Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Coronary artery disease wikipedia , lookup
Myocardial infarction wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Ventricular fibrillation wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
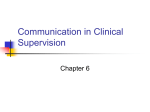
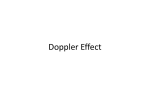
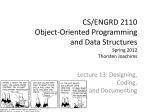
Objective and Subjective Analysis of Left Ventricular Angiograms By BERNARD R. CHAITMAN, M. D., HENRY DEMOTS, M. D., J. DAVID BRISTOW, M.D., JOSEF R6SCH, M.D., AND SHAHBUDIN H. RAHIMTOOLA, M. B., F. R. C. P. Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017 SUMMARY In order to determine the reproducibility of analyses of left ventriculograms, 35 cineangiograms were evaluated by four observers, two using standard quantitative techniques to determine ventricular volumes and a newly devised quantitative system to evaluate wall motion and two others using only visual inspection of the angiograms. Objective analysis repeated by the same observer correlated well for end-diastolic and end-systolic volumes and ejection fraction (r = .98, .99, .99, respectively) and only one of 105 (1%) wall segments were identified differently. Variability in assessments increased when comparisons were made with a second objective observer. Correlation coefficients for the three volumetric parameters were .93, .98, and .95 and there was disagreement in the assessment of 8% of wall segments. Wide variability was present between an objective and two subjective observers in analyses of end-diastolic volumes (r = .63, .64). Regional wall motion was assessed differently in 19% and 27% of segments, respectively. Though the correlation of objectively and subjectively determined ejection fractions was much better than the correlation for volume (r = .92, .84), it was not as good as the correlation between two objective observers. Occasional errors of clinical significance occurred. We conclude that subjective analysis has a significant error rate and that reproducibility and accuracy of analysis of left ventriculograms require objective analysis. made by two experienced observers; 4) the variability between assessments made by subjective and objective observers. Materials and Methods LEFT VENTRICULAR CINEANGIOGRAPHY is widely used to determine the nature and severity of cardiac disease and the effects of surgical and pharmacologic interventions on left ventricular function.' Quantitative methods for determination of ventricular volumes have been described and their accuracy validated previously.7 However, the determination of left ventricular function is frequently made by visual inspection of the cineangiogram rather than by application of objective quantitative techniques. This is especially true of assessments of regional wall motion because well established quantitative techniques are not available. In this study we have examined: 1) the reproducibility of analyses by objective techniques when employed by the same observer; 2) the variation in objective analyses performed by two different observers; 3) the variation of subjective evaluations Thirty-five left ventricular cineangiograms with good opacification, adequate centering of the image and without frequent extrasystoles were chosen for evaluation. There were 23 men and 12 women with a mean age of 47 years. Six patients had no demonstrable cardiac disease, one had an ostium secundum atrial septal defect, and the remaining 28 had significant coronary artery disease demonstrated by coronary arteriography. Uniplane left ventricular cineangiography was obtained in the right anterior oblique position at 60 frames/sec using 30 to 48 ml of meglumine diatrizoate. The injection rate varied from 10 to 15 ml/sec. Objective evaluation of left ventricular volumes, ejection fractions, and segmental wall movements were made by two observers who traced end-diastolic and end-systolic frames. The largest and subsequent smallest appearing ventricular silhouettes of a beat that did not represent or follow an extrasystole were used in each instance. Volumes for each silhouette were calculated by the area-length method.7 The extent of magnification which was determined by filming a lead impregnated ruler at the height of the apex of the heart varied from 1.38 to 1.66. Systolic wall motion was assessed using external and internal reference systems as described previously.8 A segment was called akinetic when the wall did not move during systole and dyskinetic when outward (paradoxical) movement occurred during systole. To assess hypokinesis a line representing the long axis of the ventricle was drawn from the midpoint of the aortic valve to the apex of both the end-diastolic and the end-systolic silhouettes. A perpendicular chord was drawn one-fourth of the way from the apex to the base of both silhouettes, thus dividing the From the Divison of Cardiology, Department of Medicine and the Department of Radiology, University of Oregon Health Sciences Center, Portland, Oregon. Supported in part by Program Project Grant HL 06336, Graduate Training Grant HL 05791 and Research Grant HL 16461 from the National Heart and Lung Institute. Dr. Chaitman is supported in part by the Canadian Heart Fund Fellowship Training Grant. Address for reprints: Henry DeMots, M.D., Division of Cardiology, University of Oregon Health Sciences Center, 3181 S. W. Sam Jackson Park Road, Portland, Oregon 97201. Received December 30, 1974; revision accepted for publication April 21, 1975. 420 Circulation, Volume 52, September 1975 ANALYZING LV ANGIOGRAMS 421 Table 1 Synopsis of Observations Compared Anterior Segment Long Axis\- Intraobserver variation Objective vs objective Interobserver variation Objective vs objective Subjective vs subjective Inter method variation Objective vs subjective - Apical Segment Inferior Segment Figure 1 The ventricle is divided along its long axis and a chord three-fourths of the distance from the base to the apex. The two apical areas are combined, thus defining three wall segments for evaluation. Observer 1 vs Observer 1 Observer 1 vs Observer 2 Observer Y vs Observer Z Observer 1 vs Observer Y Observer 1 vs Observer Z Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017 tensive experience in an environment which had allowed them to compare their subjective impressions with objective data. These two observers, working independently, estimated end-diastolic volumes and ejection fractions and graded the wall motion in each of the segments as normal, hypokinetic, akinetic, or dyskinetic. Magnification was judged by visual inspection of the framed ruler. Time for the evaluation was not restricted so that multiple viewings of each angiogram could be made. The reproducibility of objective techniques was evaluated by comparing the two objective assessments of Observer 1 and by comparing the assessment of Observer 1 with the assessment of Observer 2. The reproducibility of subjective techniques was determined by comparing the assessments of Observers Y and Z. Variability between the objective and subjective methods was determined by comparing the assessment of each of the subjective observers with the assessments of Observer 1 (table 1). ventricle into anterior, inferior and apical segments (fig. 1). The percentage decrease in area for the anterior, inferior and combined apical segments was then determined for each patient. This method of assessing hypokinesis does not require the actual superimposition of the ventricular silhouettes, but has the same effect as superimposing them along the long axis. The normal percentage decrease in area for each segment was established by determining the decrease in area for these segments in seven patients who had neither coronary artery disease nor hemodynamic evidence of left ventricular abnormality. In these patients, the decrease in area of the anterior segment was 48 ± 16% (mean ±1 SD), the apical segment 64 + 18%, and the inferior segment 40 ± 14%. Hypokinesis was diagnosed if neither akinesis or dyskinesis was present and if the percentage of systolic decrease in area was less than two standard deviations from normal. Observer 1 analyzed each angiogram twice at intervals ranging from one week to one year without knowing the frame or beat used previously. Observer 2 selected 21 of 35 angiograms at random and analyzed them without knowing the frame or beat analyzed by Observer 1. Both observers noted the frame numbers of each silhouette traced so that it could be determined whether significant variability could be introduced by tracing different beats. Subjective evaluation of all 35 angiograms was performed by two experienced observers (Observers Y and Z) with ex- Results Intraobserver Variation End-diastolic volume (EDV), end-systolic volume (ESV), and ejection fraction (EF) were highly reproducible when measured by the same observer. The mean variation (+SEM) for these three parameters was 4.8 ± .9 ml/m2, 4.7 + 1.4 ml/m2, and .021 ± .003 respectively (table 2). Wall motion was assessed identically on both occasions except that one (1%) of 105 .80 - r-.95 X .60 -- 'z .40 2 .20 80 120 LVEDV (mi/M2) OBS. 160 20 60 LVESV (m1/M2) OBS. l 100 y=.97x+3.95 Syx=4.49 . / N-21 * -. --Line of identity - .20 40 .60 80 EJECTION FRACTION OBS. I Figure 2 A good correlation is shown between two objective observers. There is an apparent systematic tendency for Observer 2 to estimate volumes lower than Observer 1. Circulation, Volume 52, September 1975 422 CHAITMAN ET AL. Table 2 Variation in Volumetric Assessments Difference of means Standard deviation Range 1.0 .9 .01 7.4 4.7 .02 -29 to +12 -20 to +7 -.07 to .03 4.8 4.7 .02 10.4 5.4 .02 9.4 4.4 .04 -39 to +3 -13 to +2 -.95 to +11 10.8 5.77 8.1 .03 27.1 .06 19.6 .01 27.1 .09 13 18 Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017 Obs 1 and Obs 1 EDV (ml/m2) ESV (ml/m2) EF Obs 1 and Obs 2 EDV (ml/m2) ESV (ml1m2) EF Obs 1 and Obs Y EDV (mi/M2) EF Obs 1 and Z EDV (ml /M2) EF Obs Y and Obs Z EDV (mi/rM2) EF .02 .08 Mean variance (4 SEM) - .9 1.4 .003 .039 - 1.9 .8 .005 -96 to +28 -.27 to +.08 21 .049 - 3.1 .008 -113 to +20 -.19 to +.27 24.2 .068 - - 3.9 .01 -63 to +18 -27 to +.15 14.7 .056 - 2.1 .005 - The difference of the means is the difference of the mean value for the compared groups. The standard deviation quantifies the scatter about these means. Mean variance is the average absolute difference between repeated determinations. segments judged normal on one determination judged hypokinetic on another (table 3). was Interobserver Variation Objective versus objective. The variation between the average of two determinations by Observer 1 and the single observation of Observer 2 was greater than intraobserver variation. The variation (mean ± SEM) for end-diastolic volume, end-systolic volume and ejection fraction was 10.8 + 1.9 ml/m2, 5.7 ± .8 ml/m2, and .039 ± .005, respectively (table 2). Figure 2 demonstrates that there was good correlation between the two sets of measurements (r = .93, .98, .95) and also suggests that most of the variation occurred because volumes determined by Observer 2 were systematically smaller than those determined by Observer 1. The variation when the same beat was chosen for analysis is 9.8 ± 1.4 ml/m2 and when different beats were chosen 11.4 ± 2.1 ml/m2. There was disagreement in the classification of wall motion for 5 (8%) of 63 segments examined (table 3). Subjective versus subjective. Interobserver variation for the two subjective observers for EDV and EF was 14.7 + 2.1 ml/m2 and .056 ± .005, respectively. The correlation was better for EF than EDV but varied more than data collected by the two objective observers (table 2). There was disagreement in the assessment of 25 (24%) of 105 wall segments (table 4). Variation of Subjective and Objective Methods Subjective assessment of left ventricular enddiastolic volume by Observers Y and Z varied considerably from the objective assessments made by Observer 1 (table 2). Correlation of volume deterable 3 Variation Between Objective Assessments of Wall Motion Ohserver 1 Normal Hypokinetic Akinetic Dyskinetic Normal Ohserver 2 Observer 1 Normal Hypokinetic 70 1 0 12 0 0 0 0 Observer 1 48 2 Hypokinetic 0 Akinetic 1 5 0 Dyskinetic 0 1 Akinetic 0 0 8 0 Dyskinetic 1 0 1 0 0 0 0 1 13 0 0 4 Italicized numbers denote instances of agreement and numbers not italicized instances of disagreement. For quantitation of error rate, akinesis and dyskinesis were considered the same. Circulation, Volume 52, September 1975 ANALYZING LV ANGIOGRAMS 423 Table 4 Variation Between Subjective Assessments of Wall Motion Observer Z Normal 53 2 0 1 Normal Hypokinetic Akinetic Dyskinetie Observer Y Hypokinetic 12 15 1 0 Akinetic 0 7 2 1 Dyskinetic 0 2 2 7 Dyskinetic 0 2 Akinetic 0 0 2 2 14 7 4 1 0 4 4 3 1 0 1 8 Table 5 Variation Between Objective and Subjective Assessments of Wall Motion Normal 62 Normal Observer Y Hypokinetic 2 Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017 Akinetic Dyskinetic Observer 1 Hypokinetic 9 10 2 0 a 0 0 9 Observer 1 Normal Observer Z 54 1 0 1 Hypokinetic Akinetic Dyskinetic minations was poor (r = .63, .64) but the correlation of objectively and subjectively determined ejection fractions was much better (r = .92, .84) (fig. 3). There was discrepancy from the objective evaluations in the assessments of regional wall motion in 19% and 27% of instances (table 5). Although assessments regarding wall motion and ejection fraction and wall motion abnormalities were correct in many instances (fig. 4), discrepancies of great clinical significance were occasionally made by one or both of the subjective observers. Figure 5 demonstrates an example where both subjective observers thought that the ejection fraction was markedly reduced and that there was abnormal wall motion. Objective assessments demonstrated that wall motion and ejection fraction were normal. Discussion Standard techniques for the determination of left ventricular volumes and ejection fraction have been 160 OBS. I = Measured OBS.Y= Visuol 236 ` k120 Cr .80)l _r =.92 y =.90x+2.51 . 60 - Syx=6.17 )~ N = 35 .40 )h X 80 * 0 )A iz .20 ) 80 120 - 160 line of identity .20 .40 .60 .80 EJECTION FRACTION OBS. LVEDV (mI/M2) OBS. Figure 3 The correlation between objective Observer 1 and subjective Observer Y was poor for volume determination but better for estimation of ejection fraction. All volumes greater than 105 ml/m2 were underestimated by subjective Observer Y. The results of correlating Observers 1 and Z are similar to those of Observers 1 and Y. Circulation, Volume 52, September 1975 CHAITMAN ET AL. 424 o-Externol Marker MW Coronory Arteriogram: L. Main 70% Stenosis RCA Occl EGG: Non-specific ST-T Abnormolities OBS. 2 OBS. I Wall Motion: I OBS. 2 Anterior Wall Apex Inferior Wall Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017 Ejection Fraction: 0.62 0.60 OBS. Y OBS. Z HK IHK HK 0.34 HK HK HK 0.42 Figure 4 Assessments of wall motion and ejection fraction were similar for all four observers in this example though one subjective observer underestimated the ejection fraction. titated the variability in the measurement of left ventricular function by subjective and objective methods by comparing the assessments of different observers examining the same angiogram. Repeated assessments by the same observer at widely variable intervals were highly reproducible. When the second measurement was performed by a different observer the variability increased slightly. This was especially true of absolute volumes and less developed and validated previously.7 Variation from day to day in these parameters has been shown and quantitated.9 The variation demonstrated may be attributed to biologic variation or to errors in measurement. This variability would be greater if angiographic studies were performed in close temporal proximity because angiographic contrast material is known to affect ventricular performance and intravascular volume.'0-13 This study has quan- 0 / TG Coronary Arteriogram: / LAD 80% Stenosis L-Cx 80% Stenosis RCA Occl K----- EGG: IMI OBS. I OBS. 2 Anterior Wall Apex Inferior Wall HK DK HK Ejection Fraction: 0.37 Wall Motion: I OBS. Y OBSR. 7 HK DK HK HK DK HK HK DK HK 0.37 0.28 0.40 -J Figure 5 A disparity of clinical significance between objective and subjective observers in the estimate of both ejection fraction and wall motion is demonstrated in this example. Circulation, Volume 52, September 1975 ANALYZING LV ANGIOGRAMS Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017 true of ejection fraction where systematic errors in end-diastolic and end-systolic volume measurements tend to cancel one another. No significant variability resulted from selection of different beats so the major source of variability arose from tracing of silhouettes. The extent of variation is much greater if subjective assessments are used instead of objective measurements. Subjective observers did well in judgments of ejection fraction although each made errors of judgment with definite clinical implications (fig. 5). The subjective observers did less well in the assessment of absolute ventricular volumes probably because this requires the viewer to integrate the visual image and the degree of magnification. The disagreement between the two subjective observers contrasts with the close agreement of the two objective observers and suggests that the difference between subjective and objective measurements is not systematic but rather due to random variability in the assessments of subjective observers. Akinesis, hypokinesis, and dyskinesis are easily defined in qualitative terms but several problems become apparent in clinical application. Various reference systems have been proposed for the crucial step of superimposition of end-diastolic and endsystolic silhouettes.8' 14, 15 It is obvious that the choice of technique for superimposition will influence the determination of segmental wall motion. It is also apparent that the designation of hypokinesis is frequently arbitrary when it is defined only in qualitative terms. Although designations of segment borderlines in our study are arbitrary and more satisfactory systems may be devised, our results demonstrate that subjective evaluation of wall motion is highly variable and that reproducibility in the assessment of wall motion is facilitated by using objective techniques. Precise determinations of the effects of surgical or pharmacologic interventions on wall motion require quantitative analysis and a clear statement regarding the method of superimpositon of silhouettes and quantitation of segmental wall motion. Each observer must be aware of his or her own limitations in the assessment of left ventricular cineangiograms whether objective or subjective techniques are used. Error rates in the assessment of left ventricular function vary from one individual to Circulation, Volume 52, September 1975 425 another but our study demonstrates that error will be minimized if objective techniques are used. References 1. CHATTERJEE K, SWAN HJC, PARMLEY WW, SUSTAITA H, MARCUS HS, MATLOFF J: Influence of direct myocardial revascularization on left ventricular asynergy and function in patients with coronary heart disease: with and without previous myocardial infarction. Circulation 47: 276, 1973 2. REES G, BRISTOW JD, KREMKAU EL, GREEN GS, HERR RH, GRISWOLD HE, STARR A: Influence of aortocoronary bypass surgery on left ventricular performance. N Engl J Med 284: 1116, 1971 3. GRIFFITH LSC, ACHUFF SC, CONTI CR, HUMPHRIES JO, BRAWLEY RK, GOTT VL, Ross RS: Changes in intrinsic coronary circulation and segmental ventricular motion after saphenous vein coronary bypass graft surgery. N Engl J Med 288: 589, 1973 4. MCANULTY JH, HATTENHAUER MT, ROSCH J, KLOSTER FE, RAHIMTOOLA SH: Improvement in left ventricular wall motion following nitroglycerin. Circulation 51: 140, 1975 5. BONCHEK LI, RAHIMTOOLA SH, CHAITMAN BR, ROSCH J, ANDERSON RP, STARR A: Vein graft occlusion: Immediate and late consequences and therapeutic implications. Circulation 50 (suppl II): 11-84, 1974 6. RAHIMTOOLA SH, EHSANI A, LOEB HS, ROSEN KM, GUNNAR RM: Left ventricular function in the convalescent phase of acute myocardial infarction. Chest 66: 333, 1974 7. SANDLER H, DODGE HT: The use of single plane angiocardiograms for the calculation of left ventricular volume in man. Am Heart J 75: 325, 1968 8. CHAITMAN BR, BRISTOW JD, RAHIMTOOLA SH: Left ventricular wall motion assessed by using fixed external reference systems. Circulation 48: 1043, 1973 9. MCANULTY JH, KREMKAU EL, ROSCH J, HATTENHAUER MT, RAHIMTOOLA SH: Spontaneous changes in left ventricular function between sequential studies. Am J Cardiol 34: 23, 1974 10. BROWN R, RAHIMTOOLA SH, DAvIs GD, SWAN HJC: The effects of angiocardiographic contrast medium on circulatory dynamics in man: Cardiac output during angiocardiography. Circulation 31: 234, 1964 11. RAHIMTOOLA SH, DUFFY JP, SWAN HJC: Ventricular performance after angiocardiography. Circulation 35: 70, 1967 12. RAHIMTOOLA SH, GAU GT, RAPHAEL MJ: Cardiac performance after diagnostic coronary arteriography. Circulation 41: 537, 1970 13. KLOSTER FE, BRISTOW JD, PORTER GA, JUDKINS MP, GRISWOLD HE: Comparative hemodynamic effects of equiosmolar injections of angiographic contrast materials. Invest Radiol 2: 353, 1967 14. HERMAN MV, HEINLE RA, KLEIN MD, GORLIN R: Localized disorders in myocardial contraction. N Engl J Med 277: 222, 1967 15. McDONALD IG: The shape and movements of the human left ventricle during systole. Am J Cardiol 26: 221, 1970 Objective and subjective analysis of left ventricular angiograms. B R Chaitman, H DeMots, J D Bristow, J Rösch and S H Rahimtoola Circulation. 1975;52:420-425 doi: 10.1161/01.CIR.52.3.420 Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017 Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1975 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7322. Online ISSN: 1524-4539 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circ.ahajournals.org/content/52/3/420 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation is online at: http://circ.ahajournals.org//subscriptions/