Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
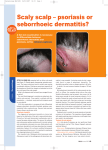
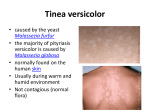
Derm Oct-AH/NH/SON* 9/10/06 11:43 Page 1 Forum Dermatology Optimal management of seborrhoeic dermatitis Approximately 3%-5% of the population suffers from seborrhoeic dermatitis which is a chronic, relapsing condition, writes Bernadette O’Leary Figure 1. Red, scaly rash of seborrhoeic dermatitis in a typical facial distribution Table 1 DERMATITIS MEANS SKIN INFLAMMATION and seborrhoea means sebum. Seborrhoeic dermatitis (SD), as the name hints, means inflammation of the sebum or oily-rich areas of the skin, that is, areas rich in sebaceous glands. But as sebum isn’t known to cause inflammation, several other theories have been postulated for the aetiology of SD such as hormonal levels, CNS causes and the overgrowth of a yeast. The possible hormonal links are raised because of the appearance of the condition in infancy (secondary to maternal hormones) and also because of its post-puberty appearance (higher androgen levels starting to circulate). A link with the CNS and some possible neurogenic deficiency has been proposed because of its association with Parkinson’s disease and other neurologic disorders including post CVA, epilepsy and facial nerve palsy. A more causal link seems to exist between SD and the proliferation of the Malassezia species, ie. Malassezia furfur and Malassezia ovalis because of the ability to isolate it in patients with SD and by the therapeutic response of seborrhoeic dermatitis to antifungal agents. This species lives on the sebaceous gland-rich areas (head, upper back and chest) of most people’s skin, needing oil to survive. Its overgrowth in patients with SD is felt to cause irritation of the skin, either directly or through the secretion of a toxin triggering the inflammatory cascade causing hyperproliferation, scaling and erythema of the skin. It is not contagious and is not the same yeast that is present in food products, so dietary exclusion of yeast foods hasn’t been found to be of help. Classification Males are affected more than females in all age groups. SD is seen frequently in patients with Parkinson’s disease, perhaps due to neurotransmitter abnormalities resulting in increased sebum production. Levodopa decreases sebum production, so SD usually improves in these patients when commenced on it. HIV may first present in patients with a generalised SD rash. This is felt to be secondary to their reduced immunity, Differential diagnosis Scalp Psoriasis Atopic eczema Contact allergic dermatitis Pityriasis amantacia Tinea capitis Flexures Psoriasis Intertrigo Candidiasis Erythrasma Ear Psoriasis Atopic eczema Sebo-psoriasis Contact dermatitis Face Rosacea Psoriasis Eczema Impetigo Body Pityriasis rosea Pityriasis versicolor Psoriasis resulting in overgrowth of the yeast. Many patients give a positive family history of dandruff, SD or psoriasis even though it is not felt to be hereditary. Exacerbations usually occur in the winter as UV light inhibits the malassezia species. Drugs (eg. cimetidine and neuroleptics) and stress can also cause exacerbations. Distribution Seborrhoeic dermatitis can affect the scalp; face; nasolabial folds, eyebrows, external ears, eye-lashes, glabella, beard area, axillae, umbilicus, groin and inframammary area. It can frequently become apparent when men grow moustaches or beards and disappear once the facial hair is removed. FORUM October 2006 55 Derm Oct-AH/NH/SON* 9/10/06 11:43 Page 2 Forum Dermatology Table 2 Treatment of adult SD • Frequent washing Anti-fungals • 2% Ketoconazole shampoo/cream (Nizoral) Thrice wkly • Selenium sulphide shampoo (Selsun) Twice wkly • Zinc pyrithione shampoo (Head and Shoulders) Thrice wkly • Tar shampoos (capasal, T Gel, Exorex) Thrice wkly Anti-Inflammatory (immunomodulatory) agents • Steroid shampoo, eg. Bettamouse Twice wkly • Topical steroids with antifungal ointments/creams eg. Daktacort, Canesten HC Daily • Lithium succinate ointment (Efalith) Daily • Topical calcineurin inhibitors -eg. tacrolimus ointment (Protopic) Daily Keralolytics • 3%-5% salicylic acid shampoo Twice wkly • Tar with anti-fungal shampoo Thrice wkly • Zinc pyrithione shampoo-also antifungal Twice wkly • Warm olive oil washed out 4 hrs later with tar shampoo Thrice wkly Anti-androgens (females) • Dianette, Yasmin, Spironolactone Daily Others treatment for refractory Ds • Roaccutane • Oral ketoconazole 200mg od x 14 days • Oral itraconazole 100mg od < 21 days • UVB therapy Wkly Alternative medication • Tea tree oil shampoo Daily • Vinegar Daily Clinical appearance For mild scalp scaling, the term ‘dandruff’ is used. When the inflammatory cascade increases with scaling plus erythema arising in certain locations in the body, the term seborrhoeic dermatitis is used. Adult SD usually commences with a mild greasy scaling of the scalp, with scaling and erythema of the nasolabial folds or post auricular skin. In Afro-Caribbean skin, the diagnosis is more difficult. The scaling is prominent but the erythema may be masked by the darker skin. Sometimes, post inflammatory hypopigmentation is seen after treating these patients. Two types of SD may appear on the chest – a common petaloid type – named after its resemblance to flower petals, and a rarer pityriasiform type which resembles pityriasis rosea. For some patients, chronic otitis externa may be the only manifestation. However, another possible manifestation is blepharitis with eyelid crusts and scale, sometimes resulting in meibomian gland occlusion and abscess formation. Seborrhoeic dermatitis is usually diagnosed clinically by its appearance and distribution but if doubt arises a skin biopsy may distinguish it from similar disorders, eg. SD on the scalp margin can be difficult to distinguish with psoriasis, hence the term applied – ‘sebopsoriasis’. Good hygiene For the patient who normally shampoos just once a week, increasing this to daily or alternative day shampooing may be enough to clear mild dandruff and erythema. Similarly for the face, daily cleansing with a mild soap and water may be enough if they were not doing this previously. It is impor56 FORUM October 2006 tant to note though that skin affected by SD is more sensitive than normal skin so if the mild soap irritates, a fragrance-free cleanser, eg. Emulave, or Alveeno range of cleansers may be tried. If the skin is extremely dry and sensitive, water alone should be used. To aid in deciding whether ingredients in cleansers, cosmetics or moisturisers may be potentially irritating, check www.zerozits.com/Articles/acnedetect.htm – this webpage lists skin-irritating ingredients in moisturisers (scroll down the page for the list). Medicated cream or ointment can replace the need for a moisturiser. For men, electric razors can provide a less irritating shave than razor blades. If a wet shave is preferred, shaving products need to be chosen very carefully as they may irritate the skin. In general, shaving gels or oils seem to be less irritating than shaving creams. If regular washing isn’t clearing the SD, then the addition of an antifungal agent may help. Anti-fungal treatment Using 2% ketoconazole kills the Malassezia yeast. It is also more cosmetically acceptable than tar shampoos, which can have a distasteful smell. Selenium sulphide has been found to have similar efficacy as 2% ketoconazole when compared but can cause scalp burning, lightening of hair colour and an orange staining of the scalp.1 In 1994 Faegemann found the use of topical ketoconazole to be superior over other imidazoles at decreasing Malassezia.2 Two separate studies have shown 2% ketoconazole cream to be as effective as steroid creams four Derm Oct-AH/NH/SON* 9/10/06 11:43 Page 3 Forum Dermatology Table 3 Treatment of infantile SD Scalp • Olive oil rubbed into the scalp followed by brushing with soft brush • Frequent shampooing with 1:10 dilution Johnson’s baby shampoo • 0.5%-1% hydrocortisone cream • 2nd line – 2% ketoconazole Body • Daily bath with oil/emulsifying ointment • Emollients • 1% hydrocortisone • 2% ketoconazole cream bd < 2 weeks weeks post-treatment and often resulting in more prolonged remissions without the risk of skin atrophy/telangiectasia.3,4 However, skin creams may need to be used initially with ketoconazole creams as approximately 10% of people report skin irritation with it. In 1999 Bulmer et al compared 2% ketoconazole with zinc pyrithione (Head and Shoulders) and found ketoconazole to be 100 times more effective at clearing SD.5 Also, the recurrence rate was significantly lower with ketoconazole. Ketoconazole can be drying on the hair so a conditioner may be used after it has been left on the scalp for three to five minutes before rinsing off. Due to the thick hair type of most Afro-Caribbeans, leave the 2% ketoconazole on the scalp (not hair) for 15-20 minutes. Anti-inflamatory treatment Steroid treatments are better not used long-term because of their side-effects and patient dependence. Oral steroids are occasionally used short-term in severe attacks or resistant cases. Topical tacrolimus (Protopic) ointment has fungicidal and anti-inflammatory properties without the risk of cutaneous atropy. Clinical improvement occurs after one week of use. Sun-screens must be used with it and the skin must be devoid of infection. Long-term studies are awaited on this product. An alternative anti-inflammatory treatment to steroids is Efalith. This cream contains lithium succinate and zinc. However, it is quite expensive. It is usually reserved for second-line treatment as it can cause skin irritation. Descaling agents (keratolytics) Removing scale first will allow topical treatment to act better on the skin. Refractory disease Roaccutane may be used to decrease sebaceous gland activity and thus reduce sebum production. It also has antiinflammatory properties. It is used in resistant cases. Lower doses to that used to treat acne are used and also a quicker response is seen, usually by four weeks. The dose is 0.1mg/kg-0.3mg/kg as opposed to 0.5mg/kg-1mg/kg used in acne. Contraception is essential for one month before its use and for three months post its discontinuation. Alternative medicine Tea tree oil is an essential oil and found to have fungicide activity, especially against Malassezia species.6 The therapy appears to have some effect and is well tolerated when used daily as a 5% shampoo.6 Vinegar Some anecdotal evidence suggests that vinegar applied topically can improve SD. It is believed to act as an antifungal agent via its acidic properties thus hindering the yeast’s ability to colonise the skin. Supposedly, the Malassezia species doesn’t thrive well in acidic environments. Antiandrogens, eg. cyproterone acetate (Dianette), drospirone (Yasmin), and spironolactone may be useful in women when oily skin is believed to contribute to SD. Infantile SD Rare and different to adult SD, this usually occurs from three months onwards, peaks at six months and is gone by one year. It usually presents with thick, yellow, greasy scales adherent to the scalp. The groins may also become affected with erythema and scale which involves the flexures. The axillae may also be similarly affected. In severe cases the entire body may be affected but this is uncommon in healthy children. Treatment options are outlined in Table 3. Those infants with generalised SD should be evaluated for immunodeficiency as immunocompromised children can get this. They may also have concomitant diarrhoea and failure to thrive (Leiner’s syndrome). Bernadette O’Leary is in practice in Co Waterford References on request