Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Heart failure wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Echocardiography wikipedia , lookup
Myocardial infarction wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Electrocardiography wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Ventricular fibrillation wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
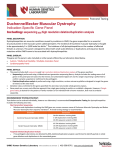
CONTRACTION AND RELAXATION OF LV WALL/Goldberg et al. hypertensive subjects. Circulation 59: 623, 1979 12. Henry WL, Bonow RO, Borer JS, Ware JH, Kent KM, Redwood DR, McIntosh CL, Morrow AG, Epstein SE: Observations on the optimum time for operative intervention for aortic regurgitation. I. Evaluation of aortic valve replacement in symptomatic patients. Circulation 61: 471, 1980 13. Henry WL, Bonow RO, Rosing DR, Epstein SE: Observations 1061 on the optimum time for operative intervention for aortic regurgitation I I. Serial echocardiographic evaluation of asymptomatic patients. Circulation 61: 484, 1980 14. Henry WL, Bonow RO, Borer JS, Kent KM, Ware JH, Redwood DR, Itscoitz SB, McIntosh CL, Morrow AG, Epstein SE: Evaluation of aortic valve replacement in patients with valvular aortic stenosis. Circulation 61: 814, 1980 Echocardiographic Determination of Contraction and Relaxation Measurements of the Left Ventricular Wall in Normal Subjects and Patients with Muscular Dystrophy Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017 STANLEY J. GOLDBERG, M.D., LINDA FELDMAN, CYNTHIA REINECKE, LAWRENCE Z. STERN, M.D., DAVID J. SAHN, M.D., AND HUGH D. ALLEN, M.D. SUMMARY Boys with Duchenne's muscular dystrophy (DMD) usually have a cardiomyopathy characterized by fibrosis of the epicardial half of the left ventricle. This cardiomyopathy is difficult to detect by noninvasive techniques. We report a technique that evaluates incremental left ventricular posterior wall thickening and thinning. High-quality left ventricular posterior wall echoes in 24 boys with DMD and 32 controls were recorded at chordal level two times 1 year apart. Endocardial and epicardial echoes and a timing ECG were digitized and analyzed by minicomputer. Left ventricular wall amplitudes were determined at standardized temporal increments during contraction and relaxation. To compare with this left ventricular assessment technique, systolic ejection times, shortening fraction and mean velocity of circumferential fiber shortening (Vcf) were also computed in the standard way. Mean year-to-year changes were minor. Mean Vcf, the ratio of preejection period to left ventricular ejection time and shortening fraction during the first year were statistically similar to those of the controls. Shortening fraction decreased slightly during the second year and became significantly different from the control, but remained within the normal range. Left ventricular wall thickness and cavity size were significantly less in boys with DMD than in controls. Therefore, we had to normalize incremental wall thickness to determine if any significant difference occurred. To do this, we evaluated the percentage of maximal wall thickness which occurred at a given percent of systole and diastole. Using this technique, it was shown that thickening during systole was a nearly linear process with respect to time in both groups. However, relaxation was significantly different between the groups. Relaxation was found to be an alinear process, and most thinning occurred in the first 40% of diastole. The major finding of this investigation was that the left ventricular wall of boys with DMD thinned at a slower rate than that of normal subjects. This new technique appears to be sensitive and demonstrates subtle changes in the left ventricular posterior wall. THE CARDIAC PATHOLOGY of Duchenne's muscular dystrophy (DMD) has been described in only a few patients. Detailed gross and microscopic analyses of 15 hearts of affected boys showed that left ventricular fibrosis and/or dilation was present in 94%.1` The results (table 1) indicate that left ventricular fibrosis was usually localized to the epicardial half of the left ventricular free wall and usually occurred in a diffuse distribution. In 27%, fibrotic changes were localized to the posterior basal area of the heart. The fibrosis is not similar to that observed in From the Departments of Pediatrics and Neurology, University of Arizona Health Sciences Center, Tucson, Arizona. Address for correspondence: Stanley J. Goldberg, M.D., Department of Pediatrics (Cardiology), University of Arizona Health Sciences Center, Tucson, Arizona 85724. Received November 8, 1979; revision accepted April 4, 1980. Circulation 62, No. 5, 1980. myocardial infarction, for in DMD, normal muscle cells are intermixed with fibrotic areas. Although death in some patients with DMD results from congestive cardiac failure, frank cardiac decompensation is a relatively uncommon feature in the early or middle stage of the disease.5 However, electrocardiographic evidence of cardiac abnormality is frequently found in children younger than 5 years of age.6 Thus, DMD provides a model of mild cardiomyopathy that progresses to a more severe form in the second decade.7 8 The purpose of our investigation was to develop a method for evaluating the cardiomyopathy found in DMD patients. Previous investigations have shown that conventional echocardiographic measurements of myocardial function, such as velocity of circumferential fiber shortening (Vcf), shortening fraction, ejection fraction and stroke index, have been normal or ClIRCULATION 1062 TABLE 1. Combined Data from Examination of Gross Specimensl-'-Duchenne's Mluscular Dystrophy Pathology. (15 reported cases) Heart size Increased 47 Normal 33( /o Unstated 20%/o Fibrosis Epicardial-half generalized Posterobasal Type unspecified None 47% 27%, 20c ' 6%,6 Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017 Other areas (1 each) Septal Right ventricle Papillary Coronary only slightly decreased in DMD.8 9 Most of these global measurements of myocardial function evaluated cyclic changes in left ventricular dimension or time intervals,8 9 hut did not directly evaluate the involved portion of the heart, the left ventricular posterior wall. Kovick and co-workers'0 evaluated the left ventricular wall and determined that DMD patients have abnormalities of systolic and diastolic velocity. They determined this by drawing a tangent to the endocardial surfaces and measuring the slope of that tangent to determine velocity. Although their observation was important, the measurement did not take into account the fact that varying degrees of epipericardial separation might influence this measurement or the problems of tangent construction. Ahmad and co-workers9 repeated the study of Kovick et al.'0 and failed to confirm the systolic change, and concluded that the reduced maximal diastoli-c endocardial velocity may reflect overall movement of the heart within the thorax rather than a functional cardiac abnormality.9 In this investigation, we report a method that separates total cardiac motion from changes in wall thickness that occur in systole and diastole. Our results demonstrate that the left ventricular posterior wall (LVPW) in DMD fails to thin rapidly during early diastole. Methods The study group included 24 boys with DMD, ages 2-24 years, followed in our DMD clinic, who had varying degrees of progressive muscular dystrophy. To a maximal extent, all other neurologic diagnoses had been ruled out. Confirmatory information for the presence of DMD consisted of family history, muscle biopsy, elevated creatine phosphokinase and an abnormal ECG.6 All had muscular weakness and in most instances the weakness was severe. All had been followed serially with muscle-testing analysis. VOL 62, No 5, NOVEMBER 1980 The control group consisted of normal subjects in the same age range as the DMD boys. None was known to have neuromuscular or cardiac disease. These boys were unrelated friends of the families or other randomly selected volunteers. For boys with DMD and controls, height, weight and blood pressure were obtained. For those with DMD only, an ECG was obtained if one had not been previously performed in the Duchenne's clinic. A standard echocardiogram was obtained for each participant and this was repeated 1 year later. Equipment for echocardiography consisted of a Smith Kline 20A echograph modified to have increased receiver gain by altering the receiver card circuitry. A switched-gain circuit was installed after the description of Griffith and Henry.'1 Recording was accomplished on a Honeywell 1856 recorder at a recording speed of 50 or 100 cm/sec. Time mark accuracy was verified with a stopwatch. A chest wall equivalent of electrocardiographic lead II was recorded for timing reference. If the QRS was isoelectric in this lead, another lead was selected. A variety of ultrasonic transducers, ranging in frequency from 2.25-5 MHz with crystal sizes of 6-12 mm, was used. After a standard echocardiogram was recorded, the LVPW was reexamined at the level of the chordae, and the posterior left ventricular wall image was then electronically expanded so that the septum was at the top of the oscilloscope screen and the LVPW was at the bottom. The objective was to enlarge the left ventricular posterior wall to improve tracing accuracy (fig. IA). An acceptable wall was defined as one in which the plane of the beam was appropriate and the endocardial and epicardial surfaces were seen as continuous. We also required that the epicardium was imaged separately from the pericardium. After each tracing was obtained, it was assigned a random six-number sequence to eliminate any future analysis bias. Standard Measurements The left ventricular internal dimension (LVID) and LVPW were measured according to suggested criteria in end-systole (s) and end-diastole (d)."1 All measurements were made from leading edge to leading edge. Left ventricular ejection time (LVET) for the mean Vcf calculation was obtained from aortic valve tracings recorded at R-R intervals matched to those of the ventricular dimensions under analysis. Vcf was computed as: LVID(d)-LVID(s)/LVID(d) X LVET. 13 Shortening fraction was computed as LVID(d)-LVID(s)/LVID(d).'4 Left ventricular systolic time ratio was computed as: Preejection period (PEP)/LVET. PEP was measured as the time from the first inscription of the QRS to the first opening motion of the aortic valve. LVET was measured as the time from the initial opening of the aortic valve until aortic leaflet recoaptation."1 Computer Analysis of LVPW Wall Tracing The endocardium and epicardium of the expanded LVPW were manually traced with an ultrasonic CONTRACTION AND RELAXATION OF LV WALL/Goldberg et al. 1063 FIGUREE 1. (A) An expanded section of left ventricular pos terior wall (L VPW). The septum is partially visible at the top of the panel and the endocardium and pericardium are clearly visible, particularly in the left complex. Pieces of chordae are noted. (B) An example of a wall thickness plot for one beat. The QRS initial deflection is at the origin and end of the trace. Numbers on the x-axis refer to a given percent of contraction or relaxation. :.LVPW Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017 ME, 25 75 100 1020 40 CONTRACTION AT RELAXATION AT % TIME % TIME TIME TO TIME TO No CONTRACTION S% RELAXATION digitizing pen interfaced to a Wang 600 computer. The onset of the QRS was digitized for each complex to act as a time marker. The program accepted only epicardial measurements that occurred at exactly the same time as the previously digitized endocardial points. One hundred twenty-eight points were allocated for each cardiac cycle. Wall thickness was determined by subtracting endocardial from epicardial distance between each pair of points. Then an X-Y plotter drew a reconstruction of the original wall as a check and a continuous LVPW thickness from subtraction data. The computer then subdivided the X axis first into systolic and diastolic time, and then into quartiles and deciles for each phase (fig. IB). At the quartiles and deciles of time, the Y value, wall thickness, was automatically determined. The standardized beginning of systole was the initial deflection of the QRS complex. End-systole was defined from the wall thickness graph as the peak of wall thickness. This was initially verified experimentally by comparing the time between the onset of the QRS and aortic coaptation and the time from the QRS onset to the peak of wall thickness. The times were found to be identical in 12 subjects - five normals and seven with DMD, and thereafter the wall graph alone was used for identification of end-systole. Repeatability for Wall Trace Evaluation Repeatability was tested by: (1) having different individuals trace the same complex of the same tracing; (2) comparing the values of traces of different complexes of the same record; (3) comparing values of tracings of the same individual recorded on different days; and (4) comparing values of all participants obtained from tracings one year apart. Two-dimensional Evaluation To rule out the possibility that we might have selected an isolated affected segment of the wall for evaluation that differed from the rest of the ventricle, we performed two-dimensional echocardiography to observe for akinetic or dyskinetic segments. Examination was performed with a Toshiba SSH lOA phasedarray or an electronically focused, high-resolution prototype 3-MHz scanner. The left ventricle was evaluated in three planes: long axis, short axis and apical.'6' 17 The short axis was evaluated at the level of 1064 CIRCULATION the anterior mitral valve leaflet, the area in which both leaflets were visible, the chordal level and the papillary level. The long axis was then evaluated from the standard precordial position and from the four-chamber apical position. The transducer was rotated to progressively evaluate as much myocardial wall as possible. Images were reviewed after the method of Rogers et al. to observe for akinesis or dyskinesis.'8 Data Handling Data were dealt with exclusively by the six-digit numbers. The code was broken only after the computer formed the groups and analyzed the data. Statistics For reproducibility, analysis of variance techniques or paired t ratio was used as applicable, depending upon the number of groups and group size. For comDownloaded from http://circ.ahajournals.org/ by guest on June 14, 2017 parison of controls and DMD patients, unpaired t ratio was used. A linear correlation technique was used to compare variables for the two groups. Results Two sets of data, separated by 1 year, were obtained for 26 boys with DMD and 32 controls. Two DMD traces were excluded because of inadequate record quality, leaving 24 adequate pairs of records. Anthropometric Data Although ages of the patients and their controls statistically similar, normal subjects were a mean of 1 1 kg heavier and 15 cm taller than DMD patients. The height of many DMD patients was inaccurate because of severe skeletal deformities, usually kyphoscoliosis. In many patients, we used length from heel to head measured while the boy was lying down. Mean calculated body surface area was 0.48 m2 smaller in boys with DMD, but this number is probably falsely low because of the kyphoscoliosis. were VOL 62, No 5, NOVEMBER 1980 Vital Signs Heart rate was significantly faster in DMD than in controls (p < 0.05), but no significant year-to-year variability occurred in either group (table 2). Blood pressure was statistically similar for both groups. Vcf The Vcf was statistically similar for controls and DMD patients (table 2). Statistical similarity remained after Vcf was corrected for heart rate after the data of Hirschleiter et al.19 Ratio of PEP/LVET The ratio was statistically similar for controls and DMD patients (table 2). Shortening Fraction Comparison of controls and DMD boys indicated that mean shortening fraction was similar in year 1, but was slightly but significantly lower (p < 0.05) in year 2 for DMD patients compared with year 2 controls (table 2). However, the mean of both groups fell within the previously described normal range. 14 Cavity Size LVID in systole and diastole was less in boys with DMD than in controls (p < 0.05) (table 3). Although the decrement might appear greater than could be accounted for on the basis of body size differences,20 such a comparison is unwarranted, for the body surface area in these DMD boys is more speculative than known, because accurate heights were not obtainable. Wall Thickness During the Cardiac Cycle The thickness of the wall was measured in milli- meters at 25%, 50%, 75% and 100% of systolic time, and 10%, 20%, 40% and 100% of diastolic time (table 4). Systolic divisions were initially selected arbitrarily TABLE 2. Comparison of Velocity of Circumnferential Fiber Shortening, Preejection Period/Left Ventricular Ejection Time, Shortening Fraction, and Heart Rate for Normal Subjects and for Duchenne's Muscular Dystrophy Patients for Years 1 and 2 Control year Control year DMD year DMD year 1 1 2 2 (n= 32) (n= 24) (n= 32) (n= 24) Significance Vcf 1.6 0.34 1.5 0.33 1.6 0.35 1.5 0.42 0.29 0.09 0.28 0.09 0.29 0.08 0.30 0.07 PEP/LVET 0.35 0.04 0.35 0.04 0.33 0.07 0.31 0.06 a Shortening fraction 81.1 Heart rate 14.8 78.3 14.3 101.9 13.0 104.3 12.0 a, b Values are mean * SD. Differences between the means for controls year 1 and year 2 and differences between the means for DMD patients year 1 and year 2 were not significant. a = p < 0.05 between the means for controls year 2 and DMD patients year 2. b = p < 0.05 between the means for controls year 1 and DMD patients year 1. Abbreviations: Vcf = velocity of circumferential fiber shortening; PEP/LVET = ratio of preejection period to left ventricular ejection time; DMD = Duchenne's muscular dystrophy. CONTRACTION AND RELAXATION OF LV WALL/Goldberg et al. 1065 TABLE 3. Comparison of Means for Raw Standard Echocardiographic Measurements of Controls and Duchenne's Muscular Dystrophy Patients Control year 1 (n 32) Control year 2 (n= 32) DM1) year 1 (n 24) DMD year 2 (n= 24) Significance LVIDd 42.6 5.3 43.8 6.0 36.2 3.8 37.3 3.0 a, b LVIDs 27.7 4.2 28.6 4.3 24.2 4.1 26.0 4.0 a, b LVPWd 6.1 1.2 6.3 i 1.1 4.8 1.3 5.0 1.3 a, b LVPWs 11.9 2.1 12.0 1.8 8.7 2.0 9.0 + 1.8 a, b Values are mean - SD. Differences between the means for controls year 1 and year 2 and differences between the means for DMD patients year 1 and year 2 were not significant. a = p < 0.05 between the means for controls year 1 and DMD patients year 1. b = p < 0.05 between the means for controls year 2 and 1)MD patients year 2. Abbreviations: LVIDd = left ventricular internal dimension at end-diastole; LVIDs = left ventricular internal dimension at end-systole; LVPWd = left venitricular wall thickness at end-diastole; LVPWs = left ventricular posterior wall thickness at end-systole; l)MI) = Duchenne's muscular dystrophy. Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017 and retained when it became apparent that systolic thickening progressed linearly. As diastolic thinning occurs rapidly, diastolic divisions were selected to track this event. The 100% diastolic measurement is identical to conventional LVPW thickness at enddiastole, and 100% systolic thickness is identical to conventional maximal thickness of the left ventricular wall. These data demonstrated that during the 1-year interval between examinations, the wall, for each time interval, increased in end-diastolic measurement for both groups 1-10%. This increase was almost certainly due to growth and in several timed measurements the change was significant at the p < 0.05 level. However, wall thicknesses at any time interval were significantly less (p < 0.05) for boys with DMD than for normals (fig. 2, table 4). In boys with DMD, end-diastolic thickness increased 82% and in normal subjects it increased 92%. The difference between the two groups, for this measurement, was not statistically significant. The absolute thicknesses of the two groups were different, so we had to evaluate the percent thickening during systole and percent thinning during diastole at a percent of systolic or diastolic time. When this was done, the contraction was a nearly linear process for both groups. In year 1, boys with DMD demonstrated 26% thickening at 25% time, 53% thickening at 50% time, and 78% at 75% time. For normals, the mean values at 25%, 50%, and 75% were 31%, 48%, and 77%. Thus, for both groups, thickening proceeded similarly and linearly (table 5, fig. 3). Relaxation was an alinear process. As an example, for the normal group in year 1, 31% of relaxation occurred within the first 10% of diastole, 68% occurred at the end of 20% of diastole, and 87% occurred when diastole was 40% completed. For each time range, boys with DMD demonstrated slower relaxation rates. Relaxation proceeded at a significantly slower (p < 0.05) rate of 22%, 51%, and 80% for 10%, 20%, and 40% of diastolic time, respectively (table 5, fig. 3). TABLE 4. Comparison of Means and Standard Deviations for Wail Thickness at a Percent of Systolic and Diastolic Time Control year Control year DMD year DMD year 1 1 2 2 Wall thickness (n = 24) (n = 24) (n = 32) (n = 32) (mm) at Significance 6.0 1.6 8.1 1.2 1.5 7.3 5.8 1.5 25% S time a, b, c 7.1 1.6 6.9 1.8 8.8 v 1.7 9.7 1.5 50% S time a, b, c 8.1 1.8 11.0 1.9 1.9 1.7 7.8 b, c 10.5 75% S time 1.8 2.0 9.0 2.1 8.7 11.9 12.0 1.8 a, b, c 100%o S time 2.0 1.7 7.8 7.8 10.0 2.0 10.0 1.7 b, c 10% D time 1.6 1.6 6.8 b, c 6.6 8.0 - 1.4 7.8 1.5 20% D time 5.9 1.8 1.4 1.4 7.0 - 1.1 5.5 6.8 b, c 40% D time 1.3 5.0 1.3 4.8 6.1 1.2 6.3 - 1.1 b, c 100% D time Differences between the means for DMD patients year 1 and year 2 were not significant. a = p < 0.05 between the means for controls year 1 and 2. b = p < 0.05 between the means for controls year 1 and DMD patients year 1. c = p < 0.05 between the means for controls year 2 and DMD9patients year 2. Abbreviations: S = systolic; D = diastolic; DMD = Duchenne's muscular dystrophv. 1066 CIRCULATION VOL 62, No 5, NOVEMBER 1980 12 11 * CONTROL P< .05 9 FIGURE 2. Change (in mm) in wall thickness for systole (left) and diastole (right). The dashed line represents controls and the solid line represents boys with Duchenne's muscular dystrophy (DMD). The cross-hatched lines indicate that the difference between means for a time period 7 5 4 3 2 50 25 75 Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017 % TIME SYSTOLE is significant (p < 0.05). m 10) 80 100 % TIME DIASTOLE Difference in relaxation could also be noted by merely observing the wall thickness tracings. Figure 4 demonstrates four randomly selected normal tracings. All curves showed biphasic relaxation, and this configuration was a uniform characteristic of the normal group. The initial phase of relaxation is rapid wall thinning followed by a slower phase. The lower panel of this figure demonstrates four types of relaxation curves found for boys with DMD. The least common (lower left) was a normal curve. Most had tracings similar to those in the middle two panels. Both panels show slowing of wall thinning during relaxation. The left middle trace shows two recognizable phases of thinning, but the right middle example demonstrates a single slow phase in diastole. Older patients, who had more severe muscular dystrophy, had traces that were similar to the right lower tracing. In these subjects contraction started longer after the QRS, wall thickness increased less, and diastole had a single very slow non-phasic slope. Wall Tracing Repeatability Wall tracings results were shown to be highly repeatable by repeat tracing of the same and different complexes on a given record and by evaluating the results of tracings obtained 1 year apart (fig. 4). Correlation of Age, Size, Heart Rate and Blood Pressure to Contraction and Relaxation Measurements Low-level (r = 0.28 to 0.60) but significant correlations (p < 0.05) were found between measurements obtained at a percent of systolic or diastolic time, and age, weight, height and body surface area. Heart rate showed a very weak (r = -0.34 to -0.49) negative, but significant (p < 0.05) correlation to contraction and relaxation measurements. Despite the statistical significance of the correlations, the level of correlation was too low to be of clinical importance. TABLE 5. Comparison of Percent Contraction at a Percent of Systolic and Diastolic Time Control year Control year 1 (n = 32) 2 (n 32) DMD year 1 (n = 24) 31.2 8.1 48.3 f12.5 76.9 9.9 31.7 60.3 82.8 7.7 7.2 5.3 26.2 53.1 78.0 DMD year 2 (n = 24) Significance % contraction at 25%oS time 50'% S time 75%:,S time 12.2 14.6 i 12.8 27.0 54.3 79.0 11.4 11.7 10.1 % relaxation at 1QC D time 31.9 11.6 34.0 16.5 22.3 13.8 31.0 19.6 20% D time 68.4 17.9 68.2 16.9 51.4 i23.5 55.0 - 23.2 40% D time 87.7 11.5 86.0 10.3 80.1 14.0 16.1 75.7 Differences between the means for DMD patients year 1 and year 2 were not significant. p < 0.05 between the means for controls year 1 and 2. p < 0.05 between the means for controls year 2 and DMD patients year 2. p < 0.05 betweeni the means foi controls year 1 and DMD patients year 1. Abbreviations: S = systolic; D = diastolic; DMD = Duchenne's muscular dystrophy. a b = = c = a, b a c b, c b, c CONTRACTION AND RELAXATION OF LV WALL/Goldberg et al. 1067 100 ------* COM X9 P<.05 950 I- 40 El 20 FIGURE 3. Data offigure 2, normalized by plotting the percent of thickening or thinning at a percent of systolic or diastolic time. Boys with Duchenne's muscular dystrophy (DMD) and normal subjects thicken linearly in systole. However, diastole shows a slower rate of thinning in DMD than normal (p < 0.05). 10 25 75 50 20 100 %SYSTOLIC TIME 40 60 60 1W) % DIASTOLIC TIME NORMALS Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017 1 cm except an noted ~~~~~.31 1 DUCHENNES FIGURE 4. The top four tracings were randomly selected from the normal group and the bottom panel shows traces for Duchenne's muscular dystrophy patients. Each trace starts and stops at the onset of a QRS. See text for detailed interpretation. Abbreviation: MN mainly normal; SR = slow relaxation, LR = loss of biphasic relaxation; Tt = increased time from QRS until contraction. = / .51 MN 1 SR . SR, LR SR,LR9T+ Interpretation of Two-dimensional Echocardiogram Two-dimensional echocardiograms did not reveal detectable left ventricular akinesis or dyskinesis in any patient. Discussion The unique feature of this investigation is the use of digitized LVPW echocardiograms to demonstrate that a major component in the Duchenne's cardiomyopathy is inability to thin normally during diastole. The heart in DMD has received considerable attention. One of the earliest findings was an abnormal electrocardiographic pattern in approximately 90% of affected boys.6 This was characterized by an increased net R-S, RSR' or polyphasic R in lead V,. Deep T waves were also found in the left precordium. However, the ECG is not indicative of the state of the disease or myocardial involvement.8 Tachycardia is usually present. The size of the heart on radiograph is variable and may be difficult to interpret because of severe skeletal deformities.8 The most common techniques for evaluating myocardial function rely on changes in the left ventricular cavity. Although cavity size and a change in cavity during the cardiac cycle would be expected to reflect, in part, the state of the myocardium, these cavity sizes are clearly affected by numerous factors, only one of which is myocardial function. None- theless, with these techniques, marked depression in myocardial function can usually be separated from normal function,22 but subtle or perhaps even moderate structural changes may go undetected. In a similar manner, systolic time intervals are a function of many variables,23 but may not detect subtle changes in the myocardium in children. Perhaps it is not surprising that these indicators are normal in DMD. Evaluation of LVPW by M-mode echocardiography is not simple, and this is probably why it has been infrequently evaluated. However, Kovick and coworkers'0 and Ahmad et al.9 found diastolic endocardial velocity (DEVM) to be the most sensitive method for detecting the abnormality in DMD. However, DEVM is a problematic measurement. Most important, it neglects the fact that the myocardium separates from the pericardium to a variable extent in systole. This epi-pericardial separation was found in 100% of our patients and its detection is principally a function of meticulous techniques and axial resolution. Axial resolution, in this instance, is complicated because the distance between the transducer and the area of interest is maximal in studying the epipericardial separation of the posterior wall. At this depth, the signal-to-noise ratio of the echograph is at its lowest for cardiac examination. The magnitude of the separation is not apparent in the figures of Kovick and co-workers or those of Ahmad and coworkers.9' 1' We could record the separation by in- 1068 CI RCULATION Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017 creasing the echocardiographic receiver gain in each stage of the receiver board. We also increased the dynamic range of the echograph with switch gain." The latter appears to be more important than the former. Observation of tracings leads to the suspicion that the larger the epi-pericardial space, the greater would be the DEVM; the reverse also seems true. Factors that govern the size of the space are unclear. It could result from motion of the entire heart within the pericardium, heart size, the amount of pericardial fluid, or from all these factors. Perhaps DEVM is also affected by heart rate, as cardiac motion might be expected to be decreased if the stroke index were smaller due to tachycardia. Patients with DMD did have relative tachycardia and this could have been a factor in those slopes. The technique that we present makes no assumptions regarding the total cardiac motion, for tracing both sides of the left ventricular wall cancels the effect of cardiac motion and permits evaluation of cyclic thickening and thinning. Further, the technique of Kovick and co-workers requires drawing the best tangent to a moving wall.'0 This can be very difficult, for the wall is both thinning and moving, each at a different rate. The technique we present does not require construction of tangents. The repeatability studies for the presented technique show a high degree of reproducibility. The problem with the presented technique is obtaining very high quality recordings, and such a recording requires considerably more time, effort, knowledge of the equipment, and to an extent, equipment modification. Our technique makes two major assumptions. The first is common to all echocardiographic work, and proposes that returned echoes come from structures that are perpendicular to the ultrasonic beam and that the myocardium of the left ventricular posterior wall is relatively uniform in thickness if the operator takes care not to image the papillary muscles. Since few nonperpendicular echoes return to the transducer, or if they do return to the transducer, they appear as weak echoes, the first part of the first assumption is probably true. Pathologic examination of the free wall of the left ventricle shows that it is generally of similar thickness from just below the mitral ring to near the papillary muscle. This is important, for a different portion of the left ventricular wall is imaged at each instant, since the left ventricle has motion in all three axes, and, in effect, passes by the motionless transducer.24 This portion of the first assumption, although not frequently discussed, is common to all echographic work. The second assumption is more specific to this investigation and concerns the possibility that the area of the left ventricular wall that was examined was not a representative section, as it could have been mainly a fibrous area or alternatively, the only contractile area of an otherwise fibrotic wall. To deal with this question, we performed twodimensional echocardiographic examinations of DMD patients. The left ventricle was imaged in cross section from the apex and in long axis. This examination did not define areas of akinesis or hypokinesis. Failure to find such areas suggested that our sample VOL 62, No 5, NOVEMBER 1980 site selected for M-mode study was reasonable. However, the value of such observation is limited because we could not rule out subtle systolic, or more important, diastolic events. Our investigation shows that thickening of the left ventricular wall in DMD and normals proceeds as a linear or nearly linear function. Diastole has two phases in normal subjects: a rapid thinning phase that occupies about the first 40% of diastole and a slow phase that lasts until slightly after the inscription of the QRS complex. Although rarely a normal pattern occurs in DMD, the most common pattern was one of decreased rate of wall thinning. Decreased rate of relaxation is probably related to fibrosis. Kovick and co-workers'0 suggested that since fragmented sarcoplasmic reticulum isolated from DMD skeletal muscle accumulates calcium more slowly than does fragmented sarcoplasmic reticulum isolated from normal muscles, the slow uptake of calcium may be accompanied by slow relaxation in DMD. Ahmad et al.9 suggested that reduced DEVM may reflect reduced overall movement of the heart in the thorax rather than functional cardiac abnormality.9 Cardiac motion may be a major factor in DEVM, so this conclusion may be partially appropriate. However, the present study shows that the abnormal diastolic thinning is not a function of cardiac motion because effects of cardiac motion are, in effect, canceled by the procedure. Accordingly, the abnormal diastolic thinning of the left ventricle appears to be the major impairment that could be detected by the echocardiographic technique of this study. References 1.Perloff JK, Roberto WC, DeLeon AC Jr, O'Doherty D: The distinctive electrocardiogram of Duchenne's progressive muscular dystrophy. Am J Med 42: 179, 1967 2. Griggs RC, Reeves W, Moxley RT III: The heart in Duchenne dystrophy. In Pathogenesis of Human Muscular Dystrophies, edited by Roland LP. Amsterdam, Excerpta Medica, 1977, p 661 3. Sanyal S, Johnson WW, Thapar MK, Pitner S: An ultrastructural basis for electrocardiographic alterations associated with Duchenne's progressive muscular dystrophy. Circulation 57: 1122, 1978 4. Frankel KA, Rosser RJ: The pathology of the heart in progressive mucular dystrophy: epimyocardial fibrosis. Hum Pathol 7: 375, 1976 5. Siegel IM: Cardiomyopathy: presenting symptoms of progressive muscular dystrophy. JAMA 222: 1060, 1972 6. Slucka C: The electrocardiogram in Duchenne's progressive muscular dystrophy. Circulation 38: 933, 1968 7. Perloff JK, deLeon AC, O'Doherty D: The cardiomyopathy of progressive muscular dystrophy. Circulation 33: 625, 1976 8. Heymsfield SB, McNush T, Perkins JV, Felner JM: Sequence of cardiac changes in Duchenne muscular dystrophy. Am Heart J 95: 283, 1978 9. Ahmad M, Sanderson JE, Dubowitz V, Hallidie-Smith KA: Echocardiographic assessment of left ventricular function in Duchenne's muscular dystrophy. Br Heart J 40: 734, 1978 10. Kovick RB, Fogelman AM, Abbasi AS, Peter JB, Pearce ML: Echocardiographic evaluation of posterior left ventricular wall motion in muscular dystrophy. Circulation 52: 447, 1975 11. Griffith JM, Henry WL: Switched gain - a technique for simplifying ultrasonic measurement of cardiac wall thickness. IEEE Trans Biomed Eng 22: 337, 1975 12. Sahn DJ, DeMaria A, Kisslo J, Weyman A: Recommendations CONTRACTION AND RELAXATION OF LV WALL/Goldberg regarding quantitation in M-mode echocardiography: results of of echocardiographic measurements. Circulation 58: 1072, 1978 Cooper RH, O'Rourke RA, Karliner JS, Peterson KL, Leopold GR: Comparison of ultrasound and cineangiographic measurements of the mean rate of circumferential fiber shortening in man. Circulation 46: 914, 1972 Gutgesell HP, Paquet M, Duff DF, McNamara DG: Evaluation of left ventricular size and function by echocardiography. Results in normal children. Circulation 56: 457, 1977 Hirschfeld S, Meyer R, Kaplan S: Measurement of right and left ventricular systolic time intervals by echocardiography. Circulation 51: 304, 1975 Sahn DJ, Terry R, O'Rourke L, Leopold G, Friedman WF: Multiple crystal cross-sectional echocardiography in diagnosis of cyanotic congenital heart disease. Circulation 50: 230, 1974 Silverman NH, Sphiller NB: Apex echocardiography a twodimensional technique for evaluating congenital heart disease. Circulation 57: 503, 1978 Rogers EA, Feigenbaum H, Dillon JC, Heger J: Predicting survival of myocardial infarction by cross-sectional echo. Circulaa survey 13. 14. 15. 16. 17. 18. - et al. 1069 tion 58: 233, 1978 19. Hirshleifer J, Crawford M, O'Rourke RA, Karliner JS: Influence of acute alteration in heart rate and systemic arterial pressure on echocardiographic measures of left ventricular performance in normal human subjects. Circulation 52: 835, 1975 20. Epstein M, Goldberg SJ, Allen HD, Konecke L, Wood J: Great vessel, cardiac chamber, and wall growth patterns in normal children. Circulation 51: 1124, 1975 21. Meyer RA, Stockert J, Kaplan S: Echocardiographic determination of left ventricular volumes in pediatric patients. Circulation 51: 297, 1975 22. Sahn DJ, Vaucher Y, Williams DE, Allen HD, Goldberg SJ, Friedman WF: Echocardiographic detection of large left-toright shunts and cardiomyopathies in infants and children. Am J Cardiol 38: 73, 1976 23. Weissler A, Harris WS, Schoenfeld CS: Systolic time intervals in heart failure in man. Am Heart J 37: 149, 1968 24. Bhatt DR, Isabel-Jones JB, Villoria GJ, Nakazawa M, Yabek SM, Marks RA, Jarmakani JM: Accuracy of echocardiography in assessing left ventricular dimensions and volume. Circulation 57: 699, 1978 Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017 Echocardiographic determination of contraction and relaxation measurements of the left ventricular wall in normal subjects and patients with muscular dystrophy. S J Goldberg, L Feldman, C Reinecke, L Z Stern, D J Sahn and H D Allen Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017 Circulation. 1980;62:1061-1069 doi: 10.1161/01.CIR.62.5.1061 Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1980 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7322. Online ISSN: 1524-4539 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circ.ahajournals.org/content/62/5/1061 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation is online at: http://circ.ahajournals.org//subscriptions/