Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Quantium Medical Cardiac Output wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Coronary artery disease wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Jatene procedure wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Myocardial infarction wikipedia , lookup
Atrial fibrillation wikipedia , lookup
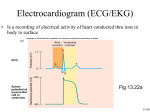
Cardiac Surgery Technical Note Interpreting an ECG Tracing An electrocardiogram (ECG) graph of potential cardiac difference (voltage) against time measures the waves of electrical excitation passing through the heart. It consists of: P Wave: Atria Interpretation Electrical impulse conduction from the SA Node through-out the atria is seen on the ECG as the P wave (Fig. 1). 1) The shape and duration of P waves may indicate atrial enlargement. 2) Absence of a P wave may indicate atrial fibrillation. 3) A saw toothed P wave may indicate atrial flutter. PR Segment: AV Node Delay The AV node delays electrical conduction so that the atria and ventricles don’t contract at the same time, and blood flows effectively from the atria to the ventricles. The delay in the AV node forms much of the PR segment on the ECG. Part of atrial repolarization can also be represented by PR segment. It is usually 120 to 200 ms long. A PR interval of over 200 ms may indicate a first degree heart block. A short PR interval may indicate a pre-excitation syndrome via an accessory pathway Fig. 1: A typical ECG tracing of a normal heartbeat (shown that leads to early activation of the ventricles. Variable PR above) consists of a P wave, a QRS complex and a T intervals may indicate other types of heart block. PR segment wave. depression may indicate atrial injury or pericarditis. QRS Complex As the branches of the Bundle of His taper out to produce numerous Purkinje fibers, individual groups of myocardial cells are stimulated to contract. This spread of electrical activity throughout the ventricular myocardium produces the QRS complex. The QRS complex takes 0.08 to 0.12 sec (80 to 120 ms). Not every QRS complex contains a Q wave, a R wave, and a S wave. The duration, amplitude, and morphology of the QRS complex is useful in diagnosing cardiac arrhythmias, conduction abnormalities, ventricular hypertrophy, myocardial infarction and other disease states. ST Segment The ST segment connects the QRS complex and the T wave and has a duration of 0.08 to 0.12 sec (80 to 120 ms). Flat, down-sloping, or depressed ST segments may indicate coronary ischemia. ST segment elevation may indicate myocardial infarction. T Wave: Ventricle Repolarization (Recovery) Absolute refractory period: from the beginning of the QRS complex to the apex of the T wave. Relative refractory (vulnerable) period: last half of the T wave. 1) T waves can signal coronary ischemia, Wellens’ syndrome, left ventricular hypertrophy, or CNS disorder. 2) Tall or “tented” symmetrical T waves may indicate hyperkalemia. 3) Flat T waves may indicate coronary ischemia or hypokalemia flutter. Reference: Wikipedia ECGInterpretation(CV-58-tn)RevC2013USltr www.transonic.com