Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
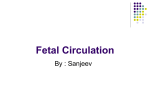
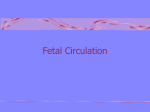
By: Nicole Stevens To have an understanding of the anatomy and physiology of fetal circulation To identify the 3 fetal shunts To have an understanding of newborn transition and conversion of fetal to neonatal circulation Identify impediments to this transition 3 4 Includes: Placenta Umbilical Vein (X1) Ductus Venosus Foramen Ovale Ductus Arteriosus Umbilical Arteries (X2) Human fetal circulation works differently to extrauterine circulation, and there are 3 key differences: The presence of a placenta in the “circuit” Blood flowing through the foramen ovale between the right atrium and the left atrium Blood bypassing through the ductus arteriosus from the pulmonary artery to the aorta There are also many other embryonic circulatory vessels; these are slowly obliterated postnatally and remain in the adult only as fibrous remants ROLES OF THE PLACENTA: Secretes endocrine hormones which increase through the pregnancy, causing progressive changes in maternal metabolism; this creates an increase in the maternal glucose and amino acids available to the foetus The placenta facilitates the exchange of oxygen and carbon dioxide between the mother and fetus. The presence of fetal Hb in the fetal blood supply ensures the movement of oxygen from mother to fetus because the fetal Hb has a higher affinity to oxygen than adult Hb. The placenta is responsible for the provision of nutrients such as water, glucose, vitamins and electrolytes. The placenta also manages waste disposal of products such as urea, uric acid and bilirubin These substances diffuse between maternal and fetal blood through the placental membrane. Adequate blood flow throughout the pregnancy to the placenta is vital to maintain healthy growth and development of the fetus ROLES OF THE PLACENTA cont..: The maternal and fetal circulations are not joined, instead, the respiratory gases, carbohydrates, lipids, vitamins, minerals and amino acids diffuse across the placental membrane The placenta is a low resistant component of fetal circulation The fetal heart generates the force to pump blood through the umbilical arteries (2) to the placenta Blood returns from the placenta to the fetus via the umbilical vein Transports O2 rich blood & nutrients Enters ductus venosus 80% saturated with O2 10 Approximately 45% of blood from the umbilical vein enters the portal circulation allowing the liver to process nutrients. Approximately 55% of the blood passes thru the Ductus Venosus, a shunt which bypasses the liver. The ductus venosus travels a short distance and joins the Inferior Vena Cava. 11 From the inferior vena cava the blood flows into the right atrium and is shunted directly into the left atrium through an opening called the foramen ovale. Foramen Ovale R ►L shunt There is a valve with two flaps that prevents backflow. 12 The fetus has high pulmonary vascular resistance due to partially collapsed alveoli There is decreased blood flow to lungs It is a relatively hypoxic environment The pulmonary vessels are relatively constricted Pulmonary Vascular Constriction 13 DUCTUS ARTERIOSUS: Connects the pulmonary trunk to the descending aorta Allows bypassing of the non-functioning lungs Returns blood to the placenta for oxygenation Systemic circulation returning to the heart goes into the right atrium then the right ventricle, this is pumped into the pulmonary artery; blood wants to travel on the path of least resistence, there is high resistence in the lungs of the fetus and low resistence in systemic circulation, the blood will prefer to flow across the ductus arteriosus into the aorta, rather than down the right and left pulmonary arteries to the lungs. 15 Return deoxygenated blood from Descending Aorta to placenta The blood is then reoxygenated in the placenta 16 FETAL CIRCULATION THE PATH: (may help to track it on your heart drawings) Deoxygenated fetal blood is carried to the placenta by the two umbilical arteries; these arise from the internal iliac arteries Gas exchange occurs in the placenta Oxygenated blood travels from the placenta via the umbilical vein and enters the IVC About 50% of this passes through the liver and the rest bypasses the liver via the ductus venosus; the IVC also drains blood returning from the lower part of the body THE PATH cont.. On reaching the heart at the right atrium the blood is divided into 2 streams (of unequal sizes); the larger stream is shunted to the left atrium through the FO, the smaller stream joins the flow of blood returning from the SVC (returning from the myocardium and upper body) The blood that goes through the FO ends up in the left ventricle and is ejected into the aorta The blood that goes into the right ventricle is pumped into the pulmonary artery but most will go across the DA and end up in the aorta as well Most of the relatively O2 rich blood that comes up the ascending aorta from the left ventricle will end up at the head and upper extremeties (the vessels feeding these areas come off the aorta prior to the DA union point) The patency of the DA is maintained by the relatively low O2 tension and the vasodilating effects of prostaglandin E2 (maternal hormone coming through the placenta) The newborn, must make five major adjustments at birth. 1) World of air 2) Circulation 3) Wastes 4) Body temperature 5) Response to infection 21 Fetal Low pressure system Lungs non-functional Right to left shunting in the heart High pulmonary resistance Low systemic resistance Neonate High pressure system Lungs functional Left to right blood flow in the heart Low pulmonary resistance High systemic resistance At birth, the circulation of fetal blood through the placenta ceases; the umbilical vessels are obliterated when the cord is clamped externally There is a reduction in blood flow through the IVC and the ductus venosus (this will close within 3 – 10 days) There is a dramatic fall in PVR with lung expansion (opening up of pulmonary vessels) A reduction in hypoxic pulmonary vasoconstriction and stimulation of pulmonary stretch receptors contribute to this process At birth the first breaths are the catalyst for the transition to neonatal circulation Lungs inflate with oxygen with an increased atmospheric pressure Lungs now become a low-pressure system as pulmonary vessels dilate with rise in oxygen level Alveolar fluid is displaced 24 At birth, the circulation of fetal blood through the placenta ceases; the umbilical vessels are obliterated when the cord is clamped externally There is a reduction in blood flow through the IVC and the ductus venosus (this will close within 3 – 10 days) There is a dramatic fall in PVR with lung expansion (opening up of pulmonary vessels) A reduction in hypoxic pulmonary vasoconstriction and stimulation of pulmonary stretch receptors contribute to this process The rise in pulmonary blood flow leads to an increase in blood returning to the left atrium; the left atrial pressure therefore exceeds the right atrial pressure; this reversal of pressure causes the flap of the FO to be pushed closed (the initial closure occurs within minutes, anatomical closure takes several days The ductus arteriosus constricts due to the high partial pressure of oxygen (the failure of this to occur will be discussed in the presentation on PDA) Highly oxygenated arterial blood in the Ductus Arteriosus causes it to constrict. Cessation of circulating PGE2 from maternal circulation. And increased metabolism of circulating prostaglandins by the lungs Bradykinin – released on lung inflation Within 10-15 hours the DA constricts and will eventually become the Ligamentum Arteriosus 27 Increased blood flow of oxygenated blood returning from the lungs Increases the pressure to the left side of the heart forces blood against the Septum Primum causing the Foramen Ovale to close and become Fossa Ovalis 28 NEONATAL CIRCULATION Lungs inflate decrease in pulmonary vascular resistance and increase in pulmonary vascular flow Blood O2 levels rise further decrease in pulmonary vascular resistance and ductus arterious constricts Increased pressure in LEFT atrium and decreased pressure in RIGHT atrium formamen ovale closes Umbilical cord is clamped ductus venosus closes increased systemic vascular resistance 30 What happens to these special structures after birth? Umbilical arteries atrophy Umbilical vein becomes part of the fibrous support ligament for the liver The foramen ovale, ductus arteriosus, ductus venosus atrophy and become fibrous ligaments 31 Foramen ovale Closes shortly after birth, fuses completely in first year. Ductus arteriousus Closes soon after birth, becomes ligamentum arteriousum in about 3 months. Ductus venosus Ligamentum venosum Umbilical arteries Medial umbilical ligaments Umbilical vein Ligamentum teres The Five H’s Hypothermia Hypoxia Hypoglycaemia Hypotension Hypercarbia 33 Blood flow to all organs is reduced Lack of adequate organ perfusion & tissue oxygenation Brain damage & multisystem organ damage DEATH Inter-uterine distress: abnormal presentations, maternal haemorrhage/seizures, ascending infection, cord prolapse Congenital cardiac abnormalities: HLHS, coarction of the aorta, TGA, TOF Pulmonary abnormalities: hypoplastic lungs, congenital pneumonia, decreased surfactant production (prematurity/diabetic mother) Insufficient ventilation and/or airway blockage Excessive blood loss or poor cardiac contractility Sustained constriction of pulmonary arterioles BEWARE THE UNDIAGNOSED CARDIAC ABNORMALITY – IF THEY ARE DUCT DEPENDENT DISORDERS THESE BABIES WILL DETERIORATE AS THE DUCT CLOSES In some circumstances a neonates circulation may revert back to be fetal-like; this state is known as persistent foetal circulation (PFC) A neonates pulmonary arterioles remain very reactive and will constrict in response to: hypoxia, hypercarbia, acidosis and cold; this can lead to an increase in PVR, which favours right to left shunting through the FO and ductus arteriosus The result of this is the neonate reverting to PFC, with one major difference – there is no placenta to provide oxygenation; a vicious cycle of worsening hypoxia and acidosis is then set in motion. The management of this requires treatment of the underlying causes: Such as, escalating respiratory support to provide better ventilation (and reduce hypercarbia) Use of nitric oxide if there is pulmonary hypertension, to aid in dilating the pulmonary vessels (nitric is inhaled through the ventilation circuit) Management of infection with antibiotics Management of thermoregulation American Academy of Pediatrics Textbook of Neonatal Resuscitation 4th Ed (2000) NRP Slide Presentation Kit Askin,D.F. (2001) Complications in the Transition from Fetal to Neonatal Life JOGNN Vol33(3) 318-327 Blackburn,S. (2006) Placental Fetal and Transitional Circulation Revisited. Perinatal Neonatal Nursing Vol20 (4) 290-294 Witt C. (1997) Cardiac Embryology. Neonatal Network Vol16(1) 43-49 Merenstein, G.B & Gardner, S.L, (2002), Handbook of Neonatal Intensive Care , 5th Ed, Mosby, St. Louis. www.echocharity.org.uk http://www.nhlbi.nih.gov/health/dci/Diseases/pda/pda_heartworks.html http://user.gru.net/clawrence/vccl/chpt1/fetcirc.HTM http://www.cayugacc.edu/people/facultypages/greer/biol204/heart4/heart4.html http://www.indiana.edu/~anat550/cvanim/fetcirc/fetcirc.html http://www.embryology.ch/anglais/pcardio/umstellung01.html http://mcb.berkeley.edu/courses/mcb135e/fetal.html http://www.indiana.edu/~anat550/cvanim/f etcirc/fetcirc.html http://www.embryology.ch/anglais/pcardio/ umstellung01.html http://www.youtube.com/watch?v=T79sMqvN 3BE 41