rate 40-60/minute SA node ↓ AV node ↓ AV bundle ↓ Bundle branches ↓ Purkinje fibers Element Atrioventricular Bundle (of His) Location Superior interventricular septum Comments Only normal conduction pathway from atria into ventricles SA node ↓ AV node ↓ AV bundle ↓ Bundle branches ↓ Purkinje fibers Element Right and left bundle branches Location Interventricular septum Comments Carries apex of the heart SA node ↓ AV node ↓ AV bundle ↓ Bundle branches ↓ Purkinje fibers Element Purkinje fibers Location Ventricular myocardium Comments Stimulate papillary muscles and ventricular myocardial cells Inherent rate is 15-30 depolarizations per minute A picture is worth a thousand words…. http://www.youtube.com/watch?v=bxKBQqe_Bo0