Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Coronary artery disease wikipedia , lookup
Heart failure wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Jatene procedure wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
430
Isolated Cat Trabeculae in a Simulated Feline Heart and
Arterial System
Contractile Basis of Cardiac Pump Function
Gijs Elzinga and Nico Westerhof
From The Laboratory for Physiology, Free University, Amsterdam, The Netherlands
Downloaded from http://circres.ahajournals.org/ by guest on June 14, 2017
SUMMARY. Isolated cat trabeculae were studied under conditions resembling those present for the
muscle fibers in the wall of the left ventricle. To obtain such a situation experimental animals,
perfusion fluid, temperature, stimulation frequency, peak stress values, contraction sequence, length,
and force control were chosen with respect to that criterion. Results were compared with those
described for the intact feline heart in previous studies. Special emphasis was placed on determinants
of the pump function graph, i.e., the relationship between mean ventricular pressure and output. It
was found that peak isometric stress values measured in the trabeculae were about twice as high as
those existing on average at the base of the intact left ventricle in the circumferential direction.
However, the duration of the mechanical activity, as measured in iso(volu)metric contractions, was
in the isolated trabeculae (206 msec) significantly less (P < 0.01) than found in intact right (292
msec) or intact left ventricle (344 msec). Furthermore the (maximum) output of the intact left
ventricle at end-diastolic pressure could not be accounted for in a simple manner by the maximum
amount of shortening found in isolated trabeculae. The points of the pump function graph obtained
by varying the input impedance of the loading arterial system over a wide range of compliance and
resistance values in the steady state deviated only little from the graph obtained from a series of
constant pressure levels applied in a beat-to-beat fashion. Therefore, the insensitiviry of the pump
function graph to the nature of the arterial load is found in the intact heart as well as in isolated
cardiac muscle. (Cite Res 51: 430-438, 1982)
FOR left (Elzinga and Westerhof, 1978, 1979, 1980)
and right (Elzinga et al., 1980) heart, we have shown
that ventricular pump function can be described by
a relationship between output and mean ventricular
pressure. This relationship is found by alterations in
arterial pressure, obtained through either variations
of the arterial input impedance or through sudden
changes in arterial pressure with an external pressure
source. When changes in arterial input impedance
were used to obtain the pump function graph, we
could show that the ventricle was insensitive to the
nature of the change (Elzinga and Westerhof, 1979),
i.e., changes in peripheral resistance yielded points on
the same curve as changes in arterial compliance.
However, especially for the right heart, it was clear
that slightly different relationships were found with
sudden pressure changes and with pressure changes
in the steady state (Elzinga et al., 1980).
It is of importance to know whether insensitivity to
the type of the pressure changes resulting from arterial input impedance variations resides also in cardiac
muscle fibers or that it should be attributed to the
complexity of ventricular geometry and the arrangement of the muscle fibers and the activation sequence.
To distinguish between these two possibilities, we
have determined "pump function" graphs from isolated cat trabeculae studied under conditions chosen
to resemble the intact heart as closely as possible,
though lacking geometrical complexities and distributed activation patterns as found in the ventricle.
Methods
Muscle Preparation
Thin, cylindrically shaped trabecular muscles were taken
from male cats (2250-2900 g) as previously described by
Elzinga and Westerhof (1981); see Table 1 for cross-sectional areas. The muscles were dissected free from the heart
under the microscope, and one end was tied with a thin
(10-0) monofil suture to a small platinum hook made of 0.1
mm in diameter plantinum wire (p in Fig. 1). The other end
of the muscle remained attached to a relatively large piece
of myocardium. The muscle then was transferred in a small
vessel to the muscle bath.
The plantinum hook was inserted into a hole (0.15 mm
in diameter) present in a small metal extension attached to
the force transducer (Fig. 1). The lump of tissue at the other
end of the muscle was gripped by four stainless steel hooks
in such a way that the origin of the muscle was just free of
the clamp. The hooks then were attached to the coil of the
muscle puller via an arm. The muscle bath was perfused
with temperature-controlled oxygenated Tyrode's solution.
More details of the set-up have been presented earlier
(Elzinga and Westerhof, 1981). In that study the same
muscles were used for a different purpose.
Force and Length Control
A muscle puller (Fig. 1) was used to control either the
length or the force of the muscle. The puller was constructed
from a loudspeaker coil and magnet assembly (Philips
AD125HP4).
Changes in muscle length were measured by a position
transducer mounted on the coil. The amplitude frequency
Elzinga and Westerhof/Contractile Basis of Pump Function
431
TABLE 1
Further details pertinent to the Experiments
23-10
25-10a
25-10b
26-10
29-10
Cross-sectional area
(mm2)
0.060
0.072
0.034
0.037
0.058
Working muscle length
(mm)
3.2
3.4
3.0
3.4
3.5
Preload (N-mm~2)
0.0016
0.0019
0.0031
0.0027
0.0016
Percentage shortening at
preload (%)
24.4
20.3
20.0
22.1
mean ± SD
0.0022 ± 0.0007
20.0
21.4 ± 1.9
Downloaded from http://circres.ahajournals.org/ by guest on June 14, 2017
Developed isometric
stress at working
length (N-mm~2)
0.045
0.033
0.036
0.057
0.042
0.043 ± 0.009
Developed isometric
stress at optimal length
(N-mm~2)
0.074
0.077
0.056
0.066
0.068
0.068 ± 0.008
Experimental stability (%)
98.6
103.3
response of the length measurement thus obtained was flat
to over 10 kHz, its noise level was equal to 5 fan, and its
linearity was within ±0.5% (Elzinga and Westerhof, 1981).
An Aksjeselskapet Mikro-Elektronikk AE 801 transducer
was used to measure force. To improve sensitivity, a small
extension was glued onto its end. Total transducer compliance: 1 mm/N; frequency response: 5 kHz; noise: 15 fiN.
Details on force and length control were given earlier
(Elzinga and Westerhof, 1981).
micrometer
adjust
96.7
100.3
100.0
Experimental Conditions
The experiments were designed for the isolated trabeculae to resemble the myocardial fibers in the wall of the
isolated cat heart used in our earlier studies (Elzinga and
Westerhof, 1973, 1978; Elzinga et al., 1980). Therefore, the
experimental animals were taken from the same stock of
male adult cats, although, for practical reasons, the animals
were somewhat smaller than those used for the intact heart
puller
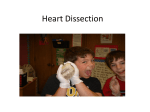
FIGURE 1. Isolated heart muscle set-up. The muscle is attached on one side to the force transducer (p) and gripped on the other side by four
bent stainless steel hooks (h). The muscle bath is perfused with Tyrode's solution and the overflowing fluid (o) is pumped back to a central
reservoir (not shown). The muscle bath is surrounded by a water jacket (w) to minimize temperature loss. The bent stainless steel pins are
attached to an arm which connects the muscle with the coil of the muscle puller. The coil is suspended in a magnetic field. The suspensions,
which are not shown in the figure, allow movement of the coil-muscle assembly in the length direction only. The position of this assembly
is registered by an optical position transducer. The force transducer is connected to a micrometer. Force and length signals are fed into an
electrical analog of the cylindrical (2D) ventricular model and "pressure" and "volume" are derived.
Circulation Research/ Vol. 51, No. 4, October 1982
432
O.O5
nj
'E
Z
I o
5min.
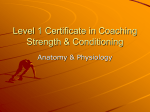
FlCURE 2. A change in stimulation frequency from 0.2 to 2 Hz
causes an increase in isometric force during the first 2 minutes. If
the preparation is sufficiently thin, force remains then at a stable
level.
Downloaded from http://circres.ahajournals.org/ by guest on June 14, 2017
studies. Temperature control was such that the temperature
measured in the bath was about 37.5°C. Temperature differences between experiments were less than 1°C. Fluctuations during the experiments, as measured with a thermometer with an RC time of about 1 minute (Yellow Springs
43TZ), were less than 0.2°C. The oxygenated perfusion
fluid used for the muscle experiments had the same composition as that used in our cardiac studies. Oxygenation
was performed with a gas mixture of 95% O2 and 5% CO2,
resulting in the bath in: P02, 492 ± 8 (SD) mm Hg; PCO2, 35.1
± 1.8 (SD) mm Hg, and pH 7 .31 ± 0.03 (SD).
Stimulation frequency of the isolated muscles in this
study was 2 Hz. This is the same frequency as the 120
beats/min used in most of our studies on the isolated cat
heart. Muscle stimulation was performed with rectangular
pulses of 1 msec duration above threshold. The stimulator
changed the polarity of the electrodes every impulse.
We have used for this study muscles with cross-sectional
areas less than 0.06 mm2 (Table 1). The following arguments
can be put forward to support the idea that the performance
of such small muscles under these conditions is not limited
by diffusion of oxygen. (1) When stimulation of the muscles
at a frequency of 2 Hz was started, isometric force increases
considerably during the first 2 minutes (see Fig. 2). If
metabolic depression due to inadequate diffusion develops,
it is likely to occur during this initial period. However, an
increase followed by a decrease in force during this time
was found only when muscles with a cross-sectional area
larger than approximately 0.20 mm2 were used. (2) After
the initial increase in isometric force, a stable level is
reached. Although we have not investigated the precise time
course over hours, this indicates that no progressive metabolic depression develops after the first 2 minutes. (3) Peak
isometric stress generated by the isolated trabeculae is at
least equal to that estimated for the myocardial fibers in the
ventricular wall (see next paragraph, and the Discussion).
(4) On the basis of the diffusion equation given by Hill
(1965) for a cylindrical muscle, and assuming an oxygen
consumption of 0.1 ml/g per min, one can calculate the
critical diameter (450 ^m, corresponding to a cross-sectional
area of 0.16 mm2) which is still compatible with an adequate
supply of oxygen (Gibbs, 1978). The size of the muscles
used was well below this critical value (see also Table 1).
Calculations based on measurements of pressure and
dimensions show that peak stress in the circumferential
direction at the base of the left ventricle during ejection is
about 100 g/cm2 (Huisman et al., 1980). Since most of the
muscle fibers at that location run circumferentially (Streeter
et al., 1969), we have assumed that the muscles should at
least be able to generate 2.5 times that stress isometrically
(Elzinga et al., 1980). Therefore, a working length (preload)
was chosen such that isometric force was about 0.025
Nmm 2, as based on an initial rough estimate of the muscle's
cross-sectional area. This length was approximately twothirds of that at Una*. No other lengths were studied. Data
on the working lengths in relationship to Lmol, the maximum
developed isometric stress at this working length and at
Lmax, are given in Table 1. These measurements were carried
out at the end of the experiment. Thereafter, the precise
cross-sectional area was determined by measuring the diameter with a microscope at 40X in two perpendicular
directions in the middle of the muscle using a mirror and
applying the formula for the area of an ellipse. All forces
were finally scaled to this correct area.
As has been reported by other investigators (Sulman et
al., 1974; Brutsaert and Paulus, 1977; Westerhof and Elzinga,
1978; Wiegner and Bing, 1977, 1978; Paulus et al., 1979),
the order of contraction found in the ventricle, i.e., isovolumic contraction, ejection, isovolumic relaxation, and filling, has to be realized for the muscle. Force is to be
compared with pressure and length with volume, so that
the muscle contraction starts in length control, followed by
force control, succeeded by length control again, and ending
in force control.
The muscle should be considered as part of the ventricular wall. Since cardiac architecture and fiber direction in
the myocardium are very complex, gross simplifications
have to be used to represent the ventricle. We have chosen
a thin-walled cylinder with fibers running in the circumferential direction: the 2D pump described by Gabe (1974).
Force and pressure, and length and volume, in this model
are related by:
Vt = k, (Lr - ALt)2 = k,Lt:
Pt = k2
(1)
(2)
where Vt is volume, U is muscle length, Lr is resting muscle
length, AL is the change in muscle length, P is pressure, F
is force, ki and k2 are constants, and the subscript t indicates
time. These equations were part of the muscle control unit
such that P and V could be controlled instead of length and
force (see above). Inputs for the control unit were force,
resting length, and length change from the position transducer. Factors ki and k2 were the same in all experiments.
Isovolumic pressure at the working length was taken as
100%. All aortic flow values were expressed as percentage
of maximal flow, which was the flow obtained by letting
the muscle shorten under the preloaded force and converting the shortening rate in volume flow rate per second.
A comparison between heart and muscle in this way may
lead to a confusing terminology, because now pressures and
flows may be measured in cardiac as well as in muscle
experiments. To avoid confusion, we have placed words
like pressure, flow, isovolumic, etc., in quotes when measured in muscle experiments.
Arterial input impedance was obtained by an R-C-R
network (Westerhof et al., 1971). The first derivative of the
"volume" change ("aortic blood flow") was taken as a
current input for this network. The resulting voltage was
used as the "aortic pressure." The control values of the
resistances and the compliance were chosen according to
the following criteria: (1) To be comparable with the isolated
heart studies, the control "pressure" value in the 2D pump
should be about 40% of the "isovolumic pressure" at the
working length. This value was approximated roughly by
setting the resistance Rp, which represents peripheral resistance. In practice, this means lower Rp for a longer
muscle. (2) The compliance, representing total arterial compliance, was chosen in such a way that an RPC time of 1
433
Elzinga and Westerhof/Contractile Basis of Pump Function
second was obtained. (3) Resistance Re, representing the
characteristic impedance of the aorta, then was set at a value
close to 10% of that found for the resistance Rp.
Apart from this physiological load, we could also introduce a fixed "ejection pressure load" level as a load for the
pump. It was possible to switch from one load to another
on a beat-to-beat basis.
Experimental Protocol, Recording, and Analysis
Downloaded from http://circres.ahajournals.org/ by guest on June 14, 2017
After we had mounted the muscle we allowed it to reach
a steady state by letting it contract isometrically with a
frequency of 2 Hz, for about 20 minutes. Then we started
the imitated ventricular contraction pattern, defined as control situation. From this control situation, fixed "arterial
pressure" levels were applied every 10th beat, the highest
level giving an isometric contraction. A series of about 10
of these "pressure" levels was given, sandwiched between
two isometric contractions. After this series of loads, we
studied a total of nine steady state loads similar to the ones
reported by Elzinga and Westerhof (1973) for the left ventricle and by Elzinga et al. (1980) for the right ventricle.
Three values of "peripheral resistance" (control and about
twice and five times control) were accompanied by three
values of "total arterial compliance" (control and about 50%
and 20% of control), resulting in a total of nine "arterial
input impedances." The control situation was the first of
the series of nine. The "impedance" resulting from the
maximum "peripheral resistance" and minimum "total arterial compliance" was subsequently used as the steady
state situation from which another series of "pressure"
levels was imposed. In this way, two series of "pressure"
levels were studied, one from the smallest "arterial impedance" and one from the largest one. The two extreme
"arterial impedances" made it possible to study the effect
of a steady state load on the "pump function" graph. After
the second series of "pressure" levels, the original control
situation was established again and a single isometric contraction was evoked. This last isometric contraction was
compared with the first one measured during the first series
of "pressure" levels to test stability of the preparation over
the whole experiment. Stability was given as the ratio
between the means of these "isovolumic ventricular pressures" times 100.
"Aortic pressure," "ventricular pressure," "aortic flow,"
"ventricular volume," muscle force, muscle length, stimulus, and trigger pulses were recorded on an Elema Schonander ink recorder (EMT 81) and an SE analog tape recorder
(SE 7000). For the measurements of peak values, values at
a given time and average values use was made of an analog
device especially designed for such a purpose (Puls and
Elzinga, 1978). Preload pressure was taken as zero implying
the use of developed pressures in the results.
second was chosen. Waveforms recorded in the other
muscle experiments were virtually identical to those
presented in Figure 3. The results shown in Figure 3
should be compared with those presented in Figure 3
of Elzinga and Westerhof (1973) for the left ventricle
and with those shown in Figure 2 of Elzinga et al.
(1980) for the right ventricle. The similarity in the
waveform patterns is striking. As is the case in the
intact ventricle, in the muscle, the shape of the
"ventricular pressure" curve is more affected by lowering the "arterial compliance" by a factor of 5 than
1.O
4
-
c
7
5Or
T
1.O
2
B
1.B
6
3
S
n
1
4.7
4
7
1
1.O
2
5O,
5
B
1.B
! \
B
3
r\
3
4.7
A
1
4
7
1.O
2
5
S
1B
Results
Individual and averaged data on the muscles are
given in Table 1. All-cross sectional areas were less
than the critical value of about 0.16 mm2 and all
isometric forces at working length were larger than
0.025 N-mm"2.
"Aortic pressures," "ventricular pressures," and
"aortic flows" generated by the isolated muscle in
nine situations with different "input impedances" of
the loading "arterial system" are shown in Figure 3.
The resistance and compliance values used in this
particular experiment are given in the figure. Note
that for the situations 1, 5, and 9, an RPC time of 1
0.22
O.57
1
^^^
5O|
B
4.7
O'
FIGURE 3. Nine steady state situations with a different input impedance of the loading "arterial" system were studied. The situations
were obtained by combining three values of the "peripheral resistance" with three values of the "total arterial compliance." One beat
of each situation was taken to compose the above Figure.
"Ventricular pressures" (upper panel), "aortic flows" (middle
panel), and "aortic pressures" (lower panel) are given in percentages of their own maximum value. Resistance values are given in
Mil and compliance values in pF.
434
Downloaded from http://circres.ahajournals.org/ by guest on June 14, 2017
by increasing the "peripheral resistance" 5 times.
Similarly, peak "blood flow" is more affected by an
increase in "resistance" (1, 2, 3) than by a decrease in
"compliance" (1, 4, 7). Moreover, as has been found
in aorta (Elzinga and Westerhof, 1973) and pulmonary
artery (Elzinga et al., 1980), changes in shape of the
"arterial pressure" trace are dominated by the changes
in RC time. However, that this is not the sole determinant can be seen by comparing panel 1 with panel
9, showing two situations with the same RC time at
different "aortic pressure" levels.
In spite of these similarities in behavior of isolated
muscle and intact heart, some differences can be seen
as well. In the present study, no incisura is found in
the "aortic pressure" and no "backflow" can be seen
in the "flow." This difference is not related to differences in contractile behavior between heart and muscle, but is due to the fact that no "backflow" is needed
in our muscle control unit to close the "valve" between "ventricle" and "aorta." A slight difference can
also be seen in the "blood flow" pattern shown in
situation 9. The small initial overshoot found for both
left and right intact ventricle (Elzinga and Westerhof,
1973; Elzinga et al., 1980) in the comparable situation
is not present in the muscle. However, in the intact
heart studies, relatively lower compliance values have
been used. At these very low values, the residual
arterial compliance was probably located mainly in
the remnants of the aorta and pulmonary artery instead of in the air volume representing total arterial
compliance. This would render the "arterial systems"
used in heart and muscle studies incomparable at
these extreme settings.
A fundamental difference between the results obtained in the intact heart and the findings in this
isolated muscle study is the duration of contraction.
The ventricular pressure pulses obtained in left and
right ventricle last longer than the "ventricular pressure" pulse in the present study. In isovolumic beats
the duration of the pressure pulse was measured for
the right and the left ventricle at 10% of the peak
pressure value [data obtained from experiments described by Elzinga et al. (1980)]. The average duration
for the left ventricle (n = 11) was 344 ± 49 msec and
for the right ventricle (n = 11) 292 ± 16 msec. In this
study, 206 ± 8 msec was found in five isolated muscles
for the corresponding time (see Table 2). The differences are statistically significant (P < 0.01; Wilcoxon
matched pairs signed rank test, Mann-Whitney U
test).
From the nine steady state situations (Fig. 3), as
well as from the two series of beat-to-beat "pressure"
changes, mean "output" and mean "ventricular pressure" values were determined. The "pump function"
graphs obtained in this way are presented for all five
experiments in Figure 4. In each graph, five different
symbols are found. Values obtained during the first
series of beat-to-beat "pressure" changes are indicated with small dots; small plusses represent the
values obtained during the final series of sudden
Circulation Research/ Vol. 51, No. 4, October 1982
TABLE 2
Duration of Contraction* in Heartf and Isolated Trabecula
Experiment
Right
ventricle
Left
ventricle
19-10-78
24-10-78
26-10-78
31-10-78
30-11-78
01-12-78
12-01-79
16-01-79
18-01-79
30-01-79
08-02-79a
307
292
312
312
292
302
267
277
292
287
267
347
361
391
351
287
436
282
317
307
396
307
23-10-79
25-10-79a
25-l-79b
26-10-79
29-10-79
mean ± SD
Isolated
trabecula
209
197
199
208
217
292 ± 16
344 ± 49
206 ± 8
The duration of contraction of the right ventricle is significantly
less {P < 0.01) than that of the left ventricle (Wilcoxon matched
pairs signed rank test). The duration of contraction of the isolated
trabeculae is significantly less (P < 0.01) than that of the right
ventricle (Mann-Whitney U test).
* The duration of contraction is given as the width (msec) of the
isovolumic presssure pulse at 10% of peak (developed) pressure.
f Left and right ventricular isovolumic beats were obtained from
the same hearts. The experiments from which the data have been
taken are described by Elzinga et al. (1980).
"pressure" changes (muscle contracting as in situation
9 of Figure 3). Data obtained during the nine steady
state situations (Fig. 3) are indicated with larger symbols (normal C: open squares; medium C: open triangles; small C: open circles). Stability of the preparations was obtained from the mean "isovolumic ventricular pressures" at the start and at the end. Stability
was better than 4%. Figure 4 shows that a small but
consistent deviation, especially near the "pressure"
axis, can be found between the two "pump function"
graphs obtained on a beat-to-beat basis, the one obtained during situation 9 (small plusses) being the
lower in all experiments. This implies that contractile
behavior of the preparation was slightly dependent
on the steady state loading conditions. This phenomenon is similar in direction to the one described by
Parmley et al. (1969) and by Jewell and Rovell (1973)
for isolated heart muscle.
The "pump function" graph of the isolated trabeculae, as determined on a beat-to-beat basis, has a
sigmoidal shape (Fig. 4). The steady state data deviate
slightly from both lines drawn through the values
obtained on a beat-to-beat basis. Even the steady state
values as measured in between the single beats with
different isotonic loads (i.e., lowest open square, obtained from situation 1 of Figure 3, and highest open
circle, from situation 9 of Figure 3), deviated from the
Elzinga and Westerhof/Contractile Basis of Pump Function
435
25.1O A
S3 no
2B.1O
S3.1O
25.1OB
steady
state
D 1,2,3
V 4,5,6
O 7,B,S
beac Co beat
• in 1
• in 3
Downloaded from http://circres.ahajournals.org/ by guest on June 14, 2017
2O
4D
BO
BO
2O
mean
4O
BO
BO
2O
4O
BO
BO
"output; C°/o)
FIGURE 4. "Pump function" graphs obtained by varying the "arterial" load in steady state situations (large open symbols) or on a beat-tobeat basis. The symbols are explained in file lower righthand panel. The numbers correspond to the numbers given in Figure 3. "Pressure"
and "output" are given in percentages of maximum.
relationship based on the beat-to-beat "pressure"
changes. However, all these deviations are rather
small.
Force and "pressure/' and length and "volume,"
are related to one another through the geometry of
the 2D model in this study (cf. Equations 1 and 2).
The effects of this cylindrical pump on the relationship between "pressure" and force is shown in Figure
5A. Here we have amplified the "pressure" and force
trace in such a way that they are superimposed during
an "isovolumic" beat. The two preceding contractions
in this example are contractions loaded as in the
control situation (situation 1 in Fig. 3). In these two
beats, force deviates from "pressure" during and after
shortening. Because of the steepness of the tracings
during relaxation, this difference is hardly visible in
that part of the cycle. In Figure 5B, the small but
consistent effect of the cylindrical pump on the
"pump function" graph is shown. The effect is small
but it seems that the S-shape is somewhat less pronounced in the relationship between mean force and
mean velocity of shortening than in the mean
"pressure" mean "output" relationship.
Discussion
The present study shows that isolated cat trabeculae
in a simulated feline heart and arterial system yield
responses to changes in "arterial load" qualitatively
similar to those found in intact hearts. We will now
try to answer the question, to what degree is such a
similarity also quantitative.
How Well do "Pressures" and "Flow" Generated by
the Isolated Muscles Compare with Those Found in
the Intact Heart?
To judge whether the force-generating capacity of
cardiac muscle is the same in the intact heart and
isolated trabeculae, we have chosen for convenience
to compare peak iso-(volu)metric stress values in the
two preparations. Such a comparison is complicated
by the fact that, in the intact heart, all muscle fibers
do not start the contraction at the same moment in
time as is the case in the isolated muscle. This asynchrony of contraction in the ventricular wall may
explain at least in part the significant differences
found between the durations of left ventricular contraction (344 msec), right ventricular contraction (292
msec), and the contraction of the isolated trabeculae
(206 msec) (Table 2).
The fact that not all muscle fibers in the left ventricular wall do contract at the same time must result
in a lower average peak stress value for that ventricle
than for the muscle if the peak stress generated by
the individual fibers is assumed to be the same in
both preparations. Although stress in the wall of the
ventricle is very difficult to measure (Huisman et al.,
1980), calculations from pressure and dimensions predict that, in ejecting dog hearts at normal pressures,
the peak of the stress value averaged over the left
ventricular wall in the circumferential direction is
between 0.01 and 0.02 N-mm~2 (Burns et al., 1971;
Huisman et al., 1980). Regarding the wide range, this
estimate can, without much doubt, be extrapolated
from the dog to the isolated intact cat heart because
Circulation Research/ Vol. 51, No. 4, October 1982
436
the smaller size of the latter corresponds roughly to
the thinner ventricular wall found in this species. We
therefore have assumed an average peak left ventricular wall stress in the circumferential direction of
0.015 N-mm~2 in ejecting beats as normal for the
isolated cat heart. In our isolated cat heart experiments
(Elzinga and Westerhof, 1978, 1980; Elzinga et al.,
1977, 1980), we have not found isovolumic left ventricular peak, pressures over 280 mm Hg. Suppose
that under normal circumstances the ejecting left
ventricle generates pressures of about 120 mm Hg,
then an average of left ventricular circumferential
peak stress value of 280/120 X 0.015 N-mirT2 is to
be expected during an isovolumic contraction. This
value of 0.035 N-mm" 2 is slightly less than the 0.042
N-mm~2 which we used on average at the working
length of the isolated trabeculae for the developed
1OO-
-5O
CD
E
E
u
CD
1OO-
(0
CO
CD
f_
Q.
-5O
L
J
Downloaded from http://circres.ahajournals.org/ by guest on June 14, 2017
3
0
L
CD
-5O
Q) 1 O D -
C
CD
CD
5O-
-5O
3
B
i
9
mean left ventricular
output Ccm3sec"/|]
FIGURE 6. Left ventricular pump function graphs, presented in a
previous study (Elzinga et al., 1980), were replotted. Apart from
experiment 30-1, a slight sigmoid shape of the pump function
graph may be present.
2O
6O
SO
"output" (O/b)
mean velocity of shortening CVo)
FIGURE 5. A: Force and "ventricular pressure" were displayed in
such a way that the two curves were superimposed under isometric
conditions. This implies that, because of the presence of the 2D
pump, superposition cannot occur during the "ejection" phase. B:
The effects of the geometrical configuration of the 2D pump on the
"pump function" graph can be noticed by comparing the mean
force mean velocity of shortening relationship with that between
mean "ventricu/ar pressure" and mean "output." All values are
given as percentages of their own maximum.
isometric peak stress value (see Table 1). The results
suggest that the preparations used in the present
study, under conditions similar to those of the isolated
cat hearts, develop stress values that are at least as
high as found in the intact ventricle. The developed
isometric stress at optimal length found in the present
study (0.068 N-mm~2) would predict, according to
the same reasoning as used above, the rather high
value of (0.068/0.015) X 120 = 544 mm Hg for the
maximum peak left ventricular pressure.
However, it should be stressed that a comparison
between force-generating capacity of the left ventricle
and isolated trabeculae is even more complicated than
suggested above. For instance, not all fibers in the
wall of the left ventricle run in the circumferential
direction (Streeter et al., 1969). This means that cir-
Elzinga and Westerhof/Contractile Basis of Pump Function
Downloaded from http://circres.ahajournals.org/ by guest on June 14, 2017
cumferential wall stress cannot, without correction for
fiber direction, be used in such a comparison. Although we estimated this correction factor to be probably less than 25%, it would make the stress value for
the circumferential fibers in the ventricle higher. On
the other hand, it is likely that the trabeculae used in
this study consist of a healthy central segment and
two damaged ends (see below). This implies that the
stress values found in an isometric muscle contraction
reflect properties of a somewhat shortening central
part of the muscle. Such an internal shortening against
a series elasticity may tend to decrease the peak stress
value found for the muscle.
All arguments presented above indicate that it is
not easy to compare the force-generating capacity of
heart and muscle precisely. Nevertheless, we think
that we are on the safe side when expressing the
opinion that the "pressure" levels generated by the
isolated muscles are of the same order of magnitude
as those found in the intact heart.
The "pressure" wave forms presented in Figure 3
were compared with those presented in earlier studies
for left (Elzinga and Westerhof, 1973) and right (Elzinga et al., 1980) ventricles. The results suggest that,
apart from minor deviations (see Results) and the
differences in the contraction duration, the reaction
of the isolated trabeculae on the various "arterial
input impedances" studied is similar to that of the
intact heart. Because we have used the same "arterial
system" in heart and muscle studies, this statement
holds equally true for the "flow" patterns shown in
these two figures. However, the question remains to
be answered whether or not the mean output of the
2D pump is quantitatively comparble to what is found
for the intact heart.
A partial answer to this question can be obtained
by comparing the maximum ejection fraction of the
left ventricle with the corresponding quantity obtained for the muscle in the 2D model. For the isolated
dog heart, the smallest possible end-systolic volume
of the left ventricle can be estimated to be about 20%
of the end-diastolic volume (Suga et al., 1973; Suga
and Sagawa, 1974; Suga et al., 1979). We found for
the isolated trabeculae a maximum percentage
shortening of 21.4% (see Table 2). Suppose that this
figure is an underestimation because of the presence
of damaged ends of the isolated muscle and that we
have to use 30% instead (29% of the full muscle length
is now assumed to be dead). The smallest end-systolic
volume as calculated from Equation 2 is then 50%.
Modeling the left ventricle with a thin-walled sphere,
which is not very realistic regarding the prevailing
fiber direction and the fact that during the ejection
phase the apex base distance remains rather constant,
would reduce this value to 35%. This value is still
considerably higher than the 20% mentioned above.
Our conclusion that the force-generating capacity of
the isolated trabeculae is not less than that found
in the heart makes it unlikely that an explanation can
be found on the basis of the idea that the isolated
muscle may shorten much less than the muscle fibers
437
in the left ventricular wall. An explanation could be
provided by the hypothesis that with ejections at such
low pressures the endocardial part of the left ventricular wall is pushed inward passively by fibers located
in the more outer layers. The space occupied by
papillary muscles may be added to part of the ventricular volume that cannot be ejected. If such inhomogeneities occur in the left ventricular wall, it is clear
that the 2D model cannot be used as a reliable model
in this respect. Until this point of uncertainty has
been properly explained, we cannot compare quantitatively the output of the left ventricle with the
"output" of our 2D muscle pump.
Possible damaged ends of the isolated muscle
(Krueger et al., 1975; Huntsman et al., 1977; Donald
et al., 1980) cannot be excluded. However, the isometric forces generated are found to be at least as
high as those found in the wall of the left ventricle at
the level of the base in the circumferential direction
(see above). Moreover, it should be realized that the
isovolumic contraction of the left ventricle is not
isometric with respect to the muscle. Not all muscles
depolarize synchronously, so some shorten at the
expense of others, and the aortic and mitral valves
may bulge. Therefore, even control of sarcomere
length in the center section of the muscle would not
make the contraction representative of the muscle in
the ventricular wall.
Comparison of Pump Function Graphs Determined
in Heart and Isolated Muscle
From the "pump function" graphs presented in
Figures 4 and 5 it was concluded that in the muscle
experiments this graph showed a slight S-shape. This
is apparently in contrast to what we have reported for
the intact left and right ventricle. However, scrutinizing in retrospect the cardiac pump function graphs
presented in the past, we could not always exclude
the existence of an S-shape there either. To demonstrate this, we have replotted left ventricular pump
function graphs from Elzinga et al. (1980). The data,
presented in Figure 6, are precisely the same as those
presented in the study quoted above, but now the
lines through the points have been drawn in a different manner. In four of the five experiments, an Sshape of the left ventricular pump function graph
cannot be excluded. We could not apply this reconsideration to the right ventricle because sufficiently
low pressure values were not available to provide an
S-shape. We conclude from this that the shape of the
pump function graph obtained in cardiac and muscle
studies is similar.
From Figure 4, it can also be concluded that the
"pump function" graphs obtained from the muscles
were little sensitive for the nature of the load. The
points obtained in different ways (steady state load or
beat-to-beat "pressure" changes, fixed "pressure"
levels, or simulated "arterial input impedances") deviated only slightly from a common path. This is in
accordance with our findings for the intact left and
Circulation Research/ Vol. 51, No. 4, October 1982
438
right ventricle (Elzinga and Westerhof, 1979; Elzinga
et al., 1980).
Address
Physiology,
Amsterdam,
Received
for reprints: Dr. N. Westerhof, The Laboratory for
Free University, Van der Boechorststraat 7, 1081 BT
The Netherlands.
June 15, 1981; Accepted for publication June 24, 1982.
References
Downloaded from http://circres.ahajournals.org/ by guest on June 14, 2017
Brutsaert DL, Paulus WJ (1977) Loading and performance of the
heart as muscle and pump. Cardiovasc Res 11:1-16
Burns JW, Covell JW, Myers R, Ross J (1971) Comparison of
directly measured left ventricular wall stress and stress calculated
from geometric reference figures. Circ Res 28: 611-621
Donald TC, Reeves DN, Reeves RC, Walker AA, Hefner LL (1980)
Effect of damaged ends in papillary muscle preparations. Am J
Physiol 238: H14-H23
Elzinga G, Westerhof N (1973) Pressures and flow generated by
the left ventricle against different impedances. Circ Res 32: 178186
Elzinga G, Westerhof N (1978) The effect of an increase in inotropic
state and end-diastolic volume on the pumping ability of the
feline left heart. Circ Res 42: 620-628
Elzinga G, Westerhof N (1979) How to quantify pump function of
the heart. The value of variables derived from measurements on
isolated muscle. Circ Res 44: 303-308
Elzinga G, Westerhof N (1980) Pump function of the feline left
heart; changes with heart rate and its bearing to the energy
balance. Cardiovasc Res 14: 81-92
Elzinga G, Westerhof N (1981) "Pressure-volume" relations in
isolated cat trabeculae. Circ Res 49: 388-394
Elzinga G, Noble MIM, Stubbs J (1977) The effect of an increase in
aortic pressure upon the inotropic state of cat and dog left
ventricles. J Physiol (Lond) 273: 597-615
Elzinga G, Piene H, De Jong JP (1980) Left and right ventricular
pump function and consequences of having two pumps in one
heart. Circ Res 46: 564-574
Gabe IT (1974) Starling's law of the heart and the geometry of the
ventricle. Ciba Found Symp 24: 193-208
Gibbs CL (1978) Cardiac energetics. Physiol Rev 58: 174-254
Hill AV (1965) Trails and Trials in Physiology. London, Edward
Arnold Ltd, pp 208-241
Huisman RM, Elzinga G, Westerhof N, Sipkema P (1980) Mea-
surement of left ventricular wall stress. Cardiovasc Res 14: 142153
Huntsman LL, Day SR, Stewart DK (1977) Non uniform contraction
in the isolated cat papillary muscle. Am J Physiol 233: H613H616
Jewell BR, Rovell JM (1973) Influence of previous mechanical
events on the contractility of isolated cat papillary muscle. J
Physiol (Lond) 235: 715-740
Krueger JW, Pollack GH (1975) Myocardial sarcomere dynamics
during isometric contraction. J Physiol (Lond) 251: 627-643
Parmley WW, Brutsaert DL, Sonnenblick EH (1969) Effects of
altered loading on contractile events in isolated cat papillary
muscle. Circ Res 24: 521-532
Paulus WJ, Claes VA, Brutsaert DL (1979) Physiological loading of
isolated feline cardiac muscle. The interaction between muscle
contraction and vascular impedance in the production of pressure
and flow waves. Circ Res 44: 491-497
Puls HW, Elzinga G (1978) An analogue device for the measurement of cardiovascular variables. Cardiovasc Res 12: 316-321
Streeter DD, Spotnitz SMHM, Patel DP, Ross J, Sonnenblick EH
(1969) Fiber orientation in the canine left ventricle during diastole
and systole. Circ Res 24: 339-347
Suga H, Sagawa K (1974) Instantaneous pressure-volume relationship and their ratio of the excised and supported canine left
ventricle. Circ Res 35: 117-126
Suga H, Sagawa K, Shoukas AA (1973) Load independence of the
instantaneous pressure-volume ratio of the canine left ventricle
and effects of epinephrine and heart rate on the ratio. Circ Res
32: 314-322
Suga H, Kitabatake A, Sagawa K (1979) End-systolic pressure
determines stroke volume from fixed end-diastolic volume in the
isolated canine left ventricle under a constant contractile state.
Circ Res 44: 238-249
Sulman DL, Bing AHL, Mark RG, Burns SK (1974) Physiologic
loading of isolated heart muscle. Biochem Biophys Res Commun
56: 947-951
Westerhof N, Elzinga G (1978) The apparent source resistance of
heart and muscle. Ann Biomed Eng 6: 16-32
Westerhof N, Elzinga G, Sipkema P (1971) An artificial arterial
system for pumping hearts. J AppI Physiol 31: 776-781
Wiegner AW, Bing OHL (1977) Altered performance of rat cardiac
muscle follows changes in mechanical stress during relaxation.
Circ Res 41: 691-693
Wiegner AW, Bing OHL (1978) Isometric relaxation of rat myocardium at end-systolic fiber length. Circ Res 43: 865-869
INDEX TERMS: Pump function • Muscle and pump arterial
impedance • Wall stress • Cat trabecula
Isolated cat trabeculae in a simulated feline heart and arterial system. Contractile basis of
cardiac pump function.
G Elzinga and N Westerhof
Downloaded from http://circres.ahajournals.org/ by guest on June 14, 2017
Circ Res. 1982;51:430-438
doi: 10.1161/01.RES.51.4.430
Circulation Research is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231
Copyright © 1982 American Heart Association, Inc. All rights reserved.
Print ISSN: 0009-7330. Online ISSN: 1524-4571
The online version of this article, along with updated information and services, is located on the
World Wide Web at:
http://circres.ahajournals.org/content/51/4/430
Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in
Circulation Research can be obtained via RightsLink, a service of the Copyright Clearance Center, not the
Editorial Office. Once the online version of the published article for which permission is being requested is
located, click Request Permissions in the middle column of the Web page under Services. Further information
about this process is available in the Permissions and Rights Question and Answer document.
Reprints: Information about reprints can be found online at:
http://www.lww.com/reprints
Subscriptions: Information about subscribing to Circulation Research is online at:
http://circres.ahajournals.org//subscriptions/