Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Jatene procedure wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Ventricular fibrillation wikipedia , lookup
Atrial fibrillation wikipedia , lookup
Heart arrhythmia wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
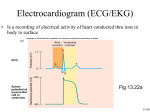
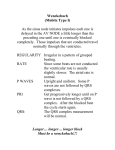
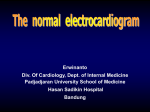
Scoring Center: Scoring Cardiac Dysrhythmias - Part 2 By Jon Atkinson, BS, RPSGT Editor’s Note: This is the second of a two-part series on scoring cardiac dysrhythmias. The first part was published in A2Zzz volume 16, number 4. For more information, including detailed features and figures of brief graphic samples, refer to chapter 36, “Cardiac Arrhythmias,” in the Fundamentals of Sleep Technology textbook (Lippincot Williams & Wilkins, 2007). The key to identifying cardiac dysrhythmias is first to understand what is normal. This begins with knowledge of the conducting system of the heart and the relationship of the electrophysiologic phenomena to the electrographic representation of the cardiac cycle. Figure 1 is an exterior view of the heart, and Figure 2 is a cross-section showing a representation of the conducting system of the heart. The normal cardiac cycle begins with a discharge of the sinoatrial (SA) node. This causes a wave of excitation across the atrium (atrial depolarization) that is represented by the P wave of the normal EKG complex. See Figure 3. Superior Vena Cava Aorta Pulmonary Artery Right Atrium Left Atrium Pulmonary Veins Right Ventricle Left Ventricle Figure 1. Exterior view of the heart Interatrial Septum Right Atrium Left Atrium AV Bundle (His) SA Node Intermodal Pathways AV Node Left Ventricle Left Bundle Branch Right Ventricle Right Bundle Branch Interventricular Septum Purkinje Fibers Figure 2. The conducting system of the heart 30 A2Zzz 2008 • volume 17 • number 1 Atrial depolarization Ventricular repolarization R T P Q S PR interval QRS interval Figure 3. The cardiac cycle There is a brief delay in conduction at the atrioventricular (AV) node, located near the junction of the atria and the ventricles in the interatrial septum separating the right and left atria. The P wave and this pause comprise the P-R interval. The normal P-R interval is 0.12 to 0.20 seconds duration. Once the AV node is stimulated, it sends a wave of depolarization down the atrioventricular bundle (bundle of His) and then to the right and left bundle branches of the conducting system. The left bundle branch bifurcates into an anterior and a posterior limb. These and the right bundle branch terminate into the Purkinje fibers, which terminate on all the cells of the myocardium, essentially allowing the entire muscle mass of the ventricles to depolarize and contract simultaneously. This is electrographically represented as the QRS complex. A key concept in cellular physiology is that in cyclical phenomena, if cells depolarize, then they must then repolarize to prepare for the next depolarization cycle. The T wave of the EKG complex represents repolarization of the ventricle. The waveform associated with repolarization of the atria is not seen because of its low amplitude and its simultaneous occurrence during the much higher amplitude QRS complex. In the adult human heart, this cyclical depolarization and repolarization occurs at a rate of 60 to 100 times per minute. This is related to another concept: “the rules of morphology.” When recorded from the same two points, an electrical phenomenon that starts at the same location and takes the same pathway will always look the same electrographically. This is the “rule of same morphology.” Conversely, if the phenomenon starts in a different location or travels a different pathway, the waveform will look different; this is the “rule of differing morphology.” The Normal Sinus Rhythm (NSR) In NSR for the adult, the P wave will always look the same, and the QRS complexes will always be identical. If depolarization always starts in the same place and takes the same pathway, the repolarization waveform (T wave) also will look the same. The ratio of P waves to QRS complexes will always be 1 to 1; i.e., there is a P wave for every QRS complex and a QRS complex for every P wave. The P-R interval will range from 0.12 to 0.20 seconds, and the QRS interval will be between 0.04 and 0.12 seconds in duration. The rhythm will be regular; i.e., the P to P interval and the R to R interval will be constant. The rate will be 60 to 100 per minute. Table 1 describes the parameters or waveforms and their characteristics or values for NSR. Parameter/ waveform Value/characteristic P wave: Present, each appears the same QRS complex: Present, each appears the same PR interval: 0.12-0.20 seconds QRS interval: 0.04-0.12 sounds P:QRS ratio: 1:1 Rate: 60-100 bpm Rhythm: Regular Table 1. Characteristics of NSR Arrhythmia Analysis Steps This section presents routine steps you should follow for a comprehensive and accurate analysis of cardiac rhythm disturbances. Whenever possible you should add a second, different EKG dipole to the montage. This may reveal differences in P wave or QRS complex configuration. It can be difficult to identify these differences with only a singlechannel recording. Use either a 10-second window or a sixsecond window when examining the EKG for detail. This will enable you to analyze the intervals and look for subtle changes in morphology. Following these routine steps will help you identify arrhythmias with greater accuracy: Step 1: Examine the P wave. Examine the tracing to detect the absence or presence of P waves. If there is no distinct P wave, then you know that the arrhythmia is not of atrial origin, except in these three cases: Atrial fibrillation: The P waves are replaced by fibrillatory waves. Atrial flutter: The P waves are replaced by Sawtoothappearing flutter waves Sinus pauses: Both P wave and corresponding QRS complexes are absent. Next, examine the P wave configuration. Do the P waves all look the same? In other words, do they have the same morphology? Remember the rules of differing morphology and same morphology that are described above. Step 2: Examine the QRS complex. Check for the absence or presence of the QRS complex. An absent QRS is a sign of some type of second-degree or third-degree AV block. It also may indicate that there is a severe ventricular disturbance such as ventricular fibrillation or asystole. Scrutinize the QRS complexes to see if they have an identical appearance. QRS complexes with different appearances indicate a shift from the normal pathway for ventricular contraction to a different pathway progressing through the ventricle (e.g., a bundle branch block). This also may be a sign of a different origin of the ventricular beat (e.g., PVCs or other beats of ventricular origin). Step 3: Examine the relationship between P waves and QRS complexes. Determine if the P waves and QRS complexes are “married.” Is there a P for every QRS? Is there a QRS for every P? Is there a 1:1 P:QRS ratio? If there are more P waves than QRS complexes (i.e., a P:QRS ratio of more than 1), then some sort of AV block is present. If there are more QRS complexes than P waves (i.e., a P:QRS ratio of less than 1), then a junctional or ventricular arrhythmia is present. Step 4: Measure the PR and QRS intervals. Inspect the PR interval. Is it too long or too short, or does it have a normal duration? There may be a junctional beat (retrograde P wave) if the PR interval is shortened. The presence of an accessory pathway [such as in Wolff-Parkinson-White (WPW) syndrome] also may explain the shortened PR interval. If the PR interval is lengthened, then there is some type of AV block. Determine if the QRS interval is normal or too long; only in rare cases will it be too short. If the QRS complex has an increased duration, then either bundle branch block or a beat of ventricular origin is likely present. In some cases, a QRS complex with an increased duration may be a sign of an aberrantly conducted beat of supraventricular origin; this occurs when the beat originates before the ventricular conductive pathway is repolarized (during the relative refractory period). Step 5: Detect a regular or irregular rhythm. Study the intervals from P wave to P wave and from R wave to R wave. If the intervals are constant, then the rhythm is regular. If the intervals vary, then the rhythm is irregular. To determine the regularity of these intervals, simply print out a screenshot and measure with calipers or a ruler. You can even use a 3x5 index card or a piece of paper; hold it up on a stationary screen view and mark a P wave and then the next one. Then move the card from P to P to P or R to R to R and see if the marks fall in line. Step 6: Determine the rate. Do not rely on the cardiotachogram to determine the heart rate, which is usually derived from the pulse oximeter. It is prone to errors such as a decreased or increased peripheral pulse sensing, or an undercount or overcount of the heart rate. Count the actual rate in a 10second period and multiply by six; or in a 15-second period and multiply by four. Arrhythmias Arrhythmias are present if the rate is too fast or too slow, the site of origin is other than the SA node, the pathway of electrical conduction is altered, or there is a combination of any of these features. Continued on page 32... A2Zzz 2008 • volume 17 • number 1 31 Continued from page 31... To learn more about specific arrhythmias in each of the following categories, see the detailed features for arrhythmia recognition and figures of brief graphic samples in chapter 36, “Cardiac Arrhythmias,” in the Fundamentals of Sleep Technology textbook (Lippincot Williams & Wilkins, 2007). Atrial Arrhythmias Atrial arrhythmias are characterized by ectopic P waves (i.e., those originating from locations in the atria some place other than the normal SA node) and therefore have a different morphology or shape. The exceptions are atrial fibrillation (i.e., no distinct P waves), atrial flutter (i.e., appearance of saw tooth waves instead of P waves) and sinus pauses (i.e., absence of P waves due to arrest of the SA node or blockage of the discharge of the SA node preventing depolarization of the atrium). Junctional Arrhythmias In junctional arrhythmias, the QRS complex will have the same morphology as that in the patient’s sinus rhythm because the pathway from the AV node to the ventricular myocardium is not altered. The P waves will either be absent (i.e., buried in the QRS complex), inverted, or perhaps, will follow the QRS complex. If the inverted P wave is seen, the P-R interval will also be shorter than normal. References American Academy of Sleep Medicine. The AASM manual for the scoring of sleep and associated events: rules, terminology and technical specifications. Westchester, Ill: American Academy of Sleep Medicine; 2007. Atkinson JW. Cardiac arrhythmias. In: Butkov N, LeeChiong T, editors. Fundamentals of sleep technology. Philadelphia: Lippincot Williams & Wilkins; 2007. p. 314-332. Atkinson, J. Appendix II Cardiac Arrhythmias. In: Barkoukis T, Avidon A, editors. Review of sleep medicine. 2nd ed. Burlington, Mass.: Butterworth-Heinemann; 2007. p. 545-560. Atkinson JW. Cardiac arrhythmias. Respir Care Clin N Am 2005;11(4):635-662. Thaller M. The only EKG book you’ll ever need. 4th ed. Philadelphia: Lippincot Williams & Wilkins; 2003. Dubin D. Rapid interpretation of EKG. 6th ed. Tampa, Fla.: Cover Publishing; 2000. Jon Atkinson, BS, RPSGT, is the AAST President. He has been in the sleep field for 27 years, and he currently works as a self-employed consultant in sleep medicine technology. AV Blocks With AV blocks the electrical conduction between the atria and the ventricles is either delayed (i.e., prolonged P-R interval) or totally absent. In 1st-degree AV block, the P-R interval is greater than 0.20 seconds. There are no lost QRS complexes. Second-degree blocks are always accompanied by the loss of at least one QRS complex. The Wenckebach phenomenon (2nd-degree AV block, Mobitz type I) demonstrates a progressively lengthening P-R interval as the AV node becomes increasingly refractory to conduction until a QRS complex is no longer generated. In 2nd-degree AV block type II, the P-R interval remains constant (i.e., it may be either normal or prolonged) and there is a sudden loss of one or more QRS complexes (i.e., visible P waves without corresponding QRS complexes). In AV dissociation (i.e., complete AV block, 3rd degree AV block), there is no relationship between the P wave and the QRS complexes. The P-P interval is usually quite constant as is the R-R interval; however, the duration of the P-P interval and the R-R interval is different giving the appearance of P waves “marching” through the rest of the EKG waveforms. Ventricular Arrhythmias Ventricular arrhythmias demonstrate the absence of P waves and widened, bizarre-appearing QRS complexes as they are generated from ventricular foci that circumvent the normal “rapid transit” pathway from the AV node to the Purkinje fibers. This causes a slower depolarization of the ventricle and thus a prolonged QRS interval. It should be noted that the T wave will not have its normal morphology either since the repolarization waveform must necessarily be aberrant as well. 32 A2Zzz 2008 • volume 17 • number 1 CORRECTION In Figure 1 of “Scoring Center: Scoring Cardiac Dysrhythmias – Part 1 of 2” (A2Zzz 2007;16(4):31), the arrow showing the direction of electrical impulse for modified lead 1 points in the wrong direction. The arrow should point from negative to positive, which would be from the patient’s right subclavicular to left subclavicular. The corrected figure is shown here. I (-,-) (+,-) III II (+,+) FIGURE 1. Locations for electrode placements The red line is a modified lead 2 (recommended), the blue line is a modified lead 1, and the green line is a modified lead 3. The polarity of the electrode in each dipole is indicated in parentheses.