Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
HYPERTROPHY & ENLARGEMENT
OF HEART CHAMBERS
Podcheko Alexey, MD
Upd Fall 2014
1
Intended Learning Outcomes
To know ECG criteria for :
1. “Left Ventricular Hypertrophy”
2. “Right Ventricular Hypertrophy”
3. “Right and Left Atrial Enlargement”
2
Precordial leads V1-V6 (horizontal plane)
V1-V2 Right
ventricle
V3 Septum
V4-V6 Left
Ventricle
Why should I know signs of LVH and
RVH?
LVH and RVH frequently misdiagnosed as acute
Myocardial Infarct and as result patient may
incorrectly treated
“Left Ventricular Hypertrophy”
“Left ventricular depolarization” is responsible for the
prominent R waves in the left sided chest leads and the S
waves of the right sided chest leads.
5
“Left Ventricular Hypertrophy”
The Voltage developed by
depolarizing cardiac muscle
is proportional to the Mass
of muscle present
During hypertrophy as the
left ventricular muscle mass
increases, greater
depolarization voltages are
produced in the thickened
ventricular wall
The amplitude of the R wave
in the left lateral leads
becomes progressively
higher while the S waves in
the right sided chest leads
become progressively
deeper.
Criteria to diagnose left
ventricular hypertrophy
“Voltage Criteria”, the best known of which is the
“Sokolow-Lyon criterium”:
If the sum of the depth of the S wave in lead
V1 and the height of the R wave in lead V5 or
V6, which ever is the taller, is greater than 35
mm (35 small squares) the patient has left
ventricular hypertrophy
7
Sokolow-Lyon criterium
If a subject meets the Sokolow-Lyon Criterion on their
ECG they have a high probability of underlying LVH.
o However, a high proportion of individuals with
underlying LVH do NOT meet the criterium on their
ECG.
o This pattern of high specificity but low sensitivity, is
observed with almost all voltage criteria and probably
reflects the fact that factors other than muscle mass
influence the amplitude of deflections in the leads.
9
Sokolow-Lyon criterium, exceptions
In obese individuals the increased
distance of the leads from the heart tends
to dampen down the amplitude of
deflections produced
If the voltage criteria are present on the
ECG this is strong evidence of underlying
LVH; however, if they are not, this does not
reliably outrule hypertrophy.
10
LVH and changes in the ST segments
and T waves
LVH can produce striking changes in
the ST segments and T waves on the
ECG, with T wave inversion and ST
segment depression in the “left” sided
leads.
ST elevation may be present in the
“right” sided chest leads. In the
setting of LVH, these T wave and ST
segment changes are referred to as an
“LV strain pattern”.
The ‘LV strain pattern’ [Chronic] is seen
on the ECG of a proportion of LVH
cases.
It is clinically important as it is easily
confused with the ECG changes of
11 acute coronary artery thrombosis
LVH and changes in the ST segments
and T waves
ST elevation may be present in the “right” sided
chest leads. In the setting of LVH, these T wave
and ST segment changes are referred to as an “LV
strain pattern”.
LV strain pattern and LVH
LV strain pattern may result from reversal of the normal transmural
dispersion of repolarization in the thickened ventricular wall with
consequent loss of T wave /QRS concordance.
The ECG changes of ‘LV strain’ are chronic and do Not
reflect underlying acute ischemia.
Most common causes of LVH: HTN, Athletic Heart, AS,
Coarctation of Aorta
13
Summary: EKG Voltage Criteria for
LVH
1. Height of R-wave in V5 or V6 + Depth of S-wave in V1 > 35
mm (35 small sq. or 7 Large Squares)
(or)
R-wave in V5 or V6 > 27 mm
(or)
R-wave in aVL > 11 mm
(and)
2. LV Strain Pattern: ST segment Depression & Asymmetrical
T-wave Inversion in “Left”-sided Leads, such as Leads I, aVL,
V5, & V6;
3. ST segment elevation may be present in the “Right”-sided
Leads
4. Heart Axis – Horizontal
Remember: in LVH Heart Axis is
horizontal, but there is no LAD!!!
-30°
0°
+60°
ECG Criteria for Right Ventricular
Hypertrophy
In the presence of gross RVH, when the RV wall has
increased to at least twice its normal thickness, the
depolarizing voltage generated in the enlarged right
ventricular muscle mass can produce:
a. abnormally tall R waves in the “right” sided chest leads
(V1)
b. persistent large S waves in those on the “left” (V6).
V1
V6
16
“EKG Voltage Criteria
for RVH”:
An R wave in lead V1
higher than 7 small squares
in amplitude
(or)
If the R wave in lead V1 is
higher in amplitude than the
S wave (R:S ratio > 1)
(or)
R wave in lead V1 + S
wave in lead V6 > 11 mm
Criteria for RVH
Some cases of RVH may be associated with an “RV
strain pattern” on the ECG with ST depression and
asymmetrical deep T wave inversion in leads V1 to V3.
In this situation, this does NOT reflect underlying acute
ischemia.
Sensitivity of the ECG in the diagnosis of RVH is poor:
20%
(RVH) primarily “Cor Pulmonale” – Pulmonary HTN, COPD, Emphysema,
PS, etc.
18
SUMMARY: ECG SIGNS OF RVH
19
20
Right and Left Atrial Enlargement
Characteristics of the Normal Sinus P Wave:
•Smooth contour
•Monophasic in lead II
•Biphasic in V1
Axis
•Normal P wave axis is between
0° and +75°
•P waves should be upright in
leads I and II, inverted in aVR
Duration
< 120 ms
Amplitude
< 2.5 mm in the limb leads,
< 1.5 mm in the precordial leads
Atrial abnormalities are most easily seen in the inferior
leads (II, III and aVF) and lead V1, as the P waves are most
prominent in these leads.
The Atrial Waveform – Relationship to
the P wave
Atrial depolarisation proceeds sequentially
from right to left, with the right atrium
activated before the left atrium.
The right and left atrial waveforms summate
to form the P wave.
The first 1/3 of the P wave corresponds to
right atrial activation, the final 1/3
corresponds to left atrial activation; the
middle 1/3 is a combination of the two.
In most leads (e.g. lead II), the right and left
atrial waveforms move in the same direction,
forming a monophasic P wave.
However, in lead V1 the right and left atrial
waveforms move in opposite directions. This
produces a biphasic P wave
Right Atrial Enlargement – Look at the
Lead II
In right atrial enlargement, right atrial
depolarisation lasts longer than normal
and its waveform extends to the end of
left atrial depolarisation.
Although the amplitude of the right
atrial depolarisation current remains
unchanged, its peak now falls on top of
that of the left atrial depolarisation
wave.
The combination of these two
waveforms produces a P waves that is
taller than normal (> 2.5 mm), although
the width remains unchanged (< 120 ms,
3 s sq).
Right Atrial Enlargement – Lead V1
Right atrial enlargement causes increased height (>
1.5mm) in V1 of the initial positive deflection of the
P wave.
“Right Atrial Enlargement”:
P waves in any inferior lead taller than 2.5 mm or
small squares
(Sensitivity 7%, Specificity 100%)
Initial positive deflection of P waves > 1.5mm in V1
Causes of RA Enlargement:
“P. Pulmonale” – Chronic lung diseases (cor pulmonale),
Pulmonary HTN,Tricuspid valve stenosis,Tricuspid valve
regurgitation,etc.
25
Left Atrial Enlargement – Lead II
In left atrial enlargement, left
atrial depolarisation lasts longer
than normal but its amplitude
remains unchanged.
Therefore, the height of the
resultant P wave remains within
normal limits but its duration is
longer than 120 ms (>3 s. sq.)
A notch (broken line) near its
peak may or may not be present
(“P mitrale”).
Left Atrial Enlargement – Lead V1
Left atrial enlargement causes widening (> 40ms wide, 1
s sq) and deepening (> 1mm deep) in V1 of the terminal
negative portion of the P wave.
“Summary: Left Atrial Enlargement”:
P waves in “any” lead broader than 2.5 small squares in
“duration”.
{Sensitivity 84%, Specificity 35%}
Negative P terminal force in lead V1 greater than 1 small square
in “Depth” and “Duration”.
(Sensitivity 37%, Specificity 88%)
Notched P waves with peak separation of greater than 1 small
square (“P. Mitrale”).
(Sensitivity 8%, Specificity 99%)…………..
28
Causes of Left Atriam Enlargement:
“P. Mitrale” – Mitral Stenosis, Mitral Regurgitation,
Remember, when applying “voltage criteria” for
chamber enlargement always check that the
calibration box is two large squares in height
and one large square in
width………………….indicating the machine is
recording at a needle speed of 25 mm/sec.
29
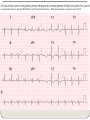
Biatrial Enlargement
Biatrial
enlargement is
diagnosed when
criteria for both
right and left atrial
enlargement are
present on the
same ECG.
Review of Cases