Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
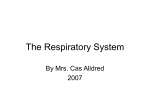
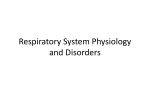
TELEFLEX Academy Ventilation Clinical Workshop Pre-Reading Package IMPORTANT NOTE: Every effort has been made by the author to ensure the information presented in this package is accurate and up to date. New research and experience in the medical field however, results in necessary changes to treatments and therapies. It is the responsibility of the professional, relying on experience and knowledge of the patient, to determine the best treatment for each individual patient. The author accepts no liability for any consequences from the application of the information in this package. Prepared by Chris Ridgway © 2014 Teleflex Academy 4 Secombe Place • Moorebank New South Wales • 2170 Ph 1300 360 226 TELEFLEX Academy Ventilation Workshop Pre-Reading Package Table of Contents INTRODUCTION ..................................................................................................................................... 5 CHAPTER 01 RESPIRATORY PHYSIOLOGY Breathing ............................................................................................................................................. 7 Inspiration .................................................................................................................................... 7 Expiration ..................................................................................................................................... 8 Active Breathing ........................................................................................................................ 9 Lung Volumes ........................................................................................................................... 10 Respiration ........................................................................................................................................... 11 External Respiration .............................................................................................................. 11 Internal Respiration ................................................................................................................ 14 Cellular Respiration ................................................................................................................ 10 Gas Transport.......................................................................................................................................... 14 Oxygen Transport .................................................................................................................... 14 Carbon Dioxide Transport.................................................................................................... 16 Control of Breathing .......................................................................................................................... 17 Central Control of Breathing................................................................................................ 17 Local Control of Breathing................................................................................................... 18 Review Questions ................................................................................................................................ 19 CHAPTER 02 PATHOPHYSIOLOGY Pathophysiology ...................................................................................................................................23 Oxygenation Impairment ..................................................................................................... 23 Ventilation Impairment ......................................................................................................... 23 Acute Respiratory Failure .................................................................................................... 24 Common Respiratory Disorders ..................................................................................................24 Atelectasis.................................................................................................................................... 24 Acute Pulmonary Oedema ................................................................................................... 25 Pneumonia ................................................................................................................................. 25 Asthma ......................................................................................................................................... 25 Chronic Bronchitis .................................................................................................................. 26 Emphysema ............................................................................................................................... 26 Chronic Obstructive Pulmonary Disease (COPD) ...................................................... 26 Acute Respiratory Distress Syndrome (ARDS) ........................................................... 26 Review Questions ................................................................................................................................27 GLOSSARY ...........................................................................................................................................29 REFERENCES ....................................................................................................................................... 35 4 | 5 TELEFLEX Academy Ventilation Workshop Pre-Reading Package Introduction This package provides an introduction to the concepts and principles of ventilation. It has been designed to be used as a prelearning package, prior to attendance at a Teleflex Academy ventilation workshop. There are practical application notes and review questions located throughout the package to help you apply the information presented. They can be identified by an icon from the key on the right. A glossary of common respiratory and ventilation terminology has also been included to assist you in your learning. During the workshop it will be assumed that all participants have read and have a good understanding of the content included in the pre-learning package. If you have any questions whilst completing the package, please bring your questions along to the training. We look forward to seeing you soon. Regards, The Teleflex Academy Team Icon Key Application note Test your knowledge 6 | 7 TELEFLEX Academy Ventilation Workshop Pre-Reading Package Respiratory Physiology 01 Cells within the body require oxygen in order to access the energy they need from nutrients (during cellular metabolism). The body is unable to store oxygen for long periods of time; therefore it needs a continuous supply of oxygen. CHAPTER A REVIEW OF THE PHYSIOLOGY OF THE RESPIRATORY SYSTEM Metabolism produces carbon dioxide, which becomes an acid in the blood and must be removed from the cells. Respiration is the process of gas exchange between the atmospheric air and the blood and between the blood and the cells of the body to provide oxygen to and remove carbon dioxide from the cells. In order to work effectively it requires: • Patent airway system to transport air to and from the lungs. • Effective alveolar system in the lungs to allow diffusion of gases into and out of the blood. • Effective cardiovascular system to carry nutrients and wastes to and from the body cells The process of gas exchange has five components: • Breathing • External Respiration • Internal Respiration • Cellular Respiration • Gas Transport Negative pressure generated during inspiration also assists in the venous return of blood to the heart BREATHING Breathing, or ventilation, is the movement of air through the airways between the atmosphere and the lungs. The air moves through the passages because of pressure differences between the atmosphere and the gases inside the lungs that are produced by contraction and relaxation of the diaphragm and thoracic muscles. There are two phases of breathing; inspiration and expiration. INSPIRATION Inspiration is the process of taking air into the lungs. It is the active phase of ventilation because it is the result of muscle contraction. During inspiration, the diaphragm and intercostal muscles contract, enlarging the thoracic cavity. The diaphragm, doing most of the respiratory work during quiet breathing, moves downwards increasing the volume of the thoracic (chest) cavity, and the intercostal muscles pull the ribs up expanding the rib cage, further increasing this volume (see Figure 1.1). This increased capacity lowers the air pressure in the alveoli to below atmospheric pressure. This decrease in intra-alveolar pressure draws air into the lungs as air, like other gases, flows from a higher pressure region to a lower pressure region. 8 | 9 FIGURE 1.1 Process of inspiration (Image from Marieb, 2004) EXPIRATION Expiration is the process of letting air out of the lungs during the breathing cycle. During expiration the diaphragm and intercostal muscles relax. This returns the thoracic cavity to its original volume, increasing the air pressure in the lungs (see Figure 1.2) . The increase in intra-alveolar pressure pushes air out of the lungs. Expiration normally takes twice as long as inspiration. FIGURE 1.2 Process of expiration (Image from Marieb, 2004) TELEFLEX Academy Ventilation Workshop Pre-Reading Package ACTIVE BREATHING The body needs to be able to rapidly respond to changes in activity and therefore demand for energy. This means that when there is an increased demand for oxygen due to increased cellular metabolism, for example during exercise or illness, there also needs to be a corresponding increase in supply of oxygen. The increased metabolism will also result in increased production of carbon dioxide, which must also be removed. In order to increase gas exchange to meet the increased demand, extra muscles are used to increase the capacity of the respiratory system. The use of these extra muscles is often referred to as active breathing. During active breathing accessory muscles are used during inspiration to lift the rib cage, creating a larger space within the thorax, further decreasing the pressure and causing a more rapid flow of air into the lungs. Expiration during active breathing becomes an active rather than passive action, with contraction of muscles to rapidly decrease the size of the thorax, thereby increasing the pressure and forcing air out of the lungs. The use of accessory muscles in the absence of exercise can be an indication of respiratory failure ic FIGURE 1.3 Muscles used during quiet and active breathing. (Image from Ingraham, 2004) 10 | 11 LUNG VOLUMES Air movement in and out of the lungs is determined by the pressure gradient between the atmosphere and the alveoli. The volume of air inhaled and exhaled with each breath is called the tidal volume. The pressure gradient, and therefore respiratory effort, required to obtain a particular tidal volume may be affected by the lung compliance and the resistance of the airways. Lung compliance is the distensibility or “stretchability” of the lung and the elastance, or elastic recoil back to its original shape. Lung compliance is affected by connective tissue and alveolar surface tension. A highly compliant lung will expand easily when pressure is applied; however a poorly compliant lung requires a greater than normal pressure, and therefore effort, to expand it. Lung volumes will be affected by the compliance & resistance of the airways The resistance of the airways refers to the opposition to gas flow through the airways. It is primarily determined by the radius of the airway, with a smaller bronchial diameter increasing the resistance or opposition to air flow, therefore slowing down the air flow for a particular pressure gradient. An airway with high resistance will therefore require greater than normal pressure gradient and effort to achieve normal levels of ventilation. APPLICATION NOTE When using an artificial airway a small diameter tube will increase the resistance to airflow causing higher airway pressures to deliver the same volume or, if the pressures are being controlled, will result in a reduced volume being delivered FIGURE 1.4 Normal lung volumes and capacities for an adult male (Image from Marieb, 2004) MEASUREMENTS OF LUNG VOLUMES AND CAPACITY Individual components of the mechanics of ventilation can be measured to allow the evaluation of lung function. Lung volumes are measured during normal quiet breathing and then during maximal inspiration and expiration. From the four volumes measured (tidal volume, inspiratory reserve volume, expiratory reserve volume, and residual volume), the lung capacity in relation to inspiration and expiration can be calculated (see Figure 1.4). TELEFLEX Academy Ventilation Workshop Pre-Reading Package Respiration EXTERNAL RESPIRATION Once the air has reached the alveoli gas exchange between the air and blood, known as external respiration, can occur. In order for effective gas exchange, there not only needs to be good ventilation but also good perfusion, or circulation, to the ventilated alveoli. The movement of oxygen and carbon dioxide between the alveoli and capillaries is controlled by diffusion, with gas moving across the alveolar membrane from areas of high concentration to areas of low concentration. Gas diffusion is affected by: • Concentration gradient • Thickness of barrier • Surface area available for exchange • Ventilation-Perfusion matching • Solubility of gas CONCENTRATION GRADIENT Gas concentrations are expressed as partial pressures. In a mixture of gases, each gas contributes to the total pressure according to its concentration. For example if a gas is 50% of total, it produces 50% of the pressure. The pressure of room air, or atmospheric pressure, at sea level is 760 mmHg. This pressure is made of different concentrations of gases – with approximately 78% nitrogen, 21% oxygen, 0.03% carbon dioxide and 0.05% water vapour. The partial pressure of oxygen in room air is therefore 21% of 760 mmHg, or 160 mmHg. When air enters the trachea it is humidified, becoming fully saturated with water vapour. The water vapour, now taking up approximately 6% (47 mmHg) of the pressure, displaces other gases and reduces their concentrations (Smeltzer & Bare, 1992). In the alveoli there is some residual carbon dioxide, which further alters the balance of concentrations, with the resulting partial pressures within normal alveoli: • • • • Nitrogen, 569 mmHg (74.9%); Oxygen, 104 mmHg (13.6%); Carbon dioxide, 40 mmHg (5.3%); Water vapour, 47 mmHg (6.2%). FIGURE 1.5 Diffusion of oxygen and carbon dioxide accross the alveolar membrane (Image from Marieb, 2004) The speed of oxygen and carbon dioxide diffusion across the alveolar membrane is affected by the size of the concentration gradient. The bigger the difference between concentrations on either side, the faster the gas will move. The biggest gradient, and therefore fastest diffusion of gas, occurs when fresh gas is brought in to the alveoli during inspiration. In the alveolar capillaries the blood is returning, through the right side of the heart, from the tissues, where oxygen has been used and carbon dioxide produced during cellular metabolism. The capillary oxygen levels are therefore usually low, and the carbon dioxide levels high in comparison to the alveolar gases. The differences in concentration, or concentration gradients, cause movement of oxygen from the alveoli into the blood, and carbon dioxide from the blood into the alveoli. 12 | 13 GAS EXCHANGE SURFACE The alveolar-capillary membrane is ideal for diffusion as it has a thin membrane, as thin as 0.3 micrometers in some areas, and a large surface area of 50-100 m 2 in a normal lung. For gas to get between the air and the red blood cells it must diffuse through the following layers (see Figure 2.5): Alveolar space Surfactant Fused basement menbranes Nucleus of endothelial cell Alveolar epithelium 0.1-1.5µm Capillary Endothelium • • • • • • • Alveolar fluid Alveolar epithelium Alveolar basement membrane Interstitial space Capillary basement membrane Capillary endothelium Plasma Any changes to the surface area or layers will affect the diffusion of gases. FIGURE 1.6 Layers of the alveolar-capillary membrane SURFACE AREA FOR GAS EXCHANGE The total amount of diffusion that occurs accross the membranes is proportional to the size of the surface through which it can diffuse, or the surface area for gas exchange. The more gas that can come in to contact with the blood, the more gas will be able to move into and out of the blood. As discussed previously, the gas exchange units in the lung provide an environment for efficient gas exchange. The alveoli have a huge surface area of around 160m², each surrounded by a mesh of pulmonary capillaries, with as many as 1000 capillaries coming in to contact with each alveoli. In order to minimise the distance for gas diffusion, each capillary is only big enough to fit one red blood cell at a time. As the red blood cell travels the full length of the capillary (from the pulmonary arterial to venous system) it may have come into contact with several alveoli. In a normally functioning body at rest the haemoglobin (Hb) on the red blood cells will be fully saturated by the time it has travelled a third of the way along the pulmonary capillary. There is therefore extra reserve capacity for diffusion, which means that the Hb may still have time to be fully saturated despite mild problems with the alveolar-capillary membrane that slow diffusion, or a high cardiac output that reduces red blood cell contact time with the alveoli. The small capillary diameter and thinness and compliance of the avleolar-capillary walls means that alveolar pressures can affect capillary blood flow. If the pressure within the alveoli exceeds that of the pulmonary capillary, it can compress or collapse the capillary, blocking blood flow through that capillary. VENTILATION-PERFUSION MATCHING For gas exchange to be optimized the body must match the distribution of ventilation with perfusion, or blood flow in the pulmonary capillaries. Ideally each gas exhange unit would have an equal ratio of ventilation and perfusion. In a normal upright person however, the ventilation and perfusion are not equally distributed in the lung, with the average alveolar ventilation 4 L/min and perfusion 5 L/min. The healthy body is however able to compensate and redirect blood flow to maximise ventilation perfusion matching. The pulmonary circulation is a low-pressure system, able to vary its resistance to accommodate the blood flow received and alter the direction of blood flow to well ventilated areas. Due to the low pressures however, the distribution of blood is greatly affected by gravity, with minimal perfusion to the lung apices when in an upright position. It is also affected by alveolar pressure, as high alveolar pressures will cause compression of TELEFLEX Academy Ventilation Workshop Pre-Reading Package the capillaries and therefore restrict pulmonary blood flow to the area. Pathological changes to the airways or pulmonary circulation can further affect the balance, with two main types of mismatch occuring: • A blockage of ventilation to gas exchange units that still have good perfusion is referred to as a shunt. The alveoli cannot get any fresh gas and therefore blood travels past the alveoli without any gases being exchanged. • A blockage of perfusion to gas exchange units that still have good ventilation is referred to as dead space ventilation. Gas is able to get in to the alveoli, but it doesn’t have contact with blood, and therefore can not diffuse accross. • An absence of both ventilation and perfusion is referred to as a silent unit. Rather than there being a mismatch of ventilation and perfusion (as they are both equally absent) there is a reduction in surface area available for gas exchange. FIGURE 1.7 Matching of ventilation and perfusion. (Center) Normal matching of ventilation and perfusion; (Left) perfusion without ventilation (i.e. shunt); (Right) ventilation without perfusion (i.e. dead space). (Image from Porth, 2005) Monitoring of blood and exhaled gas concentrations in combination with assessing the affect of changes in inspired oxygen concentrations can help in identifying the cause, and therefore treatment, of a mismatch. In order to improve the matching of ventilation (represented by the letter V with a dot over it, v̇) to perfusion (represented by the letter Q), or the v̇/Q match, the pulmonary capillaries can constrict and dilate to help to direct blood flow toward well ventilated and away from poorly ventilated areas. The capillaries respond to localised changes in oxygen and carbon dioxide levels. • In areas with good ventilation there will be effective diffusion and therefore high levels of oxygen and low levels of carbon dioxide. The high oxygen and low carbon dioxide concentrations will cause the pulmonary capillaries to dilate, increasing blood flow to these well ventilated areas. • In areas with poor ventilation there will be limited diffusion and therefore low levels of oxygen and high levels of carbon dioxide. The low oxygen and carbon dioxide levels will cause the pulmonary capillaries to constrict, diverting blood away from these areas and towards better ventilated lung units. GAS SOLUBILITY The diffusion of a gas is also affected by the gas’s solubility. Oxygen and carbon dioxide must be able to dissolve into the alveolar fluid and then the blood in order to be transported to and from the tissues. When gas is exposed to a liquid, the gas will dissolve in the liquid until the concentration, or partial pressure, of the gas is the same in the liquid and the gas. This means that oxygen and carbon dioxide are exchanged across the alveolar membrane until the partial pressure is the same in the alveoli Carbon dioxide levels are largely and the blood. controlled by minute ventilation whereas oxygen is affected by Some gases dissolve more quickly and easily than others. surface area Carbon dioxide, for example, dissolves approximately 20 times faster than oxygen. It is therefore relatively unaffected by increased fluid in the alveoli or interstitial space, whereas oxygen diffusion may be affected. As carbon dioxide diffuses and equalises so quickly, the best way to remove more from the blood is to replace the air in the alveoli with new air to re-establish the concentration gradient and therefore restart the diffusion process. 14 | 15 INTERNAL RESPIRATION The process of gas exchange between the blood and the cells, or internal respiration, is the same as for external respiration. Movement of the gases is primarily affected by the concentration gradient between the blood and the cells. When oxygen-enriched blood comes in contact with tissue with a lower PaO2, oxygen will move from the blood into that tissue. Also, when the partial pressure of carbon dioxide (PaCO2) in the tissue exceeds that of the blood, carbon dioxide will move from the tissue into the blood to be transported to the lungs. Metabolic changes, as well as increases in interstitial fluids may affect the diffusion of oxygen into the cells, and therefore impair cell function. CELLULAR RESPIRATION Cellular respiration, or cellular metabolism, is the process of deriving energy, in the form of ATP, from molecules such as glucose. The cells break down glucose either with or without oxygen. When a glucose molecule is broken down without oxygen (anaerobic metabolism) 2 ATP molecules are produced, however in the presence of oxygen (aerobic metabolism) most cells can produce a further 34 ATP molecules. Oxygen is therefore essential for energyefficient metabolism to produce enough energy to maintain normal cell function. FIGURE 1.8 Layers of the alveolar-capillary membrane Gas Transport Oxygen and carbon dioxide are transported between the lungs and the cells in the blood stream. Some of the gas is transported dissolved in the plasma; however the majority is transported combined with some of the elements of the blood (see Figure 1.8). Gas transport is therefore reliant on the adequate functioning of the cardiovascular system. Changes to circulation (such as poor cardiac output) or components of the blood (such as anaemia) will affect the ability of gas to be transported to and from the lungs and cells. OXYGEN TRANSPORT The oxygen that is dissolved in the plasma of arterial blood, measured as a partial pressure or PaO2, is in a form that is readily available for diffusion to the tissues. The poor solubility of oxygen, however, limits the amount of oxygen that can be dissolved in the blood. The body therefore needs to have a reserve of oxygen that can be made available in periods of increased demand, such as exercise The average red blood cell contains or illness. Haemoglobin (Hb), found in the red blood cells, approx 250 million Hb molecules, each significantly enhances the oxygen carrying capacity of blood capable of carrying 4 oxygen molecules and providing a reserve supply. For every 100ml of blood, approximately 0.3mls of oxygen is physically dissolved in the plasma, however approximately 20mls of oxygen is present combined with haemoglobin (which becomes oxyhaemoglobin). At rest only 30% of the oxygen on the haemoglobin is normally used by the tissues. TELEFLEX Academy Ventilation Workshop Pre-Reading Package Haemoglobin is made up of iron-containing haem molecules combined with the protein globin. The iron in haem is able to reversibly bind an oxygen molecule. This means that oxygen can bind to Hb in the lungs and then be released at the tissues. There are four iron atoms in each Hb molecule comprising four haem groups. Each Hb molecule can therefore bind with four oxygen molecules. When oxygen is bound to all 4 haem groups, the Hb is said to be fully saturated. APPLICATION NOTE Pulse oximetry measures the oxygen saturation of arterial blood (SaO2 ), i.e. the percentage of oxygen carried by the available haemoglobin rather than the total oxygen available to the tissues. Hb levels and the PaO2 are not taken into account. In the loading and unloading of oxygen, there is cooperation between the four haem groups. When oxygen binds to one of the groups, the others change shape slightly and their attraction to oxygen increases. The loading of the first oxygen results in the rapid loading of the next three (forming oxyhaemoglobin). At the other end, when one haem group unloads its oxygen, the other three rapidly unload as their groups change shape again having less attraction for oxygen. This method of cooperative binding and release can be seen in the dissociation curve for haemoglobin (see Figure 1.9). Over the range of oxygen concentrations where the curve has a steep slope, the slightest change in concentration will cause haemoglobin to load or unload a substantial amount of oxygen. OXYHAEMOGLOBIN DISSOCIATION PaO2 SaO2 150mmHg 100% 100mmHg 97% 60mmHg 90% 40mmHg 70% TABLE 1.1 Relationship between PaO2 and SaO2 The major factor that determines the movement of oxygen onto the haemoglobin is the amount of oxygen dissolved in the plasma (PaO2). As the concentration of oxygen in the plasma increases, more oxygen combines with the haemoglobin, until it is fully saturated i.e. oxygen is bound to all 4 haem groups. Haemoglobin usually becomes 100% saturated, under normal conditions, at a PaO2 of 150mmHg. In healthy person breathing room air, the expected arterial oxygen levels would be a PaO2 100mmHg (achieving equalisation with alveolar oxygen concentration) and a corresponding SaO2 of 97%. Table 1.1 shows the relationship between PaO2 and SaO2 at various levels: • At PaO2 150mmHg, even though the PaO2 has been increased by nearly 50%, there is minimal change in the SaO2 as the haemoglobin is almost completely saturated and cannot combine with any more oxygen. • PaO2 60mmHg, when the symptoms of hypoxia normally begin, although there is a drop of nearly half the dissolved oxygen concentration, the haemoglobin is still 90% saturated at this level. Small changes in SaO2 at this level correspond with large changes in PaO2. FIGURE 1.9 Oxyhaemoglobin dissociation curve (Image from Marieb, 2004) 16 | 17 APPLICATION NOTE In most clinical situations there is minimal benefit in increasing supplemental oxygen concentrations to achieve a SaO2 >97%. Delivering high concentrations of O2 may in fact cause oxygen toxicity,damaging the airways and impeding gas exchange. It is vital to the delivery system for the oxygen to bind and release from the haemoglobin at the right time and the right place. The oxyhaemoglobin dissociation system is designed to facilitate loading of oxygen onto the haemoglobin in the lungs, and offloading of oxygen in the systemic capillaries to supply the tissues. Factors such as the temperature, pH and carbon dioxide differ from the systemic to the pulmonary capillaries. The systemic capillaries provide oxygen for and carry wastes from cellular metabolism. It is here that we need oxygen to easily leave the haemoglobin. The conditions in the systemic capillary are greatly affected by the cellular metabolism that is occurring around it. There are low levels of dissolved oxygen (PaO2) as it is consumed by the cells, but high levels of carbon dioxide (and therefore a low, or acidic, pH) and heat produced during the metabolism. These factors, low oxygen, high CO2 and high temperature all affect the binding of oxygen to the haemoglobin, helping it to release easily. The pulmonary capillaries allow release of carbon dioxide into the atmosphere and bring oxygen into the circulation. The blood, having returned from the tissues, has low oxygen levels, however as carbon dioxide quickly and easily diffuses into the alveoli, the plasma CO2 level in the pulmonary capillary is low, as is the temperature as heat is lost over the membrane. In these conditions, oxygen binds more strongly to the haemoglobin, allowing the haemoglobin to be saturated with oxygen to then be transported back to the cells. Increased O2 affinity Decreased O2 affinity pH pH CO2 CO2 Temp Temp 2, 3 - DPG 2, 3 - DPG Changes to the level of 2,3-diphosphoglycerate (2,3-DPG), which is produced in the red blood cell, also affects the affinity of oxygen to haemoglobin. Low levels of 2,3-DPG can be found during sepsis as well as in blood transfusions, which makes oxygen bind more strongly to the haemoglobin, reducing its availability to the tissues. APPLICATION NOTE Sepsis can not only affect the ability to transport oxygenated blood to the cells, but can also affect the cells ability to receive and use the oxygen in the systemic capillaries, resulting in organ failure. CARBON DIOXIDE TRANSPORT Carbon dioxide created during cellular metabolism diffuses into the blood plasma with over 90% then entering the red blood cells. Once in the red blood cell approximately 23% binds to the multiple amino groups of haemoglobin to form carboxyhaemoglobin, whilst the majority (approximately 70%) is converted to bicarbonate ions and released into the plasma. The amount of carbon dioxide being transported in the blood is one of the major determinants of the acidbase balance of the body. When carbon dioxide enters the plasma, it reacts with water to form carbonic acid. Carbonic acid is a strong acid and readily donates its hydrogen ions. An increase in carbon dioxide levels within the blood will therefore cause an acidosis. As discussed previously, the carbon dioxide diffuses easily across the alveolar membrane, equalising quickly with the alveolar gas. The arterial carbon dioxide level is therefore usually equivalent to the partial pressure of carbon dioxide in the alveoli, i.e. 40 mmHg. TELEFLEX Academy Ventilation Workshop Pre-Reading Package Control of Breathing Breathing is controlled both centrally and locally in response to the stimulation of receptors located within the brain stem and the lungs. CENTRAL CONTROL OF BREATHING The respiratory centre is found in the brain stem. The pons and medulla oblongata are both integral to the control of breathing (Figure 1.10). The medulla oblongata rhythmically stimulates the intercostal muscles and diaphragm - making breathing possible. The pons also participates in the reflexes that regulate breathing. The brain stem receives signals from various organs in order to detect changes and respond to changes in physical demands of the body. It receives positive and negative stimuli to determine the respiratory rate and depth required. The rate of cellular respiration (and hence oxygen consumption and carbon dioxide production) varies with the level of physical activity. Vigorous exercise can increase tissue oxygen demand by 20-25 times that at rest. An increase in physical activity, and therefore cellular metabolism, will result in increased carbon dioxide levels and acidity, which is detected by peripheral and central chemoreceptors which, provide a positive stimulus to the brainstem to cause an increase in ventilation, i.e. increase in rate and depth of breathing. Stretch receptors in the lungs detect over distension, resulting in a negative stimulus to the brain stem, reducing the rate and depth of breathing, protecting against trauma to the airways. Irritant receptors in the bronchi and lungs will also cause a reduction in ventilation, to help prevent deep inhalation of irritants into the lower airways. FIGURE 1.10 The Respiratory Center is located in the medulla oblongata & pons of the Brain Stem (Image from Marieb, 2004) Breathing may be affected by emotional factors, such as fear, anxiety, or pain. Signals are transferred through the hypothalamus to the brain stem to affect ventilation. We are also capable of voluntary or conscious control over breathing. The brain stem receives signals from the higher brain centres to increase or decrease ventilation accordingly. 18 | 19 The most important factor in regulating ventilation is a rising concentration of carbon dioxide - not a declining concentration of oxygen. The concentration of carbon dioxide is detected by cells in the medulla by changes in the pH of the CSF. If the carbon dioxide level rises, the medulla responds by increasing the activity of the motor nerves that control the intercostal muscles and diaphragm. Carbon dioxide concentration is the primary stimulus to breathe However, the carotid body in the carotid arteries does have receptors that respond to a drop in oxygen. Their activation is important in situations where oxygen supply is inadequate but there has been no increase in the production of CO2 , for example at high altitude in the unpressurised cabin of an aircraft, or in situations of long term hypercapnia. FIGURE 1.11 Negative and positive stimuli to the brain stem affecting ventilation (Image from Marieb, 2004) Local Control of Breathing In addition to central control affecting the rate and depth of breathing, there is also a local control within the lungs. The smooth muscle in the walls of the bronchioles is very sensitive to the concentration of carbon dioxide. A rising level of CO2 causes the bronchioles to dilate. This lowers the resistance in the airways and thus increases the flow of air in and out. FIGURE 1.12 Primary mechanism for control of breathing (Image from Marieb, 2004) TELEFLEX Academy Ventilation Workshop Pre-Reading Package TEST YOUR KNOWLEDGE Try to answer the questions below without initially referring to the chapter. The short answer questions should be completed in your own words. MATCHING EXERCISES A. Affinity1. Alterations in this pulmonary function may be the result of airway obstruction, changes in lung compliance, and gravity B. Compliance 2. The capacity of haemoglobin to combine with oxygen that may be described as high or low C. Resistance 3. Alterations in this pulmonary function may be the result of changes in pulmonary artery perfusion, alveolar pressure, and gravity D. Ventilation 4. A property of the lung that is a measurement of dispensability or how easily a tissue is stretched E. Perfusion 5. A property of the lung that is determined mainly by the radius or the size of the airway through which the air is flowing TRUE/FALSE Please indicate whether the following statements are true or false. 1. Normal expiration takes twice as long as normal inspiration 2. In the erect adult, more air exchange occurs in the lower regions of the lungs than in the higher regions of the lungs because of gravity 3. The diffusing power of a gas is directly proportional to its partial pressure 4. Hypothermia, alkalosis, a decreased PaCO2 level, and a decrease in 2,3 diphosphoglycerate (2,3-DPG), result in an increased affinity of the haemoglobin for oxygen at any given PaO2 value, resulting in less oxygen released to the tissues 5. Central chemoreceptors located in the medulla respond to a low CSF pH by increasing, through medullary stimuli to the muscles of inspiration, both rate and volume 6. Hypoxia is the primary stimulus to breathe TRUE / FALSE 20 | 21 SHORT ANSWER/FILL-IN QUESTIONS 1. Describe the mechanism for spontaneous breathing. 2. Identify four conditions or situations that reduce pulmonary compliance. a. b. c. d. 3. Name four conditions that cause increased airway pressure. a. b. c. d. 4. Name four factors affecting alveolar–capillary gas exchange. a. b. c. d. TELEFLEX Academy Ventilation Workshop Pre-Reading Package SHORT ANSWER/FILL-IN QUESTIONS 5. Name four factors that affect the affinity of haemoglobin and oxygen. a. b. c. d. 6. Describe how oxygen and carbon dioxide are transported around the body. 7. What is internal and external respiration? 8. Draw or describe the movement of oxygen and carbon dioxide during internal and external respiration. 22 | 23 TELEFLEX Academy Ventilation Workshop Pre-Reading Package Pathophysiology 02 Effective gas exchange relies on each part of the respiratory process to be functioning. An interruption at any point will affect the ability of the body to supply oxygen to the tissues and remove carbon dioxide. CHAPTER Impaired pulmonary function can be classified into two main types: • • Oxygenation impairment – inadequate arterial oxygenation, or hypoxia. Ventilation impairment – inadequate carbon dioxide removal, or hypercapnia, in the presence of normal alveolar-arterial (A-a) gradient. OXYGENATION IMPAIRMENT Diffusion of oxygen, as previously discussed, is greatly affected by any changes to the air-blood barrier in the alveoli. Due to its poor solubility, any changes in the surface area, thickness of the barrier or increased fluid can result in inadequate oxygenation of the arterial blood. Not all of the oxygen can diffuse into the capillaries, with a higher concentration still left in the alveoli (called an A-a gradient). Treatment of oxygenation impairment requires supplementing oxygen (which increases the concentration gradient, speeding up oxygen diffusion) to ensure tissue hypoxia doesn’t occur, whilst treating the cause; e.g. increase surface area, reduce alveolar/interstitial fluid, improve ventilation-perfusion match. FIGURE 2.1 Oxygenation impairment in early ARDS (Image from Morton et al, 2005) VENTILATION IMPAIRMENT Ventilation impairment, or inadequate exchange of gas through the airways between the atmosphere and the lungs, is characterised by high arterial carbon dioxide levels, respiratory acidosis and increased work of breathing. The inadequate spontaneous ventilation may be caused by a reduced drive to breathe, as is found in CNS disorders; or a reduction in tidal volumes from neuromuscular, musculoskeletal, pleural, or conducting airways disorders. As carbon dioxide excretion is dependent on the amount of air it can exchange with, any changes to the respiratory rate or tidal volume (and therefore the minute ventilation) affects the arterial carbon dioxide level, resulting in hypercapnia. 24 | 25 Treatment of ventilation impairment is focused on increasing the respiratory rate by minimising any central respiratory depressants or improving tidal volumes by reducing the work of breathing and supporting the inspiratory effort. ACUTE RESPIRATORY FAILURE Respiratory failure is a syndrome in which the respiratory system fails in one or both of its gas exchange functions: oxygenation and carbon dioxide elimination. The lungs cannot maintain adequate alveolar ventilation. Hypoxic failure, characterised by low oxygenation, is also known as Type 1 Failure, and hypercapnic failure, characterised by high carbon dioxide levels, is also known as Type 2 Failure. Respiratory failure may be acute or chronic. Acute respiratory failure is characterised by life-threatening alterations in arterial blood gases and acid-base status and is the most common indication for mechanical ventilation in the Intensive Care Unit Acute respiratory failure can be defined as a PaO2 value of less than 60 mmHg while breathing air, or a PaCO2 of more than 50 mmHg. The manifestations of chronic respiratory failure are less dramatic and may not be as readily apparent. Common causes of acute respiratory failure include pneumonia, apnoea, neuromuscular dysfunction, head trauma, cardiac arrest, or drug-induced central nervous system (CNS) depression. Common Respiratory Disorders ATELECTASIS Atelectasis refers to the collapse of an area of lung, which could be an alveoli, lobule or larger lung unit. Atelectasis may result from: • Airway obstruction (eg. from sputum blocking a bronchiole), preventing airflow into the alveoli. The gas remaining in the alveoli eventually gets absorbed into the capillary, and with no fresh air to replace it, the alveoli collapse. Failure to adequately remove secretions, due to neurological or respiratory disorders, commonly causes atelectasis. • Compression of the lung tissue, limiting expansion and restricting air movement into the alveoli. The lung tissue may be compressed by air or fluid in the pleural space (i.e. pneumothorax or pleural effusion), enlarged heart, pericardial effusion, thoracic tumor, patient positioning preventing adequate lung expansion, or abdominal distension pushing the diaphragm upward. • Failure of the normal splinting mechanisms: - Loss or dilution of surfactant in the alveoli will increase the surface tension, causing collapse of the alveoli. - Loss of nitrogen in the alveoli due to inhaling high concentrations of oxygen. Nitrogen normally comprises approx 75% of the gas in the alveoli. It is a large molecule that does not diffuse across the alveolar membrane, assisting in splinting the alveoli open. If high concentrations of oxygen are delivered, there will be a consequential drop in the percentage of nitrogen. If all the alveolar oxygen diffuses into the capillary the alveoli before it is refreshed with new gas, the alveoli can collapse. - Decrease in alveolar pressure, which may cause collapse FIGURE 3.2 Atelectasis caused by airway obstruction on of the terminal bronchioles, which do not have any left, and compression on right (Image from Porth , 2005) cartilage to splint them open. TELEFLEX Academy Ventilation Workshop Pre-Reading Package ACUTE PULMONARY OEDEMA Acute pulmonary oedema (APO) is the abnormal accumulation of fluid in the lungs, either in the interstitial spaces or in the alveoli. An increase of fluid at the air-blood interface impairs the ability of oxygen to diffuse into the capillaries (with carbon dioxide being largely unaffected due to its high solubility). An increase in fluid within the alveoli causes a dilution of the alveolar surfactant, which may result in collapse of the alveoli. APO may be caused by left heart failure (cardiogenic APO) which results in increased pulmonary blood flow and pressure, causing fluid to leak out of the capillaries into the interstitial airways. Non-cardiac APO may also be caused by conditions that increase the pulmonary pressures, affect the colloid osmotic pressure (e.g. in nephritis), increase the permeability of the pulmonary capillaries (e.g. systemic inflammation) or damage to the capillary walls (e.g. inhalation of noxious gases, pneumonia and ARDS). FIGURE 3.3 Asthmatic bronchus (Image from Morton et al, 2005) PNEUMONIA Pneumonia is an infection of the alveoli. It can be caused by many kinds of bacteria (e.g., Streptococcus pneumoniae) and viruses. Fluid accumulates in the alveoli, reducing oxygen diffusion as well as diluting the surfactant causing collapse of the alveoli and therefore reducing the surface area exposed to air. Treatment includes clearance of secretions, and antibiotic treatment, if appropriate. If enough alveoli are affected, oxygenation is impaired and the patient may need supplemental oxygen. ASTHMA In asthma, periodic constriction of the bronchi and bronchioles makes it more difficult to breathe in and, especially, out. The swollen walls and increased secretions narrow the airways, increasing resistance and reducing air flow. During inspiration the airways are pulled open, however during expiration, the elastic recoil causes some obstruction of the airways, trapping air in the alveoli. The resultant ventilation impairment causes a rise in carbon dioxide levels. Attacks of asthma can be triggered by: • • • Food and environmental allergies ; eg. dust mites, pollens, animal dander Air borne irritants; e.g. chemical fumes, pollution, cigarette smoke Exercise Drugs; e.g. aspirin, β-blockers, NSAIDs 26 | 27 CHRONIC BRONCHITIS Any irritant reaching the bronchi and bronchioles will stimulate an increased secretion of mucus. In chronic bronchitis inflammation and thickening cause narrowing of the airways, with increased mucous secretions leading to a persistent cough. Oxygenation is impaired as diffusion is difficult through the secretions and due to alveolar collapse. Chronic bronchitis is usually associated with cigarette smoking. FIGURE 3.4 Inflammation & secretions seen in bronchitis (Image from Morton et al, 2005) EMPHYSEMA FIGURE 3.5 Lung changes in emphysema (Image from Morton et al, 2005) In emphysema, the delicate walls of the alveoli break down, reducing the gas exchange area of the lungs. They are grouped into three types according to where in the alveolar unit the tissue break down occurs. The condition develops slowly and is seldom a direct cause of death. However, the gradual loss of gas exchange area forces the heart to pump ever-larger volumes of blood to the lungs in order to satisfy the body’s needs. The added strain can lead to heart failure. CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) Irritation of the lungs can lead to asthma, emphysema, and chronic bronchitis; in fact, many people develop two or three of these together. This combination is known as chronic obstructive pulmonary disease (COPD). ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Acute respiratory distress syndrome is the clinical manifestation of severe, acute lung injury. It is characterised by the acute onset of diffuse, bilateral pulmonary infiltrates secondary to non-cardiogenic pulmonary edema, refractory hypoxia, and decreased lung compliance. Acute respiratory distress syndrome can result from direct chest trauma, prolonged or profound shock, fat embolism, massive blood transfusion, cardiopulmonary bypass, oxygen toxicity, or acute hemorrhagic pancreatitis. Most of these patients have no previous lung disease. At the onset of ARDS, lung injury may first appear in one lung, but then quickly spreads to affect most of both lungs. When alveoli are damaged, some collapse and lose their ability to receive oxygen. With some alveoli collapsed and others filled by fluid, it becomes difficult for the lungs to absorb oxygen and get rid of carbon dioxide. Within one or two days, progressive interference with gas exchange can bring about respiratory failure requiring mechanical ventilation. As the injury continues over the next several days, the lungs fill with inflammatory cells derived from circulating blood and with regenerating lung tissue. Fibrosis (formation of scar tissue) begins after about 10 days and can become quite extensive by the third week after onset of injury. Excessive fibrosis further interferes with the exchange of oxygen and carbon dioxide. FIGURE 3.6 Late stage ARDS (Image from Morton et al, 2005) TELEFLEX Academy Ventilation Workshop Pre-Reading Package TEST YOUR KNOWLEDGE Try to answer the questions below without initially referring to the chapter. The short answer questions should be completed in your own words. MATCHING EXERCISES A. Atelectasis 1. A pulmonary disease triggered by inhaled irritants, exercise, cold air, and viral infections that causes bronchospasm, which is usually reversible, and produces airway inflammation and increased airway responsiveness B. Chronic bronchitis 2. A pulmonary disease often caused by cigarette smoking or chronic infection during which mucus-secreting glands of the tracheobronchial tree become thickened and encroach on the diameter of the airway lumen C. Emphysema 3. A common postoperative pulmonary problem resulting from decline of volume or collapse of alveolar lung units that can lead to increased shunting of unoxygenated blood back to the left ventricle D. Asthma 4. An infection of the alveoli causing collapse of alveoli and impairment of oxygen diffusion E. Pneumonia 5. An irreversible pulmonary disease of the alveolus accompanied by destructive changes of alveolar walls with resultant loss of elastic recoil of the lung, resulting in over distension of alveoli TRUE/FALSE Please indicate whether the following statements are true or false. 1. Passive atelectasis can occur if communications between the alveoli and trachea are obstructed 2. Ventilation impairment can be caused by a loss of surface area or change in alveolar membrane and is assessed by low arterial oxygen levels 3. Hypoxia can be treated by increasing the surface area for gas exchange, decreasing excess alveolar fluid whilst supporting the patient organ function by supplementing their oxygen intake 4. Acute respiratory distress syndrome often occurs in patients with no previous lung disease TRUE / FALSE 28 | 29 SHORT ANSWER/FILL-IN QUESTIONS 1. Name four causes of atelectasis. a. b. c. d. 2. Describe how atelectasis impairs gas exchange. 3. List four common triggers of asthma a. b. c. d. 4. Describe how acute pulmonary oedema affects gas exchange. TELEFLEX Academy Ventilation Workshop Pre-Reading Package Glossary ACCESSORY MUSCLES OF VENTILATION Muscles other than the diaphragm or the internal and external intercostals, which are used in ventilation. Most visible are the sternocleidomastoid muscles on either side of the neck. The other accessory muscles are the scalenes. Activity of these muscles is assessed to determine a patient’s breathing effort. ACIDOSIS A pathologic condition resulting in the accumulation of acid or loss of base in the body. Respiratory acidosis is the state of excess retention of carbon dioxide. ACUTE Having severe symptoms and a short course. AEROPHAGIA The swallowing of air. AFFINITY An attraction or force between substances that causes them to interact or combine. AIR FLOW Air will flow from an area of higher pressure to one of lower pressure; during inspiration, the pressure in the alveoli must be less than the pressure at the mouth for air to flow in, and during expiration, the reverse is true. Air flow may be laminar, turbulent or transitional, depending on the velocity of flow and on the diameter and configuration of the tube. AIRWAY The anatomical structures through which air passes on its way to or from the alveoli; the nasopharynx and oropharynx, the larynx, the trachea, bronchi, and bronchioles. ALVEOLAR HYPOVENTILATION The inability to exchange sufficient amounts of air between the room and the lung to allow for gas exchange that produces normal concentrations of oxygen and carbon dioxide in the blood. Also referred to as ventilatory impairment. ALVEOLAR PRESSURE The pressure within the alveoli, conventionally given in cm H 20, with reference to an atmospheric pressure of zero. Thus, a negative alveolar pressure indicates that the pressure is lower than atmospheric; a positive alveolar pressure indicates that the pressure is above atmospheric. ALVEOLI The air sacs that act as the primary gas exchange units of the lung. APNOEA The cessation of ventilatory activity. Must persist for at least ten seconds. ARDS Acute Respiratory Distress Syndrome. Indicates respiratory failure with life threatening distress and hypoxaemia, associated with acute pulmonary injuries. 30 | 31 ATELECTASIS A shrunken and airless state of part or all of the lung; the disorder may be acute or chronic. ASTHMA A condition characterised by increased tone of the smooth muscle surrounding the bronchi and by bronchial inflammation and excess mucous secretion. An individual with acute asthma will present with an obstructive profile on respiratory function tests. ATMOSPHERIC PRESSURE Ambient air pressure averages 760 mm Hg at sea level. In pulmonary calculations, atmospheric pressure is taken as the reference value, 0 cm H 20. Pressures higher than atmospheric pressure then are positive; those lower than atmospheric pressure are negative. BLOOD GASES A term used to describe the assessment of arterial blood gas levels of oxygen (PaO2) and carbon dioxide (PaCO2). BRONCHITIS A clinical condition marked by airway inflammation and excess mucus secretion, manifested by cough and sputum production. It may cause narrowing of the airways and increase their resistance; this results in an obstructive ventilatory defect. CHEST WALL The anatomical structures that border the parietal pleura, including the ribs with intercostal muscles, and diaphragm; when the muscles of the chest wall are relaxed, the chest wall acts in an elastic fashion comparable to the lung, responding passively to the pressure differences around it. CHRONIC Persisting for a long time. COMPLIANCE Comprises the distensability, or “stretchability”, and elastance of the lung. Defined as the relationship between a given change in volume and the pressure required to achieve that change COMPLIANCE CURVE The pressure-volume curve for the lung or relaxed chest wall; plotting volume as a function of pressure inside minus pressure outside. The slope of this curve is the compliance. DEAD SPACE The portion of each breath that does not participate in gas exchange. Anatomic dead space is the volume of the conducting airways; physiologic dead space also includes the contribution of alveoli that are well-ventilated but poorly perfused. DIAPHRAGM A thin, dome-shaped sheet of muscle that inserts into the lower ribs; it is the most important muscle of inspiration – when it contracts, it lowers pleural pressure. DISTENDING PRESSURE The inside pressure minus the outside pressure of an elastic structure; for the lung, this is also referred to as the transpulmonary pressure or the recoil pressure of the lung. TELEFLEX Academy Ventilation Workshop Pre-Reading Package DYSPNEA Shortness of breath. ELASTANCE A component of lung compliance, it it’s the elastic recoil of the lungs after inspiration back to their original shape. Can be measured by alveolar pressure minus pleural pressure (Palv-Ppl). EMPHYSEMA A condition characterised by dilation and destruction of alveolar walls; it produces airflow obstruction as determined by pulmonary function testing. ERV Expiratory reserve volume. The difference between FRC and RV. This is the maximal amount of air that can be expired starting at FRC. ESOPHAGEAL BALLOON A thin walled balloon positioned in the lower oesophagus and attached to a strain gauge for estimating pleural pressure. F i O2 The fraction of inspired oxygen. Can be expressed as a decimal or a percent. Room air has an FiO2 of 0.21 or 21%. FORCED EXPIRATION The recording of a maximal expiration from Total Lung Capacity (TLC). This permits the measure of forced vital capacity (FVC) and various of air flow. FUNCTIONAL RESIDUAL CAPACITY Also known as FRC, this is the lung volume at the end of a normal expiration, when the muscles of respiration are completely relaxed FVC Forced vital capacity; the total volume of air that can be exhaled from the lungs during a forced expiration following a maximal inspiration. GAS DILUTION A method of ascertaining functional residual capacity (FRC) and residual volume (RV) by mixing the unknown volume of gas in the lungs with a known volume of gas containing a known concentration of a poorly soluble gas like helium. GLOTTIS The true vocal cords; when one closes the glottis, no air can escape from the lungs. HYSTERESIS The difference in the pressure-volume curves of the lung during inflation and deflation (the lung volume at any given pressure during deflation is larger than during inflation). HYPERCAPNIA An elevated level of carbon dioxide in the blood. PaCO2 typically over 45mmHg. 32 | 33 HYPERVENTILATION A situation where the patient’s breathe rate and/or tidal volume exceed their respiratory needs. PaCO2 is reduced below normal levels. HYPOXAEMIA A reduced level of oxygen in the blood. PaO2 is 55mmHg or below. IRV Inspiratory reserve volume; the difference between VC and FRC. This is the maximal amount of air that can be inspired starting at FRC. LAMINAR FLOW Air flow in the lungs which is streamlined, low velocity, and obeys Poiseuille’s Law; generally it is confined to the small peripheral airways. LAPLACE‘S LAW Equation expressing the relationship between the surface tension of a sphere and the resultant pressure: P=2T/r, where P=pressure, T=surface tension, and r=radius (for a soap bubble or sphere with two surfaces, P=4T/r). MINUTE VENTILATION The volume of gas that moves out of the lungs (expressed in litres per minute). It is calculated by multiplying the exhaled tidal volume by the respiratory rate. MUSCLES OF RESPIRATION During quiet inspiration: diaphragm and external intercostals. During active inspiration: the muscles of quiet inspiration plus the scalenes and sternomastoids. During quiet expiration: passive active expiration: abdominal muscles, internal intercostals. OBSTRUCTIVE DISEASE A respiratory abnormality characterised by delay in forced expiration of air from the lungs. Palv Alveolar pressure The pressure within the alveoli, conventionally given in cm H20, with reference to an atmospheric pressure of zero. Thus, a negative alveolar pressure indicates that the pressure is lower than atmospheric; a positive alveolar pressure indicates that the pressure is above atmospheric. Asthma, bronchitis, and emphysema are all considered obstructive conditions. PARIETAL PLEURA The portion of the pleural membrane that lines the thoracic cavity. PL Transpulmonary pressure The pressure difference across the lung. Alveolar pressure minus pleural pressure (Palv-Ppl), which is also known as the elastic recoil pressure of the lung. PLEURAL EFFUSION Collection of fluid within the pleural space. If the fluid is blood it may be referred to as a haemothorax, if there is a collection of pus it is referred to as a empyema. TELEFLEX Academy Ventilation Workshop Pre-Reading Package PLEURAL PRESSURE PPL The pressure within the pleural space. Its value is generally given with reference to an atmospheric pressure of zero, and it is measured in cm H 2O. Its symbol is Ppl. PLEURAL SPACE The tiny fluid-filled ‘space’ between the visceral and parietal pleura; if air should enter this normally noncommunicating space, a pneumothorax will result. PNEUMOTHORAX The presence of air in the pleural cavity, which may occur spontaneously, as a result of trauma, overinflation of the lungs, or a pathological process. POISEUILLE‘S LAW An equation which describes laminar flow in a straight tube. V=P¹r4/8nl, where V= flow P= driving pressure r= radius of tube n= fluid viscosity l= length of tube PULMONARY FIBROSIS A condition characterised by deposition of fibrous tissue in the lung. It decreases lung compliance and results in a restrictive ventilatory defect as seen on pulmonary function testing. RESISTANCE Refers to the opposition to gas flow through the airways. Affected predominantly by the diameter of the airways. RESPIRATORY FAILURE Occurs when there is an impairment in the exchange of gases between the circulating blood and the room air. Failure is seen when the PaO2 is reduced, but PaCO2 is normal, low or high. RESPIRATORY INSUFFICIENCY A broader class of respiratory impairment in which the patient is not capable of sustaining the work required to maintain ventilation for a prolonged period. RESTRICTIVE VENTILATORY DEFECT A condition characterised by a reduction in total lung capacity and vital capacity. Restrictive disorders may be caused by stiffening of the chest wall, stiffening of the lung itself, or by muscle weakness. RESIDUAL VOLUME Also known as RV, this is the volume of the lungs after a maximal expiration. SPIROMETRY A simple lung function test that measures lung volume as a function of time; it can be used to ascertain lung volumes or to gain information about maximal expiratory flow rates.. SURFACE TENSION The force of attraction between adjacent molecules of a liquid. SURFACTANT A phospholipid secreted by the Type II alveolar cells. It not only decreases surface tension, but decreases it most at low volumes and least at high volumes, contributing to the overall stability of the alveolar units. The lungs of neonates are often deficient in surfactant. 34 | 35 TIDAL VOLUME Also known as V T, this is the volume of an individual breath during quiet breathing. It averages about 500 ml. TOTAL LUNG CAPACITY Also known as TLC, this is the volume of the lungs after a maximal voluntary inspiration. TRANSITIONAL FLOW An intermediate type of airflow which has characteristics of both laminar flow and of turbulent flow. See Turbulent Flow. TRANSPULMONARY PRESSURE The pressure difference across the lung. Alveolar pressure minus pleural pressure (Palv-Ppl), which is also known as the elastic recoil pressure of the lung. TURBULENT FLOW Air flow characterised by disorganised movement of gas molecules and/or eddy formation; it occurs when there are high gas flow rates or the are irregularities in the lining of the airways. Turbulence can increase the pressure within the airways for a given volume of gas. VENTILATORY IMPAIRMENT The inability to exchange sufficient amounts of air between the room and the lung to allow for gas exchange that produces normal concentrations of oxygen and carbon dioxide in the blood. Also referred to as alveolar hypoventilation. VISCERAL PLEURA The portion of the pleural membrane that covers the lung. VITAL CAPACITY Also known as VC, this is the difference between Total Lung Capacity (TLC) and Residual Volume (RV); i.e., it is the maximum volume of air that can be exhaled starting at full lung inflation. TELEFLEX Academy Ventilation Workshop Pre-Reading Package References Antonelli, et al.(1998). A Comparison of Non-Invasive Positive-Pressure Ventilation and Conventional Mechanical Ventilation in Patients with Acute Respiratory Failure New England Journal of Medicine. 339:42935 Australian Institute of Health and Welfare (2001). Cancer in Australia, 2001[online] Available: http://www.aihw. gov.au/publications/index.cfm/title/10083 [Accessed 24th January, 2006] Ball, W.C. Jr (1996). Interactive Respiratory Physiology. [online] http://oac.med.jhmi.edu/res_phys/index.HTML [Accessed 17th January 2006] Bare, B.G. and O’Connell, S.C. (1992). Brunner & Suddarth’s Textbook of Medical-Surgical Nursing. (7th ed.). Philadelphia: Lippincott Bare, B.G. and O’Connell, S.C. (2004). Brunner & Suddarth’s Textbook of Medical-Surgical Nursing. (10th ed.). Philadelphia: Lippincott [online] Available: http://connection.lww.com/Products/smeltzer10e/frc.asp [Accessed 9th January 2006] Brochard, L. et al.(1995). Non-Invasive Ventilation for Acute Exacerbations of COPD. New England Journal of Medicine. 333:817-822. Burns, S.M. (1997). Understanding, applying and evaluating pressure modes of ventilation. American Association of Critical Nurse 7(4): 495- 506. Forrest, G. (1999) NSW College of Nursing. Critical Care Course Notes. Grossan, M. (2003). Sinus Disease & Problems explained. [online] Available: http://www.ent-consult.com/sinus_ lay.html [Accessed 10th January, 2006] Grossbach, I. (1986) Troubleshooting ventilator and patient related problems. Part 1. Critical Care Nurse. 6(4): 58-70. Hillberg, et al.(1997). Non- Invasive Ventilation. New England Journal of Medicine 337: 746-1752 Huskey, R.J. (1999) Introductory Biology. [online] Available from The University of Virginia, website: http:// www.biologie.uni-hamburg.de/b-online/library/bio201/bio201.html [Accessed 23rd January, 2006] Ingraham (P). The Respiration Connection: How the mechanics of respiration cause pain and upper body injuries. [online] Available from MindBodyGuide.ca website: http://mindbodyguide.ca/articles/respiration-connection. php [Accessed 7th November, 2005] Ingraham, P. (2004). The Respiration Connection: How the mechanics of respiration cause pain and upper body injuries [online] Available: http://mindbodyguide.ca/articles/respiration-connection.php [Accessed 7 November, 2005] King, M. (1996). Oncology for GPs: Lung cancer. [online] Available: http://www.quitnow.info.au/oncology.html [Accessed 24th January, 2006] 36 | 37 Kramer N. et al (1995). Randomized, prospective trial of non-invasive positive pressure ventilation in acute respiratory failure. American Journal Respiratory Critical Care Medicine 151: 1799-1806. Lin, M. et al. (1995). Reappraisal of CPAP therapy in acute pulmonary edema: short-term results and long-term follow up. Chest 107:1379-86. Marieb (2004). Human Anatomy & Physiology. (6th ed.). San Francisco: Benjamin Cummings [online] Available: http://academic.pgcc.edu/~aimholtz/AandP/ANPmain.html [Accessed 7th November, 2005] Mehta, S.. et al.(1997). Randomized, prospective trial of bi-level versus continuous positive airway pressure in acute pulmonary edema. Critical Care Medicine. 25:620-628. Moore, K.L. and Agur, A. (2003) Essential Clinical Anatomy (2nd ed.). Philadelphia: Lippincott [online] Available: http://connection.lww.com/products/moore/frc.asp [Accessed 9th January 2006] Morton, P.G.; Fontaine, D.K.; Hudak, C.M.; and Gallo, B.M. (2005). Critical Care Nursing: A Holistic Approach (8th ed.) Philadelphia: Lippincott [online] Available: http://connection.lww.com/Products/morton/frc.asp [Accessed 6th January 2006] Paulev, P. (2000). Textbook in Medical Physiology and Pathophysiology: Essentials and clinical problems. [online] Available: http://www.mfi.ku.dk/ppaulev/content.htm [Accessed 7th November, 2005] Pocanic, D. (2004) Physics of the Human Body [online] Available from The University of Virginia, Faculty of Physics website: http://www.people.virginia.edu/~dp5m/phys_304/pix.html [Accessed 6th July, 2005] Poponick, J. et al. (1999). Use of a Ventilatory Support System (BIPAP) for Acute Respiratory Failure in the Emergency Department. Chest 116:166-171 Porth, C.M. (2005). Pathophysiology: Concepts of Altered Health States. (7th ed.). Philadelphia: Lippincott [online] Available: http://connection.lww.com/Products/porth7e/frc.asp [Accessed 9th January 2006] Rappard, S. Use of CPAP and BiPAP in Acute Respiratory Failure. [online] Available: http://www.theberries. ns.ca/Archives/CPAP Stedman’s Medical Dictionary for the Health Professions and Nursing Illustrated (5th ed.). (2004). Philadelphia: Lippincott [online] Available: http://connection.lww.com/Products/stedmansmedict/frc.asp [Accessed 9th January 2006] Tamarkin, D.A. (2004) Anatomy and Physiology I & II [online] Available: http://distance.stcc.edu/AandP/ [Accessed 7th November, 2005] Taylor, L. and Stephens, D. (1990). Arterial blood gases: clinical application. Journal of Post Anaesthesia Nursing. 5(4): 264-272. U.S. National Cancer Institute’s Surveillance, Epidemiology and End Results (SEER). Introduction to the Respiratory System. [online] Available: http://training.seer.cancer.gov/module_anatomy/unit9_4_resp_ passages4_bronchi.html [Accessed 12th January, 2006] Whitfield, P., and D.M. Stoddard. (1984). Hearing, Taste, and Smell; Pathways of Perception. New York: Torstar Books, Inc. TELEFLEX Academy Ventilation Workshop Pre-Reading Package Woronczuk, J.; Medwid, S.; Neumann, L. and Eshelman, S. The Olfactory System: Anatomy and Physiology [online] Available http://www.macalester.edu/psychology/whathap/UBNRP/Smell/nasal.html [Accessed 10th January, 2006] TELEFLEX Academy Clinical Support and Education Team Level 4 Building B, 201 Coward Street, Mascot NSW 2020 Tel. +61 (0)409 533 759 e: [email protected] www.teleflex.com/academyaustralia TFXA-NIV-PREREADING - AP AU 01 ∙ REV B ∙MC/PDF ∙ 03 15 PDF